Atopic dermatitis is a chronically relapsing inflammatory skin condition that has profound impacts on quality of life of patients and their family. The aim of this study is to investigate the psychological stress in parents of children with atopic dermatitis in Korea, using data from the Korean National Health and Nutrition Examination Survey (KNHANES). This cross-sectional study included parents of participants under 19 years of age (970 with atopic dermatitis and 5,733 without atopic dermatitis after excluding those who meet the exclusion criteria) from the 2009 to 2012 KNHANES. The psychological stress state was evaluated with the following four questionnaire items: self-perception of stress, depressed mood, suicidal ideation, and diagnosis of depression by a physician. After adjusting for age, gender, education level, occupation, and marital status, logistic regression analyses indicated that mothers of children with atopic dermatitis had a higher frequency of stress perception (adjusted odds ratio (aOR) 1.46 (95% confidence interval (95% CI) 1.22–1.74), p < 0.01) and suicidal ideation (aOR 1.40 (95% CI 1.1–1.79), p < 0.01) than those without atopic dermatitis. In contrast, fathers of children with atopic dermatitis did not show a significant difference in all items compared with those of children without atopic dermatitis. Understanding the psychological stress in parents of children with atopic dermatitis is important for clinicians, since evaluation, management and support for parents, especially mothers, of children with atopic dermatitis are required.
Key words: atopic dermatitis; parents; mother; psychological stress.
Accepted Nov 8, 2022; Published Jan 9, 2023
Acta Derm Venereol 2023; 103: adv00844.
DOI: 10.2340/actadv.v103.2242
Corr: Young Min Park, Department of Dermatology, Seoul St Mary’s Hospital, College of Medicine, The Catholic University of Korea, 222 Banpo-daero, Seocho-gu, Seoul 06591, Korea. E-mail: 96015367@cmcnu.or.kr
SIGNIFICANCE
Atopic dermatitis is one of the most common skin diseases that adversely affects the quality of life of patients and even their families. As a result of analysing a database representing Korea, it was found that mothers of children with atopic dermatitis were more stressed than mothers of children without atopic dermatitis. The results of this study suggest that there is a need for evaluation, management and support for the stress experienced by mothers of children with atopic dermatitis.
INTRODUCTION
Atopic dermatitis (AD) is a chronic pruritic inflammatory skin disease with high prevalence in childhood and adolescents. Recent studies have reported that the prevalence of AD in these populations (6 months to <18 years) is 2.7–20.1% according to Asian, European and American data (1). The prevalence and incidence of AD have increased persistently over recent decades (2). AD is aggravated by various factors, such as stress, physical activities that cause sweating, and a dry atmosphere (3). The chronic course of the disease, including recurrent acute exacerbations, treatment burden (such as frequent moisturizing and steroid-phobia), dermatological complications, and coexisting medical comorbidities, as well as psychiatric conditions, degrade the quality of life (QoL) of patients and their families (4, 5).
A child’s chronic illness adversely affects the primary caregiver (6). In a prospective questionnaire-based study of 55 parents of children with AD, both mothers and fathers showed greater sleep loss, anxiety, and depression than parents of children with asthma (7). A recent paper reviewing 3,436 journals on the QoL of families of children with AD described caring for children with AD as a considerable, time-consuming, task that impairs personal relationships, decreases psychosocial functioning, and produces sleep disturbance (8).
The Korea National Health and Nutrition Examination Survey (KNHANES) is conducted by the Korea Centers for Disease Control and Prevention. This nationally representative cross-sectional survey includes approximately 10,000 individuals each year as a survey sample, and collects information on socioeconomic status, health-related behaviours, QoL, healthcare usage, anthropometric measures, biochemical and clinical profiles for non-communicable diseases, and dietary intake, using 3 component surveys: health interview, health examination, and nutrition survey (9).
Although several journals have reported the psychological stress in parents of children with AD, there has been no large-scale, well-designed statistical study. Therefore, the aim of this study is to investigate the psychological stress in parents of children with AD in Korea using the KNHANES data.
