ORIGINAL REPORT
Based on Immune Microenvironment and Genomic Status, Exploring Immunotherapy in Advanced Hidradenocarcinoma: A Retrospective Analysis
Jing LIN1,2#, Li ZHU3#, Yanping CHEN4#, Qian LI3#, Zhiheng KE3, Huishan ZHANG1,2, Yufang HUANG1,2, Jianping LU4 and Yu CHEN1,2
1Department of Medical Oncology, 2Cancer Bio-Immunotherapy Center and 4Department of Pathology, Clinical Oncology School of Fujian Medical University, Fujian Cancer Hospital, and 3Clinical Oncology School of Fujian Medical University, Fuzhou, Fujian Province, China
#These authors contributed equally.
There are no standard treatment guidelines for hidradenocarcinoma, and the immune microenvironment and genomic data are very limited. Thus, in this study the immune microenvironment and genomic indicators in hidradenocarcinoma was investigated, and immunotherapy for hidradenocarcinoma was initially explored. Forty-seven hidradenocarcinoma patients were retrospectively collected. Immunohistochemical staining was performed to identify CD3/CD8+ T cells and programmed death ligand-1 expression. In total, 89.4% and 10.6% of samples had Immunoscores of 0–25% and 25–70%. Tumour proportion score distribution was as follows: tumour proportion score < 1% in 72.4%, 1–5% in 17.0%, and > 5% in 10.6%. Combined positive score distribution was as follows: combined positive score < 1 in 63.8%, 1–5 in 14.9%, and > 5 in 21.3%. Next-generation sequencing revealed that TP53 (33%), PI3KCA (22%), and ERBB3 (22%) were the most frequently mutated genes. The PI3K-Akt signalling pathway, growth, and MAPK signalling pathways were significantly enriched. Five patients had a low TMB (< 10 muts/Mb), and 9 patients had MSS. Three patients treated with immune combined with chemotherapy achieved significant tumour regression, and the progression-free survival was 28.8 months. In conclusion, the hidradenocarcinoma immune microenvironment tends to be noninflammatory. Evidence-based targets for targeted therapy are lacking. Immunotherapy combined with chemotherapy may be better for most advanced hidradenocarcinoma patients with a noninflammatory microenvironment.
Key words: hidradenocarcinoma; NGS; PD-1 inhibitor; immunotherapy; immune microenvironment.
SIGNIFICANCE
Capsule summary
- It was found that the immune microenvironment of hidradenocarcinoma was noninflammatory and evidence-based targets for targeted therapy were lacking.
- New ideas and strategies for the use of immunosuppressive agents in advanced hidradenocarcinoma are suggested.
Citation: Acta Derm Venereol 2024; 104: adv22146. DOI https://doi.org/10.2340/actadv.v104.22146.
Copyright: © 2024 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Oct 11, 2023; Accepted: Apr 11, 2024; Published: May 13, 2024
Corr: Yu Chen, Department of Medical Oncology, Clinical Oncology School of Fujian Medical University, Fujian Cancer Hospital, Fuzhou 350000, Fujian Province, China. E-mail: chenyu1980@fjmu.edu.cn
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Hidradenocarcinoma is a rare malignant neoplasm originating from the dermis and accessory sweat gland tissue of the skin, accounting for approximately 7.6% of skin adnexal tumours (1). Histopathologically, hidradenocarcinomas present with 2 different cell types: 1 type is dark-coloured spindle cells with eosinophilic cytoplasm arranged around their periphery, the other is a large, atypical, hyperplastic, clear cell that has polymorphonuclear nuclei and stains high with the Periodic acid–Schiff stain (PAS) (2). Patients with early stage hidradenocarcinoma are usually treated with wide local excision or Mohs micrographic surgery (3). There have been a few reports of a patient with metastatic hidradenocarcinoma who achieved a partial response and a decrease in the size of the cutaneous metastases after treatment with first-line 5-fluouracil therapy and doxorubim in combination with platine as second-line therapy (4). However, there are no consistent treatment guidelines for advanced patients. Therefore, there is an urgent requirement to make progress in the treatment of advanced hidradenocarcinoma.
