The COVID-19 pandemic has led to enhanced hygiene procedures and use of personal protective equipment, but also to increased attention to occupational skin disease in healthcare workers. The occurrence of hand and facial skin disease in > 5,000 Swedish healthcare workers was investigated in a questionnaire survey. Levels of skin exposure related to hygiene procedures and personal protective equipment were recorded. Caring for patients with COVID-19 entailed higher levels of wet work and face mask exposures, and was associated with higher 1-year prevalence of both hand eczema (36%) and facial skin disease (32%) compared with not being directly engaged in COVID-19 care (28% and 22%, respectively). Acne and eczema were the most common facial skin diseases; for both, a dose-dependent association with face mask use was found. Dose-dependent associations could be shown between hand eczema and exposure to soap and gloves, but not to alcohol-based hand disinfectants.
Key words: occupational dermatitis; health personnel; COVID-19 pandemic; facial dermatoses; hand dermatoses; epidemiology.
Accepted Aug 18, 2021; Epub ahead of print Aug 24, 2021
Acta Derm Venereol 2021; 101: adv00543.
doi: 10.2340/00015555-3904
Corr: Nils Hamnerius, Department of Occupational and Environmental Dermatology, Lund University, Skåne University Hospital, Malmö, Sweden. E-mail: nils.hamnerius@med.lu.se
SIGNIFICANCE
Occupational skin disease was investigated in more than 5,000 healthcare workers. Wearing a face mask for more than 3 h daily was associated with facial skin disease, most commonly eczema and acne. Washing hands with soap more than 20 times daily and wearing gloves for more than 3 h daily was associated with hand eczema. Healthcare workers caring for COVID-19 patients were more exposed to face masks, soap, and gloves, and more often had face and hand skin disease. This indicates that the specific work routines related to the care of patients with COVID-19 increases the risk of occupational skin disease.
INTRODUCTION
Since the start of the COVID-19 pandemic there has been an increased attention to occupational skin disease in healthcare workers (HCWs). Hand eczema causes suffering in HCWs and entails costs for the individual and society (1, 2). It also carries a risk of transmitting infections, as hand eczema can increase the carriage of pathogenic microbes, including methicillin-resistant Staphylococcus aureus, on the skin (3–5). The impaired skin barrier in hand eczema makes alcohol-based hand disinfectants (AHDs) sting, which may reduce compliance with the mandatory hygiene procedures (6). Hand eczema in HCWs is associated with wet work exposure and contact allergies, primarily to rubber additives in medical gloves, but also to fragrances (6–8). Irritant contact dermatitis in HCWs has been associated mainly with exposure to soap and water, and to wearing occlusive gloves, while exposure to AHDs has not been shown to be a major factor (7, 9).
We have previously performed a questionnaire study on occupational wet work exposure and occurrence of hand eczema in HCWs in southern Sweden, including Region Skåne (7), and have investigated the causes of hand eczema with a clinical examination including contact allergy testing with patch testing in more than 450 HCWs (6). That survey resulted in increased recommendations regarding hand hygiene for HCWs, encouraging the use of AHDs and information on the risk of hand eczema associated with soap. This information has been used for educational purposes in HCWs in Region Skåne since 2019. A special concern in HCWs has been the introduction of new brands of AHDs, used during periods of shortage of products from the regular manufacturers. These brands were produced ad hoc by temporary manufacturers, and included products based on the WHO-recommended hand rub formulation (10).
Facial skin disease in HCWs has not previously been investigated in our region. The Department of Occupational and Environmental Dermatology, Lund University, Skåne University Hospital, Malmö, Sweden is the referral clinic for occupational skin disease in the region, and over recent years we have received only occasional referrals for possible face mask-related dermatitis. However, since the beginning of the COVID-19 pandemic we have received many referrals, not only for hand eczema, but also for facial skin disease in HCWs. Since the start of the COVID-19 pandemic there have also been a number of reports in the literature on facial skin disease related to face mask use (11, 12). We have therefore conducted a new questionnaire survey of occupational skin exposure and occurrence of hand and facial skin disease in HCWs.
The aims of this study were to investigate, in HCWs during the ongoing COVID-19 pandemic: (i) associations between hand eczema and wet work exposures, with a special focus on AHDs; (ii) associations between face mask use and facial skin disease; (iii) differences in skin exposure and occurrence of hand and facial skin disease between HCWs engaged vs HCWs not engaged in daily care of patients with COVID-19.