METHODS
Study design and participants
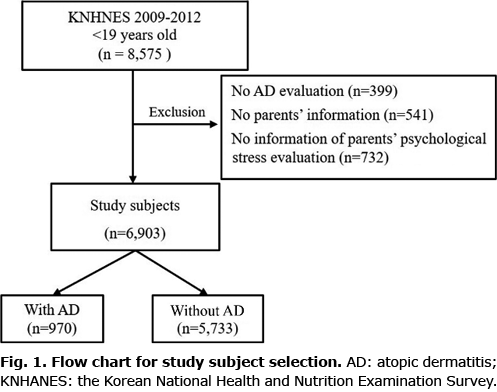
The study design was cross-sectional, using data from KNHANES (2009 to 2012) (https://knhanes.cdc.go.kr/knhanes/index.do) with the national representative sample through the multi-stage probability sampling method and a structured and validated questionnaire. Data were collected in a variety of ways, including household interviews, physical examinations, laboratory tests, and nutritional status assessments. All survey protocols were approved by the Korea Centers for Disease Control and Prevention (KCDCP) Institutional Review Board (IRB). Written informed consent was obtained from all participants before the survey began. The study included 8,575 people under 19 years of age from KNHANES (2009 to 2012). Among these, 541 participants with no parental information, 399 with no atopic disease evaluation and 732 participants with no information on parental psychological stress were excluded. The remaining 6,903 participants were included in the final analyses. 970 participants those who had been diagnosed with AD by a physician were assigned to an AD group, and the rest, 5733 participants were assigned to a group without AD (Fig. 1).
Data and measurements
In this study, all subjects in the national survey were evaluated equally, using the same questionnaire. The presence or absence of AD was investigated with the question, “Have you ever been diagnosed with AD by a physician?”. Psychological stress status was defined by a yes/no answer to 4 questions: Q1: “Do you feel stress in your daily life?”; Q2: “Have you experienced suicidal ideation within the last year?”; Q3: “Have you ever suffered from feeling down, depressed, or hopeless for 2 consecutive weeks or longer during the last year?”; and Q4: “Have you ever been diagnosed with depression by a doctor?’. Additional questionnaires, the EuroQol-5 dimension (EQ-5D) index (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) and the EuroQol Visual Analogue Scale (EQ-VAS), were performed.
Data obtained from the survey and anthropometric measurements for children included the following: socio-demographic factors of gender (male, female), age (< 10, ≥ 10 and < 15, and ≥ 15 years), household income (lowest quartile or others), and body mass index (BMI) (kg/m2). Data for parents included the following: socio-demographic factors of gender (male, female), age, education level (high school or more; or not), BMI (obese: ≥ 25 kg/m2 or not), abdominal obesity (≥ 90 cm for men and ≥ 85 cm for women); behavioural factors of smoking status (current smoker or not), the number of alcohol consumption per month (the percentage of drinking more than once a month in the last year), and physical activity (active, engaging in moderate or vigorous physical activity; inactive); allergic disease status, such as AD and asthma, systemic illness of hypertension (systolic blood pressure ≥ 140 mmHg, diastolic blood pressure ≥ 90 mmHg or taking antihypertensive drugs), diabetes mellitus (fasting blood sugar ≥ 126 mg/dl or taking diabetes medication or insulin injection or diagnosed by a doctor), and hypercholesterolaemia (fasting total cholesterol ≥ 240 mg/dl or taking cholesterol medication).
Statistical analysis
Frequencies of distribution of the baseline characteristics of the study participants were analysed using a χ2 test, and the effect of size on the difference in frequency distribution in each variable was measured. The prevalence ratio and associations between factors and psychological states including stress were evaluated using multivariate logistic regression analysis adjusted by age in model 1 and age, gender, education level, occupation, and marital status in model 2. All statistical tests were 2-tailed with a 5% level of significance and performed using SAS version 9.3 (SAS Institute, Inc., Cary, NC).
Declaration of Helsinki
All procedures were carried out in accordance with relevant guidelines and regulations.
Ethics approval
All KNHANES surveys were conducted with the informed consent of participants by KCDCP, and the IRB of KCDCP approved the protocols of the KNHANES. This study used a dataset of the KNHANES that is open to the public for retrospective analysis, which did not include personally identifiable information.