Programmed death 1 (PD-1) and programmed death ligand-1 (PD-L1) is an important immune checkpoint pathway with an immunosuppressive effect associated with malignant tumour cells (5). Currently, PD-1 inhibitors have been demonstrated to be effective for treating skin malignancies such as basal cell carcinoma (6) and melanoma (7). PD-1 inhibitors generally work well in patients with a high tumour mutation burden (TMB-H), high levels of microsatellite instability (MSI-H)/mismatch repair deficiency (dMMR), and high PD-L1 expression (8, 9). Large-scale research on PD-L1 and T cells in the microenvironment of hidradenocarcinoma is limited, and reports on patients with hidradenocarcinoma treated with PD-1 inhibitors are rare. Hence, it is necessary to explore the immunotherapy-related markers of patients with hidradenocarcinoma and the effectiveness of PD-1 inhibitor treatment in patients.
Data on the genetic basis of hidradenocarcinomas at the molecular level are still very limited. Two reports have shown additional activating mutations in the form of 17q LOH and APC, and PIK3CA mutations in hidradenocarcinomas. Much remains unknown about the genetic background of hidradenocarcinomas.
In this study, we retrospectively collected the clinical data of 47 hidradenocarcinoma patients with complete paraffin sections and evaluated the CD3+/CD8+ T cells and PD-L1 expression with immunohistochemical staining. In addition, we analysed the mutational spectrum of 9 patients by next-generation sequencing (NGS); we then discuss the prognosis of 3 patients who were treated with PD-1 inhibitors. Our study initially explored the efficacy and pattern of immunotherapy for advanced hidradenocarcinoma, based on tumour microenvironment and genetic background status.
MATERIALS AND METHODS
Patients
In this study, the medical record files of 47 patients diagnosed with hidradenocarcinoma from January 2012 to March 2022 were reviewed from Fujian Cancer Hospital. The clinical information included sex, age, clinical stage, gene results, detailed treatment history, and imaging evaluation. This study was approved by the ethics committee of the Fujian Medical University Cancer Hospital. A detailed treatment history of the 3 patients with hidradenocarcinoma treated with PD1 inhibitors in this study can be seen in Appendix S1.
Immunohistochemical assessment
All cases were carefully reviewed independently by 2 dermatopathologists to confirm the histological diagnosis following the criteria of the WHO Skin Tumour Classification (4th ed.). Immunohistochemical staining to identify CD3/CD8+ T cells and PDL1 (22C3) expression was performed on paraffin embedded tissues using a Dako Link 48 Autostainer. For each case, manual slide reading and review of the tumour invasive margin (IM) and tumour centre (TU) were performed independently by 2 pathologists with more than 10 years of experience. The IM is defined as a 1 mm area including tumour glands infiltrating healthy tissue. The TU is defined as the tumour mass and adjacent hidradenocarcinomas. The CD3+ T cells and CD8+ T cells were counted, and the percentage of CD3+ T cells or CD8+ T cells in total cells was calculated for each representative tumour region (IM and TU). The mean of 4 values (CD3+/IM, CD3+/TU, CD8+/IM, and CD8+/TU) was calculated to determine the Immunoscore (IS). The samples were grouped based on average percentage: 0–25%, > 25–70%, and > 70%. The samples were defined as having low (IS-low), medium (IS-int), or high (IS-high) Immunoscores (10) (Fig. 1).

Fig. 1. Representative images of programmed death ligand-1 (PD-L1) staining in hidradenoma carcinoma tumour cells and immune cells. Hidradenoma carcinoma samples with CPSs of 0 (A, B), 1 (C, D red arrow refers to immune cells), and 10 (E, F red arrow refers to immune cells, black arrow indicates the tumour cell) are shown at 20× and 200× magnification. Representative images of haematoxylin and eosin (H&E) stain in the IS-int tumour invasive margin (IM) (G, 200×) and tumour centre (TU) (H, 200×). Representative images of CD3 IS-int in IM (I) and TU (J) region are shown at 200× magnification. Representative images of CD8 IS-int in IM (K) and TU (L) region are shown at 200× magnification. Representative images of haematoxylin and eosin (H&E) stain in the IS-low tumour invasive margin (IM) (M, 200×) and tumour centre (TU) (N, 200×). Representative images of CD3 IS-low in IM (O) and TU (P) region are shown at 200× magnification. Representative images of CD8 IS-low in IM (Q) and TU (R) region are shown at 200× magnification.