METHODS
Study group and questionnaire
The study population consisted of hospital-based employees in the County of Skåne in southern Sweden. There are 3 different hospital administrations in the county, with a total of 9 hospitals. An Internet-based questionnaire was distributed to all hospital-based staff members (n = 24,468) in the e-mail database provided by Region Skåne. This database also includes staff members who only temporarily serve at the hospitals in the county. Based on administration data at the time of the survey, approximately 60% of the staff included in the e-mail database were in service. Therefore, the survey reached approximately 15,000 hospital employees. HCWs were defined as respondents who reported that they were nurses, assistant nurses or physicians by profession. The HCWs who answered yes to the question “Do you on a daily basis care for or examine patients with COVID-19 infection?” (here referred to as “COVID-HCWs”) were compared with HCWs who were not engaged on a daily basis in the care of patients with COVID-19 (non-COVID-HCWs).
For the survey, an electronic, Internet-based application (Sunet Survey; Artologik, Växjö, Sweden) was used. The questionnaire was distributed during the second half of October 2020 and up to 4 reminders were sent. During the spring of 2020 the number of COVID-19 patients at the hospitals in southern Sweden was low compared with other regions of Sweden. It happened that the questionnaire was distributed at the start of the second wave of the pandemic, which was much more severe than the first wave (Appendix S1; Fig. S1). Until then face masks and face shields had been mandatory when engaged in the care of patients with suspected or confirmed COVID-19 infection, but not in other healthcare work. Recommendations on face mask use for all hospital employees irrespective of work tasks were not introduced until after the survey was completed. This allows for comparisons between different levels of face mask exposure.
Exposures surveyed were daily occupational use of soap and water (hereafter referred to as “soap”), AHD, disposable non-sterile examination gloves (hereafter called “disposable gloves”) and face masks. Age, sex, non-occupational skin exposure (soap, AHDs, face masks) and a history of atopic dermatitis (AD) were analysed as possible confounding factors.
The prevalence data are based on questions on self-reported hand eczema (13, 14), any facial skin disease as well as facial eczema, facial seborrhoeic dermatitis, acne, rosacea, and facial abrasions/wounds. AD data are based on self-reported history of childhood eczema (15).
Statistical analysis
For exposure data, descriptive statistics are presented. Correlations between different exposures were analysed using Spearman’s correlation analysis. Associations between exposures and self-reported eczema and facial skin disease, respectively, during the past 12 months were investigated using χ2 tests and odds ratios (ORs) obtained from univariate and multivariable logistic regression analysis. In the multivariable models, adjustments were made for non-occupational wet work and face mask exposure, respectively, as well as for age, sex, AD, and working hours. Respondents answering “other” for sex or “don’t know” for history of AD were not included in the regression analyses. The exposure data were grouped into 3 groups: “low”, “medium” and “high” exposure. For hand eczema, the 3 occupational wet work exposures soap, AHDs and disposable gloves were included in the same regression model.
Using the categorical variable as a continuous covariate in a separate regression model, p-values for trend were calculated when data were consistent with a possible trend.
Ethical approval
The study was approved by the Swedish Ethical Review Authority (Dnr 2020-01933).
RESULTS
There were a total of 6,886 respondents. Based on the number of questionnaires distributed, the overall response rate was 28% (6,886/24,468). However, as described, the number of possible respondents in service at the time of the distribution was probably no more than 15,000, and therefore a more realistic figure for the actual participation rate would be > 40% (6,886/15,000=0.46). Healthcare workers represented 74% (5,094/6,886) of the respondents. The non-HCW group was heterogeneous, with almost 100 different professions reported. In the following, the results and analysis presented represent the data of the HCW group unless otherwise stated. Data on reported exposures and diseases among all HCWs are presented first; thereafter, to illustrate the effect of COVID-19 care work, comparisons between COVID-HCWs and non-COVID-HCWs are presented.
The mean and the median age of respondents was 46 years; 83% (4,244/5,094) were female, and 15% (751/5,094) were COVID-HCWs. The mean time working as an HCW was 20 (median 19; range 1–55) years.
