SHORT COMMUNICATION
Vogt-Koyanagi-Harada Syndrome Following COVID-19 mRNA Vaccination: Th2 to Th1 Transition-related Molecular Machinery
Yasuaki IKUNO, Akihiko YAMAGUCHI, Toshifumi TAKAHASHI and Noriki FUJIMOTO
Department of Dermatology, Shiga University of Medical Science, Setatsukinowa, Otsu, Shiga 520-2192, Japan. E-mail: ymgch@belle.shiga-med.ac.jp
Citation: Acta Derm Venereol 2024; 104: adv21502. DOI https://doi.org/10.2340/actadv.v104.21502.
Copyright: © 2024 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Oct 11, 2023; Accepted: Jan 16, 2024; Published: May 13, 2024
INTRODUCTION
Vogt-Koyanagi-Harada (VKH) syndrome is a multisystem disorder presenting with ophthalmological, neurological, and dermatological symptoms (1). There are > 20 case reports of SARS-CoV-2 (COVID-19) vaccine-associated VKH syndrome (2). However, no report has described details of dermatological features. We report here a case of COVID-19 vaccine-associated VKH syndrome with vitiligo and annular erythema with ophthalmological or neurological symptoms. Immunohistochemical staining revealed Th2 to Th1 transition with progression of vitiligo. Despite well-known Th1-skewed immunity in idiopathic VKH syndrome and vitiligo vulgaris, this transition has not been reported previously. We conclude that the transition is the aetiological and clinical feature of refractory vitiligo in vaccine-induced VKH syndrome.
CASE REPORT
A 58-year-old Japanese man noticed blurred vision 1 week after the second dose of COVID-19 mRNA vaccination (BNT162b2, Pfizer, Tokyo, Japan) in 2021. Three months later, he noticed headache, nausea, and vertigo. He visited a neurosurgeon, and magnetic resonance imaging (MRI) scans of head showed no abnormality. Due to the exacerbation of blurred vision and appearance of tinnitus, he visited an ophthalmologist and was diagnosed with iritis and uveitis. He was suspected to have Vogt-Koyanagi-Harada (VKH) syndrome and was followed up with no treatment. He reported leukoderma on his head and was referred to our hospital 9 months after his second vaccination.
He presented with depigmentation on his bilateral forehead and forearm in multiple coalescing patches, and annular erythema on bilateral upper arms (Fig. 1a–c). He had a past history of pompholyx and atopic dermatitis. No laboratory abnormalities were observed, except for the elevated serum levels of immunoglobulin E (IgE) (1,561 IU/mL) and thymus and activation-regulated chemokine (TARC) (1,050 pg/mL). Serum thyroid-stimulating hormone, free T3 and free T4 were all within normal limits. Autoantibodies, including antinuclear antibody, anti-SS-A and anti-SS-B antibody, were all negative. Histopathological examination and immunohistochemical staining of biopsy specimens from depigmentation and annular erythema at first visit showed interface dermatitis without spongiosis in the epidermis, and diminished SOX10 + and Melan-A + melanocytes in the epidermis and melanophages in the superficial dermis (Fig. 1d–f).
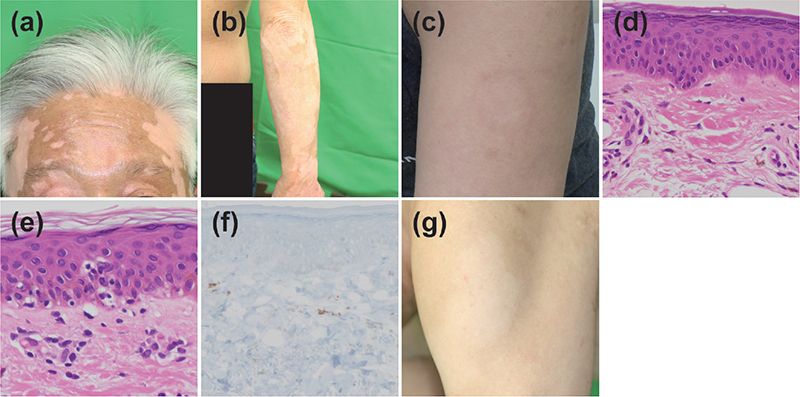
Fig. 1. Clinical course. The patient presented with depigmentation on: (a) his bilateral forehead; and (b) his bilateral forearm, in multiple coalescing patches. (c) Annular erythema on his bilateral upper arms. Histopathological examination of biopsy specimens from (d) depigmentation and (e) annular erythema revealed decreased melanocytes in the epidermis and melanophages in the superficial dermis (haematoxylin and eosin staining; original magnification (d) ×100 and (e) ×200). (f) Immunohistochemical staining of Melan-A revealed a decrease in melanocytes in the epidermis (original magnification ×100). (g) The annular erythema on bilateral upper arm became depigmented after 3 months of treatment.