PDL1 expression was measured in patients with hidradenocarcinoma. The PDL1 expression score was determined by the tumour proportion score (TPS) and combined positive score (CPS). TPS was defined as the percentage of tumour cells with partial or complete PD-L1 membrane staining (≥1+) in all live tumour cells (with negative or positive staining) present in the sample (11). CPS was calculated as the number of PD-L1-positive cells (tumour cells, lymphocytes, macrophages) divided by the total number of live tumour cells multiplied by 100 (12).
Statistical analysis
The R software “ComplexHeatmap” package and heatmap plots (R Foundation for Statistical Co,[uting, Vienna, Austria) were used to visualize somatic mutations and copy number variants (CNVs). Metascape (http://metascape.org) was used for enrichment analysis. Pathway and process enrichment analyses were carried out with the following ontology sources: GO biological process terms, KEGG pathways, Reactome gene sets, canonical pathways, and WikiPathways. Terms with a p-value < 0.01, a minimum count of 3, and an enrichment factor > 1.5 were collected and grouped into clusters based on their membership similarities. In addition, we performed protein–protein interaction (PPI) analysis and applied the Molecular Complex Detection (MCODE) algorithm to determine densely connected network components. Survival analysis was performed using Kaplan–Meier analyses with log rank test and categorical variables using a χ2 test. For stratification cut-point, the marker levels were classified as high/low using the top 50 percentile of the cohort in the study. Statistical significance was considered at p < 0.05 and analyses were performed using R software.
RESULTS
Baseline characteristics, immunoscore, and programmed death ligand-1 expression in hidradenocarcinoma
We analysed the clinical characteristics and of 47 patients with hidradenocarcinoma, summarized in Table I. The median age at diagnosis was 60.3 years (range 37 to 91 years), and the median survival was 63.7months (range 2 to 190.4 months). Of the 47 patients, 29 were male and 18 were female. Tumour stages in stages I, II, III, and IV were 19.2%, 29.8%, 10.6%, and 40.4%, respectively (according to the AJCC 8th ed.). The proportions of primary tumours in the head–face, trunk, limb, and genitalia were 31.9%, 19.1%, 34.1%, and 14.9%, respectively.
Immunohistochemical analysis was performed in 47 patients (Table II). In total, 42 (89.4%) patients had IS-low, 5 (10.6%) patients had IS-int, and none had IS-high, indicating a lower immune cell infiltration within the tumours. In addition, the PD-L1 TPS, 37 (72.3%) of tumours had no or very low PD-L1 expression (< 1%), only 8 (17.0%) of tumours had TPS = 1%–5%, and 5 (10.6%) of tumours had TPS > 5%. For the PD-L1 CPS, 63.8%, 14.9%, and 21.3% of patients in the entire cohort had CPS < 1, CPS = 1 to 5, and CPS > 5, respectively. The immunohistochemical results reported above suggest that hidradenocarcinoma is a comparative immune-desert phenotype tumour.
Gene mutation and signalling pathway enrichment results
As shown in Fig. 2, we evaluated 9 patients with hidradenocarcinoma. In the mutation analysis, 77 single nucleotide variants (SNVs) and 30 insertion/deletion mutations (indels) were identified. Among them, TP53 (33%), PI3KCA (22%), and ERBB3 (22%) were the mutated genes with a high variation frequency in somatic mutation (Fig. 2A). The OncoKB framework was used to categorize molecular alterations based on levels of actionability. Compared with all actionable alteration in all solid tumours, no level 1–3 actionable alterations were found in the 9 patients, and only 1 patient had a single level-4 alteration (in NF1). In addition, 5 patients had a low TMB (< 10muts/Mb), and there were 4 patients with TMB-H. All 9 patients had MSS tumours.