Wet work exposure and hand eczema for all healthcare workers
The point prevalence of hand eczema among all HCWs was 14% (708/5,094) and the 1-year prevalence was 29% (1,469/5,094). Exposure and background data for the whole group of HCWs, stratified according to occurrence of hand eczema within the past 12 months, are shown in Appendix S1; Table S1. A dose-dependent association was found between hand eczema and hand washing with soap at work and also duration of disposable glove wear, but not between hand eczema and use of AHDs or number of disposable gloves used. Odds ratios are summarized in Appendix S1; Table S2. Univariate analyses indicated a dose-dependent association between non-occupational hand washing with soap and hand eczema, but this finding did not reach statistical significance after adjustments were made in the multivariate analyses (p = 0.18). Analyses of correlations between different wet work exposures are shown in Appendix S1; Table S3. The most notable correlation was found between occupational and non-occupational soap exposure (Spearman’s correlation coefficient r = 0.63; p < 0.001).
Alcohol-based hand disinfectants from temporary producers
Use of AHD manufactured by temporary producers was reported by 30% of all HCWs, and by 36% of COVID-HCWs. Of the HCWs with hand eczema within the past 12 months, 37% reported use of these types of disinfectants, compared with 27% of those without hand eczema (p < 0.001).
Face mask use and facial dermatoses in all healthcare workers
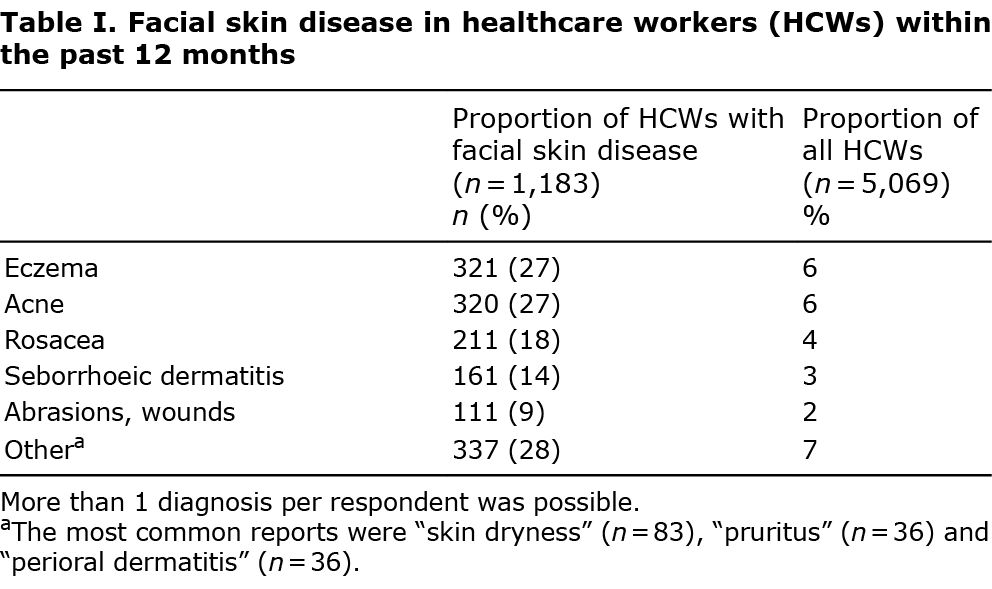
In the whole group of HCWs, wearing a face mask for 1–3 h on a daily basis was reported by 23%, and for > 3 h by 32%. The point prevalence of facial skin disease was 16% (829/5,069) and the 1-year prevalence was 23% (1,183/5,069) of HCWs (p < 0.001). Eczema and acne were the diagnoses most frequently reported (Table I).
Exposure and background data in the whole group of HCWs, stratified according to occurrence of facial skin disease within the past 12 months, are shown in Appendix S1; Table S4. A significant dose-dependent association was found between face mask use and facial dermatoses in general, and between face mask use and abrasions, eczema, acne, and rosacea (Fig. 1 and Appendix S1; Table S5).