The patient was diagnosed with VKH syndrome after vaccination. He was treated with topical vitamin D for 3 months; however, the annular erythema on bilateral upper arm became depigmented (Fig. 1g) and the depigmentation area was still increasing. He was treated with topical glucocorticoids and 10 mg/day prednisolone for 3 months. Subsequently, he was treated only with topical glucocorticoids, and the pigmentation area had been stable for 6 months.
Immunohistochemical staining for the lymphocytic profile of specimens at the first visit, from the depigmented lesion and annular erythema, which subsequently changed to depigmented lesion, revealed that infiltrated lymphocytes were predominantly CD4 + helper T-cells (Fig. 2a). There was no difference between the number of T-bet-positive Th1 cells and that of GATA-3-positive Th2 cells in annular erythema. In contrast, Th1 cells dominantly infiltrated compared with Th2 cells in depigmented lesion (Fig. 2b).
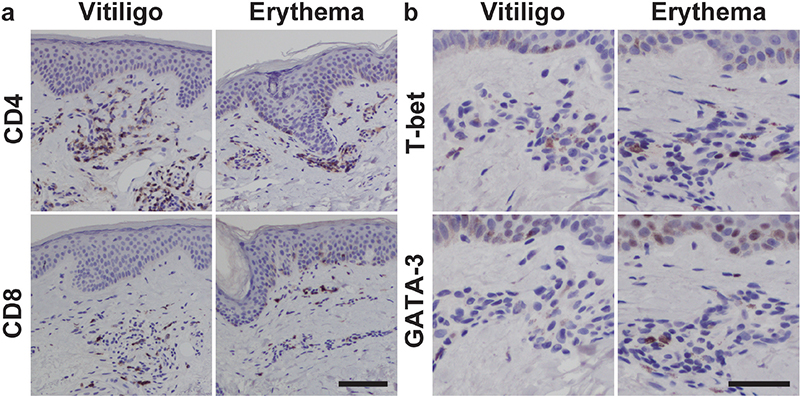
Fig. 2. Immunohistochemistry for lymphocytic profile. (a) Immunohistochemical staining of CD4 and CD8 in the specimens from depigmented lesion (vitiligo), and annular erythema in the pathogenic process, which subsequently changed to depigmented lesion (erythema) (original magnification ×100, scale bar = 100 µm). (b) Immunohistochemical staining of T-bet and GATA-3 in the specimens from depigmented lesion (vitiligo), and annular erythema in pathogenic process, which subsequently changed to depigmented lesion (erythema) (original magnification ×200, scale bar = 50 µm).
DISCUSSION
VKH syndrome is a multisystem disorder presenting with ophthalmological, neurological, and dermatological symptoms (1). VKH syndrome consists of 4 clinical stages: prodromal, acute, chronic convalescent, and chronic recurrent. Approximately 30% of patients with VKH syndrome present with dermatological symptoms, and dermatological features are often prominent in the chronic convalescent stage (3). VKH syndrome is usually diagnosed by an ophthalmologist at the acute stage.