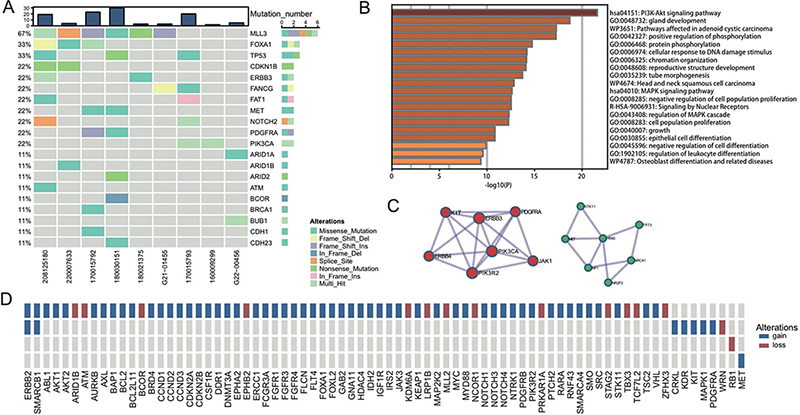
Fig. 2. Genomic features of hidradenocarcinoma. Somatic mutations in patients with hidradenocarcinoma. (A) The mutation count is shown above the heatmap, and different colours indicate different variation types. (B) All mutant genes were used for enrichment analysis, and the results are coloured by p-value. (C) 2 PPI MCODE components were identified with Metascape. (D) CNVs in patients with sweat gland carcinoma.
Analysis of CNVs identified 4 patients with detectable CNVs, and ERBB2 and SMARCB1 had a high frequency of variation (Fig. 2D). Functional enrichment analysis showed that the PI3K-Akt signalling pathway, growth pathways, and MAPK signalling pathway were significantly enriched in hidradenocarcinoma (Fig. 2B). The relevant PPIs among the mutated genes were extracted from a PPI data source, and a PPI network was generated. The MCODE algorithm was then applied to analyse this network. MCODE-based enrichment analysis was applied, and anti-EGFR resistance and the RAF/MAP kinase cascade were found to be significantly enriched (Fig. 2C), suggesting that patients with hidradenocarcinoma may be resistant to anti-EGFR therapy and may have sustained cell proliferation derived from different mechanisms.
Correlation of biomarker expression between survival and clinical features
As shown in Appendix S1 and Fig. S2, we conducted survival analysis stratified by the expression of CD3, CD8, and PD-L1. The median OS of the 47 patients was 94.2 months (95% CI: 51.7–136.7). There are distinctions in median OS between patients with different levels of CD3 and CD8 expression – high expression showed better OS – but they are not significantly associated with survival. However, for patients with high PD-L1 expression, their median OS are significantly shorter than patients with low expression (low vs high:122.5 vs 36.9 months, p = 0.0021). As the χ2 test indicated, CD3, CD8, and PD-L1 were not significantly correlated with clinical features in our study (Appendix S1 and Table SI), while the status of CD3 was positively correlated with CD8 (p < 0.001).
Efficacy of PD1 inhibitors in patients with hidradeno-carcinoma
In this study, we undertook an advanced evaluation of 3 advanced hidradenocarcinoma patients. They were treated with immunotherapy combined with chemotherapy in the intensive phase and immunotherapy in the maintenance phase. Detailed treatment history of the 3 patients are presented in Appendix S1 and Fig. S1. The clinical characteristics of the patients are as listed in Table III. They had low PD-L1 expression by histological examination. Their TPSs were < 1%, 2%, and 0, and their CPSs were 1, 5, and 0 (see Fig. 1). All 3 patients had an IS below 25%, indicating their low expression of PD-L1. Among them, 2 patients had TMB-H, with their TMB numbers being 17.28 and 32.64 (muts/Mb). They achieved PR while PFS reached 16.4 months and 12.3 months. One patient had a TMB-L of 5 (muts/Mb) and achieved CR, with a PFS that reached 28.8 months. The findings indicate that individuals diagnosed with hidradenocarcinoma, even those exhibiting low PD-L1 expression and TMB-L, can also benefit from anti-PD-1 immunotherapy in combination with chemotherapy.