RESULTS
Clinical characteristics of study subjects
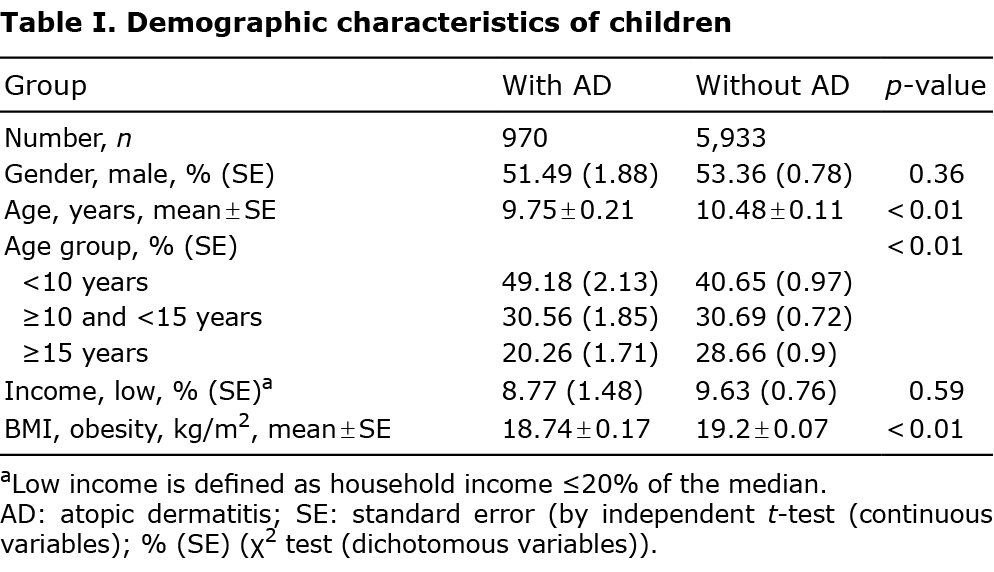
The number of children with AD was 970 (16.3% of the total). The mean age of children with AD was 9.75 years, and the mean age of the control group was 10.48 years. Because of the demographic characteristics of AD, a large proportion of the children with AD (48.18%) were less than 10 years old, which caused a difference in age composition from the control group (p < 0.01). Differences in income level and BMI (kg/m2) between the 2 groups were not significant (Table I).
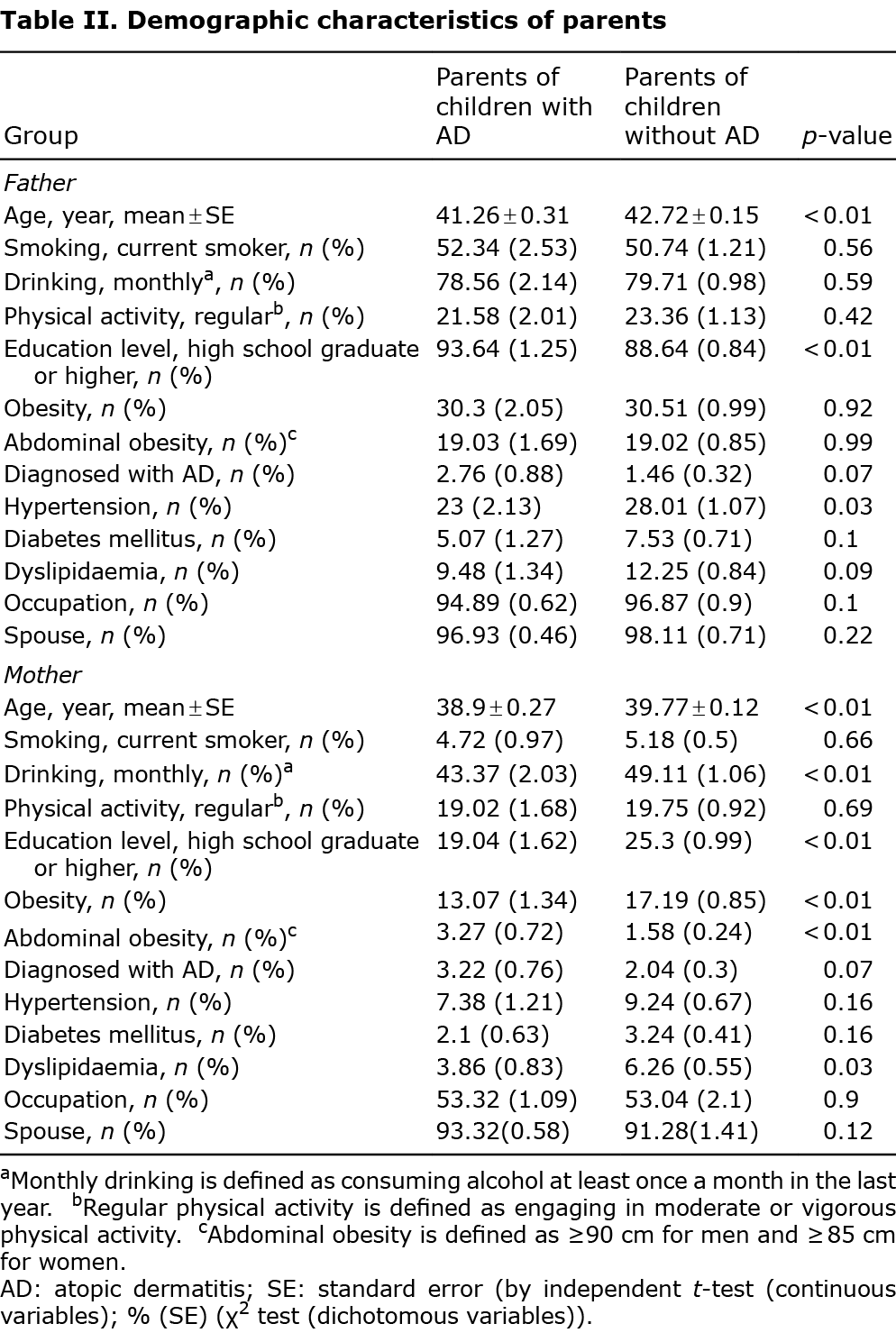
Regarding parental characteristics, the age of parents of children with AD was less than that of parents in the