There have been > 20 case reports of COVID-19 vaccine-associated VKH syndrome since 2021 (2). Probably because they were diagnosed by the ophthalmological approach, no report described details of dermatological symptoms, except for 1 case of VKH syndrome with poliosis diagnosed only by the ophthalmological approach (4). To our knowledge, this is the first case in which VKH syndrome after COVID-19 vaccination was suspected and diagnosed via the ophthalmological and dermatological approach. Depigmented patches were disseminated on the head, face, and trunk in VKH syndrome and COVID-19 vaccine-associated vitiligo (5); therefore, they were not distinguishable only by the dermatological course.
It has been shown previously that COVID-19 vaccine-associated VKH syndrome usually shows similar ophthalmological course as idiopathic VKH syndrome (2); however, it is unclear regarding the dermatological features in COVID-19 vaccine-associated VKH syndrome. In the current case, vitiligo developed 9 months after the first ophthalmological symptoms, compared with dermatological findings of idiopathic VKH syndrome, which usually appear approximately 3–4 months after onset. COVID-19 vaccine-associated VKH syndrome would show late ophthalmological and dermatological time-courses compared with idiopathic VKH syndrome.
VKH syndrome is an autoimmune inflammatory condition mediated by CD4+ T cells targeting melanocytes in multiple organs (6, 7). In skin, histological features of idiopathic VKH syndrome-associated vitiligo involve the presence of infiltration of helper T cells and macrophages containing melanin granules (8). However, there is only 1 case report in which skin immunohistochemical findings of lymphocytes were assessed (9). This report showed that infiltrating lymphocytes were composed mainly of CD4-positive T cells, as in the current case (9).
In vitiligo vulgaris, CD8-positive cytotoxic T cells, using cytotoxic mediators, such as granzyme B and Fas ligand (FasL), are predominantly infiltrated cells involved in pathogenesis by killing of melanocytes (10). Therefore, the pathogenic mechanism of vaccine-induced and idiopathic VKH syndrome, in which CD4-positive T cells predominantly infiltrates, may differ from that of vitiligo vulgaris. CD4-positive T cells are reported to be involved in melanocyte loss by destroying MHC class II expressing cells via Fas–FasL interaction in vitiligo vulgaris, and may play a critical role in melanocyte loss in vaccine-induced and idiopathic VKH syndrome by the similar mechanism.
In the current case, pathological examination of the specimen from annular erythema revealed not eczematous dermatitis but interface dermatitis (Fig. 1e), and comorbid atopic dermatitis was well controlled except for pompholyx and eczematous lesions in the hands and feet, despite high serum TARC. There are some reports of prodromal erythema before vaccine-related vitiligo (11) and idiopathic VKH syndrome with incomplete vitiligo called “inflammatory vitiligo” (12); therefore, annular erythema was considered as the lesion in the pathogenic process which subsequently changed to depigmented lesion. The current study compared the profiles of infiltrating lymphocytes between depigmented lesion considered as the complete vitiligo, and annular erythema considered as the pathogenic process before complete vitiligo by immunohistochemistry. It is notable that the results of immunohistochemistry suggest that both Th1 and Th2 cells contribute mainly to the pathogenesis at the beginning of vitiligo in VKH syndrome, and that Th1 cells gradually become dominant with progression of vitiligo.
Because Th1-dominant immunity in idiopathic VKH syndrome (6) and vitiligo vulgaris (13) is common and well-known, the Th2 reaction in the current case is unusual. Considering that prodromal erythema is rare in vaccine-related vitiligo (11) and idiopathic VKH syndrome (12), atypical Th2 immunity would contribute to the characteristic prodromal erythema in the current case. Indeed, the study of vaccination (BNT162b2) in current use revealed some Th2-skewed immune response as well as well-known Th1-skewed immune response (14); therefore, vaccine-induced atypical deleterious Th2 immunity overlapping with normal Th1 immunity may contribute to the pathogenesis of prodromal erythema. Also, Th2 to Th1 transition was reported to be required for the maintenance and potentiating of skin inflammation by the in vivo analysis of cutaneous lupus erythematosus model mice (15); therefore, Th2 to Th1 transition may contribute to refractory vitiligo in the current case. Considering the consistent Th1-skewed response in idiopathic VKH syndrome, the fundamentals of aetiological and clinical features in the current case could be considered to be due to Th2-modified idiopathic VKH syndrome.