DISCUSSION
Hidradenocarcinoma is a rare tumour with a poor prognosis when distant metastasis occurs. Standard treatments are lacking due to its rarity and the level of CD3+/CD8+ T cells and expression of PD-L1 has never been reported in hidradenocarcinoma. The CD3+/CD8+ T-cell density and PD-L1 expression have been established as biomarkers of prognosis and efficacy of PD-1 inhibitors in many studies (13–15). As our results indicate only a few patients had high CD3+/CD8+ T-cell infiltration and high expression of PD-L1, the majority of patients show a non-inflammatory tumour microenvironment. Furthermore, we found a negative survival effect of PD-L1in hidradenocarcinoma. High expression of PD-L1 may induce immune evasion in this tumour, as it can inhibit the activation of T cells and prevent tumour cells from being attacked by immune cells, thereby achieving tumour immune escape (16).
TMB and dMMR/MSI are sensitive biomarkers that illustrate the response to anti-PD-1 immunotherapy (17). KEYNOTE-158 research indicated that patients who have a TMB-H (> 10 mut/mb) have a comparatively good objective response rate (ORR) 29% when treated with pembrolizumab. Patients with MSI who received PD-1 therapy had an ORR of about 48% (9). A higher TMB results in a higher level of ORR to PD-1 inhibitors seen with a variety of tumour types, including non-small cell lung cancer (NSCLC) and melanoma (18). As Obermann et al. (19) reported, a metastatic cutaneous hidradenocarcinoma patient also had an exceptional response to anti-PD-1 treatment and achieved CR. The patient had TMB-H, MSI, and a high PD-L1 status. However, in our study 5/9 hidradenocarcinoma patients showed TMB-L (< 10 muts/Mb) and none of the patient showed MSI-H. Even with the low expression of PD-L1, it still provides potential possibilities for effective immunotherapy. At present, there are a few cases showing effective immunotherapy for advanced hidradenocarcinoma. Zhang et al. (20) reported a patient with hidradenocarcinoma who was treated with a PD-1 inhibitor combined with chemotherapy, and achieved a PR and PFS at more than 13 months despite negative PD-L1 expression and low TMB. The use of immunotherapy as a maintenance therapy after chemoradiotherapy is a good use of the combined immunotherapy modality. The PACIFIC trial (21) demonstrated a better OS and PFS in NSCLC patients treated with durvalumab after chemoradiotherapy compared with placebo. In our centre, we evaluated 3 cases of paclitaxel-based combination therapy with PD-1 inhibitors as maintenance therapy after chemotherapy, all of which achieved good PFS results. Overall, our study examined PDL1 expression and CD3+/CD8+ expression in hidradenocarcinoma patients. PD-1 inhibitors may be further explored as a new treatment option for patients with advanced hidradenocarcinoma. For example, for patients with TMB-H or MSI, single-agent immunotherapy may be an option, and for patients who are negative for all markers, a new generation of chemotherapy drugs combined with immunotherapy as maintenance therapy may be a good option.
Our results show that TP53 (33%) is the gene most likely to carry somatic mutations in hidradenocarcinomas. This is lower than the previously reported TP53 mutations in porocarcinomas, with mutation rates of up to 80% (22) and 60% (23). Apart from TP53 mutations, we identified the PI3KCA (22%) mutations as well as ERBB3 (22%) mutations in hidradenocarcinoma. Dias-Santagata et al. (24) also found that 40% of hidradenocarcinoma had PI3KCA-activating mutations. However, when mutations were classified according to operability level using the OncoKB framework, no treatable alterations were found in any of the 9 patients (grades 1–3), and only 1 patient had a single grade 4 alteration (NF1). Clinical studies of NF1 in solid tumours are currently underway (https://clinicaltrials.gov/). At the same time, we found the pathway of anti-EGFR resistance through functional enrichment analysis. Additionally, the study also identified a high frequency of ERBB2 variants through CNV analysis, which provides evidence for possible future anti-HER-2 treatment of hidradenocarcinoma patients.