Comparison between healthcare workers engaged, vs not engaged, in daily care of patients with COVID-19
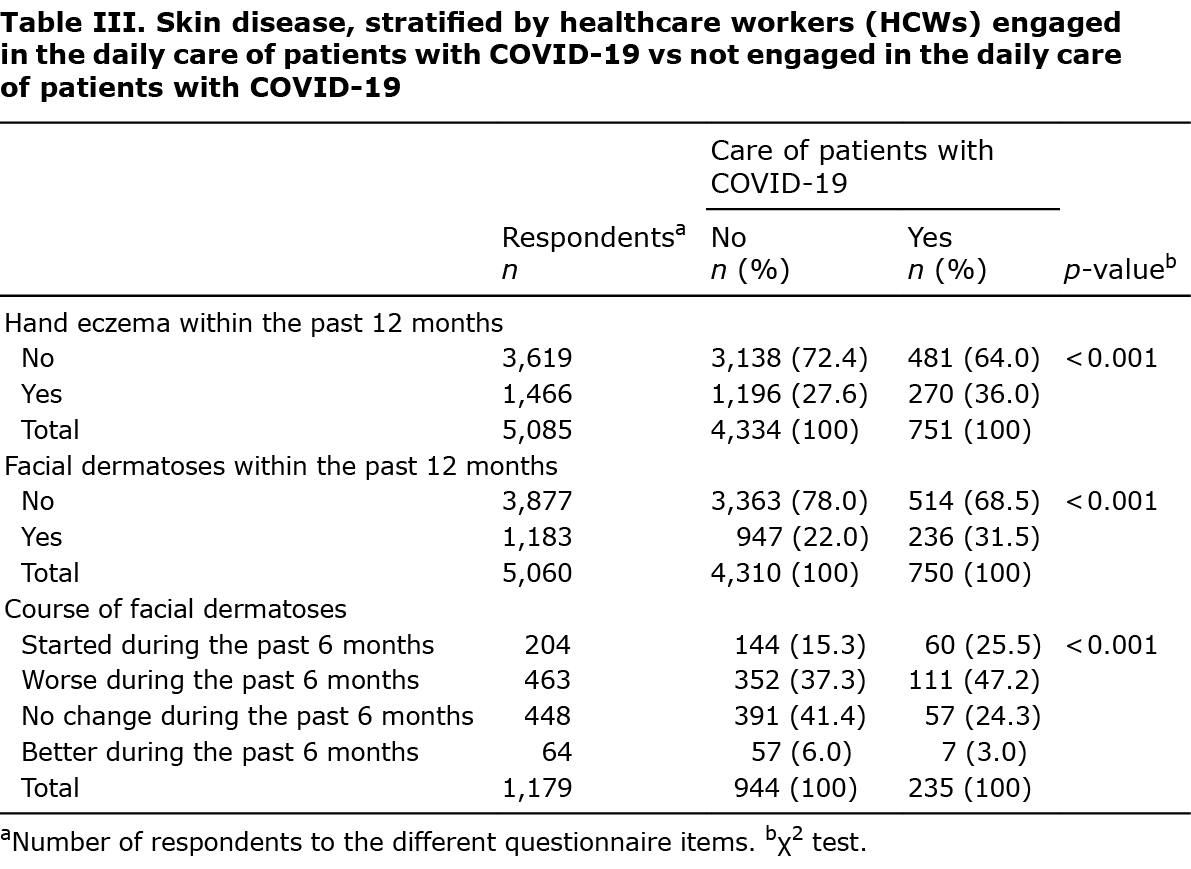
Wet work and face mask exposure levels were higher both at work and away from work for the 751 COVID-HCWs compared with the 4,334 non-COVID-HCWs (Table II). Hand eczema and facial skin disease were significantly more common in the COVID-HCWs (p < 0.001 for both) (Table III). Adjusted ORs (95% confidence intervals; 95% CIs) were 1.27 (1.06–1.53) for hand eczema during the past 12 months and 1.34 (1.11–1.62) for facial skin disease during the past 12 months. The most commonly reported facial skin disease in this group was acne (82/751; 11%), eczema (65/751; 9%) and abrasion or wound (44/751; 6%).

History of atopic dermatitis
Among all HCWs with a history of AD the 1-year prevalence of hand eczema and facial skin disease was 43% and 35%, respectively. A history of AD was associated with hand eczema (Appendix S1; Table S2) and facial dermatoses (adjusted OR (95% CI) 1.58 (1.36–1.83). Daily use of hand cream was more common in the AD group (p = 0.003), but the addition of hand cream use in the multivariate logistic regression model did not alter the associations between wet work exposure and hand eczema. Facial eczema and seborrhoeic dermatitis were more often reported in the AD group than in those with no history of AD (adjusted OR (95% CI) 3.46 (2.71–4.42) and 1.61 (1.13–2.3), respectively).