In conclusion, Th2-skewed prodromal erythema and Th2 to Th1 transition are the aetiological and clinical features in vaccine-induced VKH syndrome. Further investigations are needed to elucidate the precise feature of vaccine-induced VKH syndrome.
REFERENCES
- Damico FM, Kiss S, Young LH. Vogt-Koyanagi-Harada disease. Semin Ophthalmol 2005; 20: 183–190.
- Xu K, Gao B, Li J, Xiang Y, Cao L, Zhao M. Clinical features, diagnosis, and management of COVID-19 vaccine-associated Vogt-Koyanagi-Harada disease. Hum Vaccin Immunother 2023; 19: 2220630.
- Lim JA, Tan WC, Nor NM. Hints from the skin beneath: vitiligo in Vogt–Koyanagi–Harada disease. Dermatol Sin 2022; 40: 78–84.
- De Domingo B, López M, Lopez-Valladares M, Ortegon-Aguilar E, Sopeña-Perez-Argüelles B, Gonzalez F. Vogt-Koyanagi-Harada disease exacerbation associated with COVID-19 vaccine. Cells 2022; 11: 1012.
- Tsai T-F, Ng CY. COVID-19 vaccine–associated vitiligo: a cross-sectional study in a tertiary referral center and systematic review. J Dermatol 2023; 50: 982–989.
- Norose K, Yano A. Melanoma specific Th1 cytotoxic T lymphocyte lines in Vogt-Koyanagi-Harada disease. Br J Ophthalmol 1996; 80: 1002–1008.
- Sugita S, Sagawa K, Mochizuki M, Shichijo S, Itoh K. Melanocyte lysis by cytotoxic T lymphocytes recognizing the MART-1 melanoma antigen in HLA-A2 patients with Vogt– Koyanagi–Harada disease. Int Immunol 1996: 8: 799–803.
- Lavezzo MM, Sakata VM, Morita C, Rodriguez EE, Abdallah SF, da Silva FT, et al. Vogt-Koyanagi-Harada disease: review of a rare autoimmune disease targeting antigens of melanocytes. Orphanet J Rare Dis 2016; 11: 29.
- Okada T, Sakamoto T, Ishibashi T, Inomata H. Vitiligo in Vogt-Koyanagi-Harada disease: immunohistological analysis of inflammatory site. Graefes Arch Clin Exp Ophthalmol 1996; 234: 359–363.
- Chen J, Li S, Li C. Mechanisms of melanocyte death in vitiligo. Med Res Rev 2021; 41: 1138–1166.
- Mancha D, Antunes J, Soares-de-Almeida L, Borges-Costa J, Filipe P. Localized vitiligo and post-inflammatory hypopigmentation at the injection site of a COVID-19 mRNA vaccine. Dermatol Pract Concept 2023; 13: e2023023.
- Tsuruta D, Hamada T, Teramae H, Mito H, Ishii M. Inflammatory vitiligo in Vogt-Koyanagi-Harada disease. J Am Acad Dermatol 2001; 44: 129–131.
- Speeckaert R, Belpaire A, Speeckaert MM, van Geel N. A meta-analysis of chemokines in vitiligo: recruiting immune cells towards melanocytes. Front Immunol 2023; 14: 1112811.
- Bigenwald C, Haddad Y, Thelemaque C, Carrier A, Birebent R, Ly P, et al. RBD- specific Th1 responses are associated with vaccine-induced protection against SARS-CoV-2 infection in patients with hematological malignancies. Oncoimmunology 2023; 12: 2163785.
- Haddadi NS, Mande P, Brodeur TY, Hao K, Ryan GE, Moses S, et al. Th2 to Th1 transition is required for induction of skin lesions in an inducible and recurrent murine model of cutaneous lupus-like inflammation. Front Immunol 2022; 13: 883375.