control group (41.26 vs 42.72 years for fathers and 38.9 vs 39.77 years for mothers). Mothers of children with AD consumed alcohol less frequently than did mothers in the control group (43.37% vs 49.11%, p < 0.01), and fathers of children with AD were more highly educated than fathers in the control group (93.64% vs 88.64%, p < 0.01). The mothers in the control group were significantly more obese (19.04% vs 25.03%, p < 0.01). The diagnosis rate of AD was significantly higher in mothers of children with AD (3.27 vs 1.58, p < 0.01). Differences in other characteristics, including smoking rate, physical activity level, abdominal obesity, and prevalence of hypertension, diabetes, and hyperlipidaemia, were not significant (Table II).
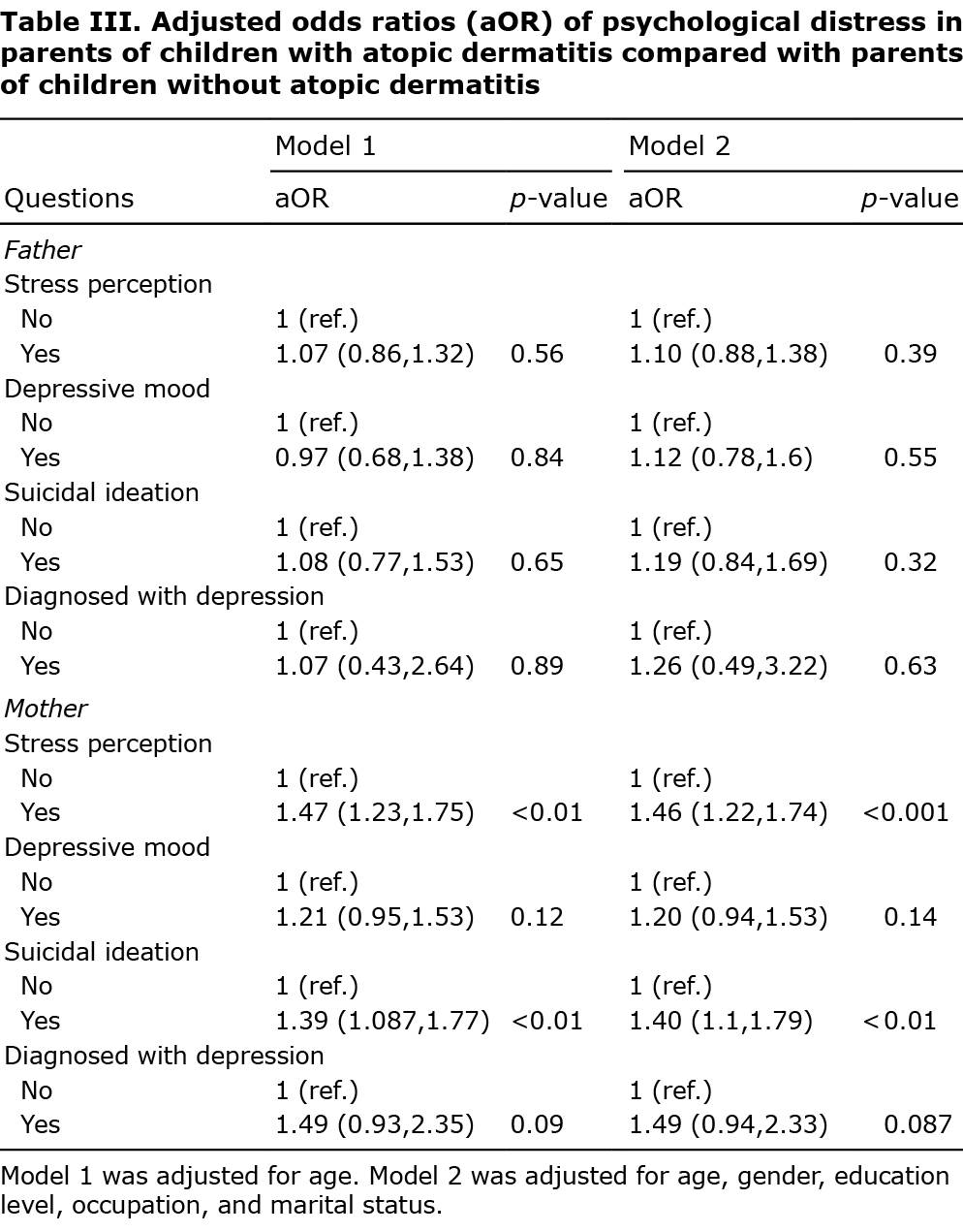
The answers to the 4 questions evaluating the subject’s psychological state included in the KNHANES are shown in Table III. After adjusting for age, gender, education level, occupation, and marital status, logistic regression analyses indicated that mothers of children with AD showed a significantly higher frequency of stress perception (adjusted odds ratio (aOR) 1.46 (95% confidence interval (95% CI) 1.22–1.74), p < 0.01) and suicidal ideation (aOR 1.40 (95% CI 1.1–1.79), p = 0.0066) than did mothers of children without AD. In contrast, fathers of children with AD did not show a significant difference in all items from those of children without AD.