Our study has certain limitations. Due to the rarity of hidradenocarcinoma, the sample size of patients receiving anti-PD-1 immunotherapy in this study was small. Nevertheless, our preliminary study of the prognosis of patients treated with PD1 inhibitors reveals for the first time the immune microenvironment of patients with hidradenocarcinoma, expanding the understanding of the genetic background of patients.
In conclusion, we found that the microenvironment of most hidradenocarcinoma patients was a comparative immune-desert type, and in a few samples sequenced, part of the population belonged to TMB-H. There are no identified targeted therapies available in patients with hidradenocarcinoma. In exploring clinical treatment, a PD-1 inhibitor combined with chemotherapy and PD1 as maintenance therapy has a good initial therapeutic effect for advanced patients with low PD-L1 expression and TMB-L, which provides a new idea and strategy for the application of an immune stimulant in advanced patients. Future studies with larger sample sizes are needed to explore the use of immunotherapy in patients with hidradenocarcinoma.
ACKNOWLEDGEMENT
This work was supported in part by the Natural Science Foundation of Fujian Province (Grant No. 2023J011254), the Science Foundation for the Excellent Youth Scholars of Fujian Provincial Health Commission (Grant No. 2022ZQNZD009), Joint Funds for the Innovation of Science and Technology, Fujian Province (Grant No. 2021Y9227), and Fujian Provincial Clinical Research Center for Cancer Radiotherapy and Immunotherapy (Grant No. 2020Y2012).
This study was approved by the ethics committee of the Fujian Medical University Cancer Hospital.
REFERENCES
- Gibbs DC, Yeung H, Blalock TW. Incidence and trends of cutaneous adnexal tumors in the United States in 2000–2018: a population-based study. J Am Acad Dermatol 2023; 88: 226–228.
- Guillot B. Unusual cutaneous malignancies: cutaneous adnexal tumours. In: Belkacémi Y, Mirimanoff R-O, Ozsahin M, editors. Management of rare adult tumours. Paris: Springer; 2009: p. 471–477.
- Baker MS, Yin VT, Ivan D, Allen RC, Carter KD, Esmaeli B, et al. Epidemiology and prognosis of primary periocular sweat gland carcinomas. Ophthalmic Plast Reconstr Surg 2017; 33: 101–105.
- Amel T, Olfa G, Faten H, Makrem H, Slim BA, Moncef M. Metastatic hidradenocarcinoma: surgery and chemotherapy. N Am J Med Sci 2009; 1: 372–374.
- Schreiber RD, Old LJ, Smyth MJ. Cancer immunoediting: integrating immunity’s roles in cancer suppression and promotion. Science (New York, NY) 2011; 331: 1565–1570.
- In GK, Nallagangula A, Choi JS, Tachiki L, Blackburn MJ, Capone S, et al. Clinical activity of PD-1 inhibition in the treatment of locally advanced or metastatic basal cell carcinoma. J Immunother Cancer 2022; 10(5): e004839.
- Liu D, Schilling B, Liu D, Sucker A, Livingstone E, Jerby-Arnon L, et al. Integrative molecular and clinical modeling of clinical outcomes to PD1 blockade in patients with metastatic melanoma. Nat Med 2019; 25: 1916–1927.
- Marabelle A, Fakih M, Lopez J, Shah M, Shapira-Frommer R, Nakagawa K, et al. Association of tumour mutational burden with outcomes in patients with advanced solid tumours treated with pembrolizumab: prospective biomarker analysis of the multicohort, open-label, phase 2 KEYNOTE-158 study. Lancet Oncol 2020; 21: 1353–1365.