DISCUSSION
In this study, work in COVID-19 care, compared with other healthcare work, was found to be associated with increased occupational skin exposures and increased ORs for hand eczema and facial skin disease. This demonstrates that the extended hygiene procedures and the increased use of protective equipment required in the healthcare work related to patients with COVID-19 are associated with higher frequency of skin disease of the hands and face. In our previous survey of HCWs, in 2014, we found a 1-year prevalence of hand eczema of 21% (1,870/9,051 HCWs) (7). Therefore, in the current study not only HCWs engaged in the daily care of patients with COVID-19, but also HCWs not engaged in the care of patients with COVID-19 had a higher 1-year prevalence of hand eczema (28% vs 21%, a difference of 6.9 (95% CI 5.4–8.5) percentage points). This probably reflects a genuine increase in hand eczema during the COVID-19 pandemic, although a selection bias cannot be ruled out. However, the data do not indicate a selection of respondents with a high level of occupational wet work exposure; in fact, the proportion of respondents with high levels of occupational wet work exposure has not increased in comparison with the survey in 2014. By contrast, the proportion of respondents reporting non-occupational exposure to soap more than 10 times daily is markedly higher in the current study (53% vs 29%, a difference of 24 (95% CI 23–26) percentage points), possibly as a consequence of the general recommendations from the authorities during the pandemic. Therefore, even though we could not ascertain a dose-dependent association between non-occupational soap exposure and hand eczema, it appears that the increased levels of non-occupational wet work exposure during the pandemic contribute to the strain on the skin of the hands. Furthermore, we found a clear correlation between frequent hand washing with soap at work and away from work, as has been reported previously (7, 9). For the COVID-HCWs, not only occupational, but also non-occupational, levels of exposure to both soap and AHDs were higher compared with the non-COVID-HCWs. This indicates that increased attention to hygiene measures at work can also influence habits away from work.
Another factor that may have contributed to the higher 1-year prevalence of hand eczema reported in the current study could be an increased awareness of hand eczema in HCWs, possibly as a consequence of increased educational information on hand eczema directed to HCWs; a possibility that has been reported previously (16).
In experimental studies, AHDs have been found to be well tolerated by the skin barrier, and the irritant potential has been regarded as low (17–19). This has also been supported in epidemiological studies (7, 9). However, a recent study has indicated that AHDs can compromise skin barrier properties when applied with increased hydration (either by water immersion or through occlusion) (20), and an association between alcohol-based hand disinfection and symptoms of hand eczema in dermatological outpatients has been reported (21). Even though hand eczema in the current study was reported more frequently in HCWs with a high exposure to AHDs, when adjusted for hand washing, glove use and other confounding factors, no association could be ascertained. Also, when using a variable of more than 100 daily applications of AHD, no significant association could be shown (data not shown).
During the first months of the pandemic, temporary brands of hand disinfectants were used which, according to the respondents, often had an unpleasant smell. Temporarily produced hand disinfectants were used in all hospitals, but brands based on the WHO-recommended hand rub formulation were delivered to only 1 of the 3 hospital administrations: the administration with the highest proportion of respondents with hand eczema. The association between use of “temporary” disinfectants and hand eczema may be related to recall bias, but an irritant potential cannot be ruled out. The WHO formula contains a known irritant, hydrogen peroxide, but in a very low concentration that is unlikely to cause harm (22). We are currently investigating this matter further.
As in our previous study, we found an association between hand eczema and daily duration of wearing gloves, but not with the daily number of gloves, which indicates that it is the daily occlusion time that is of importance. It has been shown that respondents tend to overestimate the time of glove exposure (23, 24). If the overestimation of the duration of glove wear is higher in the high exposure level compared with the overestimation of the duration in the low exposure level, this can lead to an underestimation of the dose-response association between hand eczema and hours of glove wear.
Reports on facial skin disease in HCWs prior to the COVID-19 pandemic are scarce (25, 26). Facial dermatitis related to use of a face mask has been reported in dental care personnel (27), and in HCWs in connection with the SARS epidemic in 2002 to 2003 (28, 29). The present pandemic has generated a number of reports on face mask-related facial skin disease, both in HCWs and in the general population. The clinical picture has included abrasions, eczema/dermatitis, and acne (11, 30, 31). Possible factors are increased humidity and temperature under the mask, mechanical friction and pressure, and contact allergy to chemicals in the face mask (26, 32, 33).