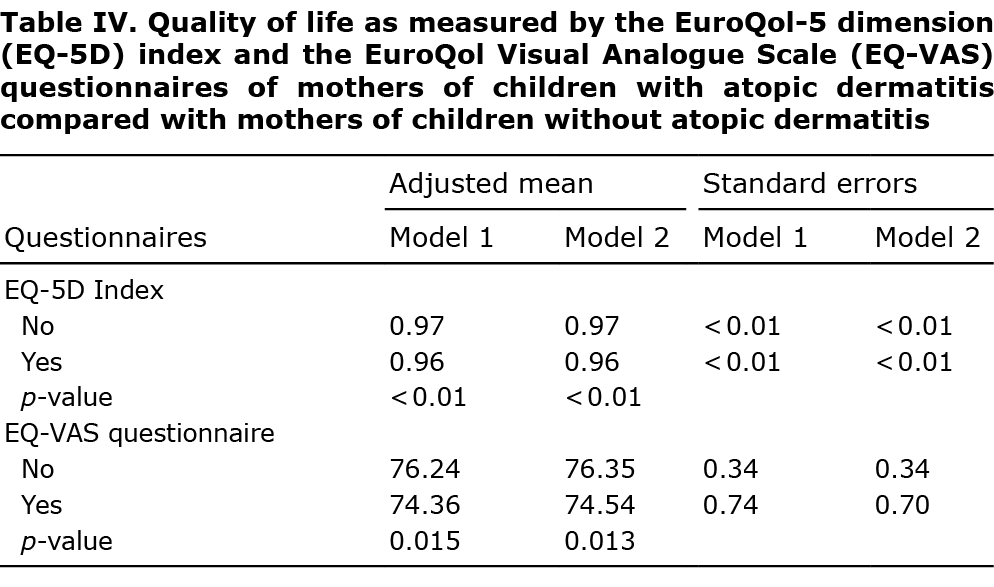
In addition, the results of evaluating the mother’s QoL with the EQ-5D index and EQ-VAS questionnaires are shown in Table IV. The QoL of mothers of children with AD was significantly lower than for mothers of children without AD in both the EQ-5D index (adjusted mean 0.96 vs 0.97, p < 0.01) and the EQ-VAS questionnaire (adjusted mean, 76.35 vs 74.54, p = 0.01). The mean EQ-5D index of the mothers of children with AD was 0.96, which was significantly lower than that of mothers of children without AD (mean EQ-5D index 0.97, p < 0.01). The mean EQ-VAS of mothers of children with AD was 74.54, which was significantly lower than that of mothers of children without AD (mean EQ-5D index 76.35, p = 0.01).
DISCUSSION
This study investigated psychological stress in parents of children with AD, using nationally representative survey data from KNHANES. Mothers of children with AD responded that they experienced stress perception and suicidal ideation more frequently than did mothers of children without AD. In contrast, fathers of children with AD showed no significant difference in stress experienced frequency from that of fathers of children without AD. These data are statistically more meaningful when adjusted for variables that show significant differences among socio-demographic factors, behavioural factors, and underlying disease status.
The increase in stress experience only in mothers of children with AD is consistent with the literature, which reports that parenting stress increases in mothers rather than in fathers (10, 11). One plausible explanation for the current findings regarding the psychological stress in mothers of children with AD is the time needed to care for children with AD. For all disease stages of AD, including eczema-free intervals, general measures, such as use of moisturizers, therapy for skin infection, avoidance of triggers, and education for children and caregivers, are recommended. Patients with AD need lifestyle management, such as washing their hands frequently, showering every day, and avoiding everyday objects that could be a source of infection. Education, such as behavioural therapy techniques and relaxation techniques, should be provided, and caregivers should be made aware of them (4, 12–14). A questionnaire study on the time taken to manage children with moderate or severe AD reported a mean of 63 min per day (15). However, another study of the same group showed a mean of 17 min per day (16). Variations in the results of these studies are probably due to the study design, which had a relatively small sample size and was conducted in a single institution. Nevertheless, caring for a child with AD is time-consuming.
The mean daily time spent doing housework in Korea is 49 min for men and 215 min for women. Compared with the international mean difference of 118 min, the difference in housework time between Korean women and men was much greater, at 166 min (17). This bias towards women in time spent performing housework could be the cause of the increased psychological stress in mothers compared with fathers. Also, prior studies have reported that mothers, who are more commonly involved in child-rearing than are fathers, feel guilty about the children’s symptoms and exhibit greater parenting stress than do fathers (18).
Many reports have studied parenting stress and the degraded QoL of caregivers, represented by parents of children with AD. One was a prospective comparative study of 55 children and 92 parents. The authors found that parents of children with AD showed sleep disturbances and increased anxiety level and depression scores (7). In addition, a survey-based study was conducted to investigate the QoL of parents of school children in a region in Korea. Although 22,904 children were included, the reliability of the study was low because the definition of AD was ambiguous (19). To overcome the limitations of these studies, the current study included a large sample size using a national representative sample. Also, based on the demographic characteristics accessible from the KNHANES, the current study tried to improve the reliability by adjusting the potential confounding factor.