- O’Malley DM, Bariani GM, Cassier PA, Marabelle A, Hansen AR, De Jesus Acosta A, et al. Pembrolizumab in patients with microsatellite instability-high advanced endometrial cancer: results from the KEYNOTE-158 Study. J Clin Oncol 2022; 40: 752–761.
- Pages F, Mlecnik B, Marliot F, Bindea G, Ou FS, Bifulco C, et al. International validation of the consensus Immunoscore for the classification of colon cancer: a prognostic and accuracy study. Lancet 2018; 391: 2128–2139.
- Li C, Huang C, Mok TS, Zhuang W, Xu H, Miao Q, et al. Comparison of 22C3 PD-L1 expression between surgically resected specimens and paired tissue microarrays in non-small cell lung cancer. J Thorac Oncol 2017; 12: 1536–1543.
- Sun JM, Shen L, Shah MA, Enzinger P, Adenis A, Doi T, et al. Pembrolizumab plus chemotherapy versus chemotherapy alone for first-line treatment of advanced oesophageal cancer (KEYNOTE-590): a randomised, placebo-controlled, phase 3 study. Lancet 2021; 398: 759–771.
- Alwers E, Kather JN, Kloor M, Brobeil A, Tagscherer KE, Roth W, et al. Validation of the prognostic value of CD3 and CD8 cell densities analogous to the Immunoscore (R) by stage and location of colorectal cancer: an independent patient cohort study. J Pathol Clin Res 2023; 9: 129–136.
- St Paul M, Ohashi PS. The roles of CD8 (+) T cell subsets in antitumor immunity. Trends Cell Biol 2020; 30: 695–704.
- Kumagai S, Togashi Y, Kamada T, Sugiyama E, Nishinakamura H, Takeuchi Y, et al. The PD-1 expression balance between effector and regulatory T cells predicts the clinical efficacy of PD-1 blockade therapies. Nat Immunol 2020; 21: 1346–1358.
- Jiang X, Wang J, Deng X, Xiong F, Ge J, Xiang B, et al. Role of the tumor microenvironment in PD-L1/PD-1-mediated tumor immune escape. Mol Cancer 2019; 18: 10.
- Fumet JD, Truntzer C, Yarchoan M, Ghiringhelli F. Tumour mutational burden as a biomarker for immunotherapy: current data and emerging concepts. Eur J Cancer 2020; 131: 40–50.
- Yarchoan M, Hopkins A, Jaffee EM. Tumor mutational burden and response rate to PD-1 inhibition. N Engl J Med 2017; 377: 2500–2501.
- Obermann H, Schmidle P, Steimle-Grauer SA, Pfarr N, Posch C. Exceptional response to anti-PD-1 treatment in a patient with metastatic cutaneous hidradenocarcinoma. Eur J Cancer 2021; 145: 143–145.
- Zhang W, Yang X, Wang Y, He L, Cheng D. Anti-PD-1 immunotherapy for advanced small sweat gland neoplasm: a case report. Chin J Cancer Prev Treatment 2021; 28:703–707.
- Spigel DR, Faivre-Finn C, Gray JE, Vicente D, Planchard D, Paz-Ares L, et al. Five-year survival outcomes from the PACIFIC trial: durvalumab after chemoradiotherapy in stage III non-small-cell lung cancer. J Clin Oncol 2022; 40: 1301–1311.
- Harms PW, Hovelson DH, Cani AK, Omata K, Haller MJ, Wang ML, et al. Porocarcinomas harbor recurrent HRAS-activating mutations and tumor suppressor inactivating mutations. Hum Pathol 2016; 51: 25–31.
- Bosic M, Kirchner M, Brasanac D, Leichsenring J, Lier A, Volckmar AL, et al. Targeted molecular profiling reveals genetic heterogeneity of poromas and porocarcinomas. Pathology 2018; 50: 327–332.
- Dias-Santagata D, Lam Q, Bergethon K, Baker GM, Iafrate AJ, Rakheja D, et al. A potential role for targeted therapy in a subset of metastasizing adnexal carcinomas. Mod Pathol 2011; 24: 974–982.