With approximately 1 in 5 of all HCWs and 1 out of 3 COVID-HCWs reporting facial skin disease, the current study confirms that this is a common problem in healthcare work. In the majority of respondents the skin disease had started or deteriorated since the beginning of the pandemic, which indicates an association with changed routines in connection with the pandemic. Furthermore, the current study’s results demonstrate a dose-dependent association between daily duration of wearing a face mask and facial skin disease. This applies not only to abrasions, but also to acne, as well as to eczematous skin disease in the face area. A history of AD was associated with increased ORs for eczematous facial skin disease, but no association was found for acne or abrasions. In general, allergic contact dermatitis is not uncommon in facial dermatitis (34, 35), but to what extent this applies to occupational skin disease in HCWs is not well studied. As the current study is a questionnaire study no conclusions regarding contact allergy can be made; for this, contact allergy testing studies are needed.
Limitations and strengths
The response rate in this study is a matter of concern. It is possible that the strained working conditions of the ongoing pandemic contributed to the low response rate. However, low response rates are not uncommon in recent cross-sectional questionnaire studies (36, 37). Because of the extensive character of the e-mail address database used for distribution of the survey, it is not possible to calculate the exact response rate. Assuming a response rate of approximately 40%, and further assuming that the 1-year prevalence for the non-responders would be between half and twice that found in the responders, this would give a possible range for 1-year prevalence of hand eczema of between 20% and 46%. Corresponding figures for facial skin disease would be 16–37%. The prevalence data on skin diseases must be interpreted with caution, both with regard to a possible selection bias of respondents with skin disease, which might lead to an overestimation of the prevalence of skin disease, and with regard to the data being self-reported. However, as for the association analyses, a bias of the associations between skin disease occurrence and exposure rates would be dependent on skewed reporting of both disease occurrence and exposure rates, which is less likely.
The accuracy of self-reported facial skin disease is not well known. In 1 validation study on skin diseases in adults, diagnosis-based self-reports underestimated the actual prevalence of acne (38). We chose to use diagnosis-based rather than symptom-based questions on facial skin diseases. It is possible that symptom-based questions have better sensitivity, although they are less specific. As the majority of the respondents had some level of medical education, we assumed that terms such as “eczema”, “acne” and “rosacea” would be relatively well known, and therefore that questions containing these would be more informative than questions on “erythema”, “pimples”, “itch”, or “burning sensations”. In the questionnaire, one alternative to the diagnosis of the facial skin disease was “other”, with a possibility to enter a comment. The comments included both reports on symptoms, such as itch, but also rather specific diagnoses, such as perioral dermatitis and psoriasis.
The survey did not include lifestyle factors, such as smoking, obesity, care of infants or household work at home. In our previous study we found an association between hand eczema and obesity and kitchen work, respectively (8). However, the effect was limited; adjusting for these factors did not influence the association between hand eczema and occupational wet work exposures. As the current study was conducted during the ongoing pandemic, we aimed to reduce the number of questions. Therefore, lifestyle factors were not included.
The strength of the current study is that it is a large-scale cross-sectional study conducted in a total of 9 hospitals. The study was conducted during the beginning of the second wave of the pandemic, and allows for comparisons between HCWs in regular healthcare and those engaged in COVID-19 care. It provides data on dose-related associations between skin disease and occupational skin exposures related to the ongoing COVID-19 pandemic.
Conclusion
Changes in skin exposure during the pandemic have resulted in occupational skin disease in HCWs, especially in HCWs directly engaged in the care of patients with COVID-19. Providing COVID-19 care has entailed higher exposure to soap, AHDs, disposable gloves and face masks, and the current study population was associated with higher prevalences of both hand eczema and facial skin disease. Exposure to soap and gloves was associated with hand eczema in a dose-dependent way, as was face mask use with facial skin disease. Although hand eczema was associated with reporting an increased use of AHD, and with reporting exposure to temporarily produced AHD, no dose-dependent association between hand eczema and disinfectant exposure could be ascertained in multivariate regression analysis. Acne and eczema were the most commonly reported facial skin diseases. In the majority of cases, facial skin disease was of recent onset, namely since the start of the pandemic.
ACKNOWLEDGEMENTS
Conflicts of interest. MB is a member of an expert panel for fragrance safety (http://fragrancesafetypanel.org/). The other authors have no conflicts of interest to declare.