Parents of young children with AD can be particularly burdened because of the lack of sleep and the emotional stress of seeing their child’s distress (20, 21). In a study of 270 patients with AD and parents in the USA, 61% of parents said their children’s AD interfered with their sleep (22). In a study of parents of inpatients with AD in Germany, the parental mental health score on the 12-Item Short Form Survey, a general measure of overall mental health, was significantly lower than the mean. Because patients with moderate-to-severe AD usually require inpatient treatment, it is difficult to apply this result to the entire family of children with AD (23). A prospective comparative study of 26 families with children with AD and 29 families with children with asthma compared the effects of these 2 diseases on parents’ sleep. Parents of children with AD spent more than 1 h caring for their children at night, whereas parents with asthma did not need additional night-time care (7). In addition, prolonged AD has been associated with depression, anxiety, attention deficit hyperactivity disorder, and suicidality (24–26). Also, decreased productivity at school, irritable mood, aggressive behaviour, sleep disturbance, and detrimental effects on emotional and social life at school are associated with AD (27). Mothers of children with eczema, who have severe sleep disruption, have significantly higher levels of anxiety and depression (7).
This study has a number of limitations. First, psychological stress in parents was evaluated only by simple self-reporting measures on the nature of data on the national population study. Furthermore, since the evaluation was performed only in the last year regarding depressed mood and suicidal ideation, the evidence may be insufficient, considering that AD is a chronic disease. Secondly, this study design did not have access to other factors, including personality, or family history of psychiatric disease, even though the study controlled several factors as potential confounding factors of psychological stress. Thirdly, because the presence of AD was determined by a single patient-retrieved question, the possibility of overdiagnosis could not be totally excluded. However, according to a previous study using the same database, the prevalence of AD in children was similar to those of previously reported studies (9). Therefore, we judged that the definition of AD used in that study was reliable. Finally, because this was a cross-sectional study, there are restrictions on the evaluation of cause-and-effect relationships between caring for children with AD and psychological stress.
Despite these limitations, the primary strength of the current study is that all the data were obtained from a nationwide population study with a high response rate and sufficient sample size, and the data provided representative information regarding the general Korean population. It is meaningful that analysis of the results of mothers and fathers separately showed the need to focus more on mothers, who are the main caregivers in Korean society, regarding stress management of parents. Furthermore, the findings have important implications for clinical practice with respect to the need for evaluation, management, and support for parents, especially mothers, of children with AD, along with education and stress relief programmes managed by the government.
The authors have no conflicts of interest to declare.
REFERENCES
- Silverberg JI, Barbarot S, Gadkari A, Simpson EL, Weidinger S, Mina-Osorio P, et al. Atopic dermatitis in the pediatric population: a cross-sectional, international epidemiologic study. Ann Allergy Asthma Immunol 2021; 126: 417–428.e412.
- Asher MI, Montefort S, Björkstén B, Lai CK, Strachan DP, Weiland SK, et al. Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC Phases One and Three repeat multicountry cross-sectional surveys. Lancet 2006; 368: 733–743.
- Yew YW, Thyssen JP, Silverberg JI. A systematic review and meta-analysis of the regional and age-related differences in atopic dermatitis clinical characteristics. J Am Acad Dermatol 2019; 80: 390–401.
- Ständer S. Atopic dermatitis. N Engl J Med 2021; 384: 1136–1143.
- Lawson V, Lewis-Jones MS, Finlay AY, Reid P, Owens RG. The family impact of childhood atopic dermatitis: the Dermatitis Family Impact Questionnaire. Br J Dermatol 1998; 138: 107–113.
- Chow MY, Morrow AM, Cooper Robbins SC, Leask J. Condition-specific quality of life questionnaires for caregivers of children with pediatric conditions: a systematic review. Qual Life Res 2013; 22: 2183–2200.
- Moore K, David TJ, Murray CS, Child F, Arkwright PD. Effect of childhood eczema and asthma on parental sleep and well-being: a prospective comparative study. Br J Dermatol 2006; 154: 514–518.
- ang EJ, Beck KM, Sekhon S, Bhutani T, Koo J. The impact of pediatric atopic dermatitis on families: a review. Pediatr Dermatol 2019; 36: 66–71.