REFERENCES
- Diepgen TL, Scheidt R, Weisshaar E, John SM, Hieke K. Cost of illness from occupational hand eczema in Germany. Contact Dermatitis 2013; 69: 99–106.
- Lindberg M, Isacson D, Bingefors K. Self-reported skin diseases, quality of life and medication use: a nationwide pharmaco-epidemiological survey in Sweden. Acta Derm Venereol 2014; 94: 188–191.
- Brans R, Kolomanski K, Mentzel F, Vollmer U, Kaup O, John SM. Colonisation with methicillin-resistant staphylococcus aureus and associated factors among nurses with occupational skin diseases. Occup Environ Med 2016; 73: 670–675.
- Mernelius S, Carlsson E, Henricson J, Löfgren S, Lindgren PE, Ehricht R, et al. Staphylococcus aureus colonization related to severity of hand eczema. Eur J Clin Microbiol Infect Dis 2016; 35: 1355–1361.
- Nørreslet LB, Edslev SM, Andersen PS, Plum F, Holt J, Kjerulf A, et al. Colonization with Staphylococcus aureus in patients with hand eczema: prevalence and association with severity, atopic dermatitis, subtype and nasal colonization. Contact Dermatitis 2020; 83: 442–449.
- Hamnerius N, Svedman C, Bergendorff O, Björk J, Bruze M, Engfeldt M, et al. Hand eczema and occupational contact allergies in healthcare workers with a focus on rubber additives. Contact Dermatitis 2018; 79: 149–156.
- Hamnerius N, Svedman C, Bergendorff O, Björk J, Bruze M, Ponten A. Wet work exposure and hand eczema among healthcare workers: a cross-sectional study. Br J Dermatol 2018; 178: 452–461.
- Aalto-Korte K, Koskela K, Pesonen M. Allergic contact dermatitis and other occupational skin diseases in health care workers in the Finnish Register of Occupational Diseases in 2005–2016. Contact Dermatitis 2021; 84: 217–223.
- Ibler KS, Jemec GB, Agner T. Exposures related to hand eczema: a study of healthcare workers. Contact Dermatitis 2012; 66: 247–253.
- World Health Organization, Safety WHOP. WHO guidelines on hand hygiene in health care. Geneva: World Health Organization; 2009. Available from: http://www.who.int/gpsc/5may/en/
- Zuo Y, Hua W, Luo Y, Li L. Skin reactions of N95 masks and medial masks among health-care personnel: a self-report questionnaire survey in China. Contact Dermatitis 2020; 83: 145–147.
- Trepanowski N, Larson AR, Evers-Meltzer R. Occupational dermatoses among frontline healthcare workers during the COVID-19 pandemic: a cross-sectional survey. J Am Acad Dermatol 2021; 84: 223–225.
- Meding B, Barregård L. Validity of self-reports of hand eczema. Contact Dermatitis 2001; 45: 99–103.
- Svensson A, Lindberg M, Meding B, Sundberg K, Stenberg B. Self-reported hand eczema: symptom-based reports do not increase the validity of diagnosis. Br J Dermatol 2002; 147: 281–284.
- Stenberg B, Lindberg M, Meding B, Svensson A. Is the question ‘Have you had childhood eczema?’ useful for assessing childhood atopic eczema in adult population surveys? Contact Dermatitis 2006; 54: 334–337.
- Fisker MH, Ebbehøj NE, Vejlstrup SG, Lindschou J, Gluud C, Winkel P, et al. Prevention of hand eczema: effect of an educational program versus treatment as usual – results of the randomized clinical PREVEX trial. Scand J Work Environ Health 2018; 44: 212–218.
- Pedersen LK, Held E, Johansen JD, Agner T. Less skin irritation from alcohol-based disinfectant than from detergent used for hand disinfection. Br J Dermatol 2005; 153: 1142–1146.
- Houben E, De Paepe K, Rogiers V. Skin condition associated with intensive use of alcoholic gels for hand disinfection: a combination of biophysical and sensorial data. Contact Dermatitis 2006; 54: 261–267.
- Löffler H, Kampf G, Schmermund D, Maibach HI. How irritant is alcohol? Br J Dermatol 2007; 157: 74–81.
- Plum F, Yüksel YT, Agner T, Nørreslet LB. Skin barrier function after repeated short-term application of alcohol-based hand rub following intervention with water immersion or occlusion. Contact Dermatitis 2020; 83: 215–219.
- Kendziora B, Guertler A, Ständer L, Frey S, French LE, Wollenberg A, et al. Evaluation of hand hygiene and onset of hand eczema after the outbreak of SARS-CoV-2 in Munich. Eur J Dermatol 2020; 30: 668–673.
- Murphy EC, Friedman AJ. Hydrogen peroxide and cutaneous biology: translational applications, benefits, and risks. J Am Acad Dermatol 2019; 81: 1379–1386.
- Anveden I, Meding B. Skin exposure in geriatric care – a comparison between observation and self-assessment of exposure. Contact Dermatitis. 2007; 57: 253–258.
- Lund T, Flachs EM, Ebbehøj NE, Bonde JP, Agner T. Wet work exposure: comparison of observed and self-reported data. Int Arch Occup Environ Health 2019; 92: 317–326.
- Bhoyrul B, Lecamwasam K, Wilkinson M, Latheef F, Stocks SJ, Agius R, et al. A review of non-glove personal protective equipment-related occupational dermatoses reported to EPIDERM between 1993 and 2013. Contact Dermatitis 2019; 80: 217–221.
- Yu J, Chen JK, Mowad CM, Reeder M, Hylwa S, Chisolm S, et al. Occupational dermatitis to facial personal protective equipment in health care workers: a systematic review. J Am Acad Dermatol 2020; 84: 486–494.
- Kanerva L, Alanko K, Jolanki R, Kanervo K, Susitaival P, Estlander T. The dental face mask – the most common cause of work-related face dermatitis in dental nurses. Contact Dermatitis 2001; 44: 261–262.
- Foo CC, Goon AT, Leow YH, Goh CL. Adverse skin reactions to personal protective equipment against severe acute respiratory syndrome – a descriptive study in Singapore. Contact Dermatitis 2006; 55: 291–294.
- Donovan J, Skotnicki-Grant S. Allergic contact dermatitis from formaldehyde textile resins in surgical uniforms and nonwoven textile masks. Dermatitis 2007; 18: 40–44.
- Singh M, Pawar M, Bothra A, Maheshwari A, Dubey V, Tiwari A, et al. Personal protective equipment induced facial dermatoses in healthcare workers managing Coronavirus disease 2019. J Eur Acad Dermatol Venereol 2020; 34: e378–e380.
- O’Neill H, Narang I, Buckley DA, Phillips TA, Bertram CG, Bleiker TO, et al. Occupational dermatoses during the COVID-19 pandemic: a multicentre audit in the UK and Ireland. Br J Dermatol 2021; 184: 575–577.
- Hua W, Zuo Y, Wan R, Xiong L, Tang J, Zou L, et al. Short-term skin reactions following use of N95 respirators and medical masks. Contact Dermatitis 2020; 83: 115–121.
- Han HS, Shin SH, Park JW, Li K, Kim BJ, Yoo KH. Changes in skin characteristics after using respiratory protective equipment (medical masks and respirators) in the COVID-19 pandemic among health care workers. Contact Dermatitis 2021 Apr 4 [Epub ahead of print].
- Schnuch A, Szliska C, Uter W. Allergisches Gesichtsekzem. Auswertungen des IVDK und Literaturübersicht. Hautarzt 2009; 60: 13–21.
- Warshaw EM, Schlarbaum JP, Maibach HI, Silverberg JI, Taylor JS, Atwater AR, et al. Facial dermatitis in male patients referred for patch testing: retrospective analysis of North American Contact Dermatitis Group data, 1994 to 2016. JAMA Dermatol 2020; 156: 79–84.
- Kingston LM, O’Connell NH, Dunne CP. A comparative study of hand hygiene and alcohol-based hand rub use among Irish nursing and medical students. Nurse Educ Today 2018; 63: 112–118.
- Sturm H, Rieger MA, Martus P, Ueding E, Wagner A, Holderried M, et al. Do perceived working conditions and patient safety culture correlate with objective workload and patient outcomes: a cross-sectional explorative study from a German university hospital. PloS One 2019; 14: e0209487.
- Jagou M, Bastuji-Garin S, Bourdon-Lanoy E, Penso-Assathiany D, Roujeau JC. Poor agreement between self-reported and dermatologists’ diagnoses for five common dermatoses. Br J Dermatol 2006; 155: 1006–1012.