- Lee JH, Han KD, Kim KM, Park YG, Lee JY, Park YM. Prevalence of atopic dermatitis in Korean children based on data from the 2008–2011 Korean National Health and Nutrition Examination Survey. Allergy Asthma Immunol Res 2016; 8: 79–83.
- Holmbeck GN, Coakley RM, Hommeyer JS, Shapera WE, Westhoven VC. Observed and perceived dyadic and systemic functioning in families of preadolescents with spina bifida. J Pediatr Psychol 2002; 27: 177–189.
- Han JW, Lee H. Actor and partner effects of parenting stress and co-parenting on marital conflict among parents of children with atopic dermatitis. BMC Pediatr 2020; 20: 141.
- Eichenfield LF, Tom WL, Berger TG, Krol A, Paller AS, Schwarzenberger K, et al. Guidelines of care for the management of atopic dermatitis: section 2. Management and treatment of atopic dermatitis with topical therapies. J Am Acad Dermatol 2014; 71: 116–132.
- Wollenberg A, Barbarot S, Bieber T, Christen-Zaech S, Deleuran M, Fink-Wagner A, et al. Consensus-based European guidelines for treatment of atopic eczema (atopic dermatitis) in adults and children: part I. J Eur Acad Dermatol Venereol 2018; 32: 657–682.
- Katayama I, Aihara M, Ohya Y, Saeki H, Shimojo N, Shoji S, et al. Japanese guidelines for atopic dermatitis 2017. Allergol Int 2017; 66: 230–247.
- Holm EA, Jemec GB. Time spent on treatment of atopic dermatitis: a new method of measuring pediatric morbidity? Pediatr Dermatol 2004; 21: 623–627.
- Jemec GB, Esmann S, Holm EA, Tycho A, Jørgensen TM. Time spent on treatment (TSOT). An independent assessment of disease severity in atopic dermatitis. Acta Dermatovenerol Alp Pannonica Adriat 2006; 15: 119–124.
- OECD. OECD Gender Data Portal. 2021 [Assessed on 05 July 2022] Available from: http://www.oecd.org/gender/data.
- Pustišek N, Vurnek Živković M, Šitum M. Quality of life in families with children with atopic dermatitis. Pediatr Dermatol 2016; 33: 28–32.
- Hwang TY, Kim SK, Kim SH, Kim M. A cross sectional survey on health-related quality of life among parents of children with allergic symptoms using the EQ-5D-5L. J Asthma 2019; 56: 1239–1245.
- Zuberbier T, Orlow SJ, Paller AS, Taïeb A, Allen R, Hernanz-Hermosa JM, et al. Patient perspectives on the management of atopic dermatitis. J Allergy Clin Immunol 2006; 118: 226–232.
- Drucker AM, Wang AR, Li WQ, Sevetson E, Block JK, Qureshi AA. The burden of atopic dermatitis: summary of a report for the national eczema association. J Invest Dermatol 2017; 137: 26–30.
- Chamlin SL, Mattson CL, Frieden IJ, Williams ML, Mancini AJ, Cella D, et al. The price of pruritus: sleep disturbance and cosleeping in atopic dermatitis. Arch Pediatr Adolesc Med 2005; 159: 745–750.
- Warschburger P, Buchholz HT, Petermann F. Psychological adjustment in parents of young children with atopic dermatitis: which factors predict parental quality of life? Br J Dermatol 2004; 150: 304–311.
- Silverberg JI. Comorbidities and the impact of atopic dermatitis. Ann Allergy Asthma Immunol 2019; 123: 144–151.
- Kage P, Zarnowski J, Simon JC, Treudler R. Atopic dermatitis and psychosocial comorbidities – what’s new? Allergol Select 2020; 4: 86–96.
- Deckert S, Kopkow C, Schmitt J. Nonallergic comorbidities of atopic eczema: an overview of systematic reviews. Allergy 2014; 69: 37–45.
- Kahn D, Iturriaga C, Bertran K, Fernandez I, Perez-Mateluna G, Borzutzky A, et al. Sleep quality in children with atopic dermatitis during flares and after treatment. Sleep Sci 2020; 13: 172–175.