ORIGINAL REPORT
Patient Preferences in the Treatment of Moderate-to-severe Atopic Dermatitis
Mahreen AMEEN1, Raed ALHUSAYE2, Henrik BRANDI3, Mette BØGELUND4, Henrik H. JENSEN4, Signe B. REITZEL4 and Jacob P. THYSSEN3,5
1Royal Free London NHS Foundation Trust, London, UK, 2Sunnybrook Health Sciences Centre, Division of Dermatology, Toronto, Canada, 3LEO Pharma A/S, Ballerup, Denmark, 4EY Economics Denmark, Frederiksberg, Denmark, and 5Bispebjerg Hospital, Department for Dermatology, Copenhagen, Denmark
Atopic dermatitis is a chronic, inflammatory skin disease. A variety of systemic treatments are available for patients with moderate-to-severe atopic dermatitis. The efficacy, safety and administration profile of these treatments vary, and determining the optimal treatment strategy may require weighing the benefits and drawbacks of therapies with diverse characteristics. This study used an online discrete choice experiment survey to investigate treatment preferences among adults with atopic dermatitis from Denmark, France, the UK, or Canada. Participants were identified through existing online panels. The survey includ-ed questions regarding different treatment attributes, defined based on currently approved treatments for moderate to severe atopic dermatitis. Treatment preferences were measured as the relative importance of different treatment attributes. A total of 713 respondents met the inclusion criteria and completed the survey. The discrete choice experiment identified a significant preference for avoiding the risk of severe adverse events, and for oral pill every day compared with biweekly injections. The time to full effect was not rated as being important. These findings suggest that patients with moderate-to-severe atopic dermatitis prioritize safety as most important, followed by ease of administration in their treatment preferences, while time to full effect and monitoring requirements were the least important attributes.
Key words: adult dermatology; patient-centred care; patient participation; patient preferences; treatment preferences.
SIGNIFICANCE
A variety of systemic treatments are available for patients with moderate-to-severe atopic dermatitis. This study found that avoiding risk of severe adverse events and ease of administration were the most valued treatment attributes by patients with moderate-to-severe atopic dermatitis. Time to full effect and monitoring requirements were the least important treatment attributes. The findings of the study are relevant, as understanding patient preferences may improve shared decision-making in atopic dermatitis patient care and enhance treatment adherence.
Citation: Acta Derm Venereol 2024; 104: adv24339. DOI https://doi.org/10.2340/actadv.v104.24339.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Submitted: Oct 26, 2023; Accepted: Jan 10, 2024; Published: Feb 21, 2024
Corr: Henrik Brandi, LEO Pharma A/S, Industriparken 55, DK-2750 Ballerup, Denmark. E-mail: HEBRD@Leo-pharma.com
Competing interests and funding: HB and JPT are employees at LEO Pharma. MB, SBR and HHJ are employees of EY Economics Denmark, which is a paid vendor of LEO Pharma. MA has been a principal/chief investigator for clinical trials and/or served as an advisor for Elly Lilly, LEO Pharma, Pfizer, AbbVie, Regeneron and Sanofi. RA has received grants/research contracts from AbbVie and Novartis and served as a consultant and received honoraria from AbbVie, Galderma, LEO Pharma, Novartis, Pfizer and Sanofi-Genzyme. JPT has received grants from The Leo Foundation, The Novo Nordisk Foundation, The Lundbeck Foundation and grants from Savværksejer Jeppe Juhl og hustru Ovita Juhls Mindelegat, during the conduct of the study. Outside of this study, JPT has served as an advisor for AbbVie, Almirall, Arena Pharmaceuticals, Coloplast, OM Pharma, Aslan Pharmaceuticals, Union Therapeutics, Eli Lilly & Co, LEO Pharma, Pfizer, Regeneron, and Sanofi-Genzyme, and served as a speaker for AbbVie, Almirall, Eli Lilly & Co, LEO Pharma, Pfizer, Regeneron, and Sanofi-Genzyme, and received research grants from Pfizer, Regeneron, and Sanofi-Genzyme.
INTRODUCTION
A topic dermatitis (AD) is a chronic, inflammatory skin disease with a complex pathophysiology characterized by skin barrier abnormalities and immune dysregulation. AD is characterized by intense itch and recurrent eczematous skin lesions and is associated with skin pain, sleep disturbance, anxiety, depression, and work absenteeism (1–6).
A variety of systemic treatments are available for patients with moderate-to-severe AD, including broad-acting systemic immunosuppressive therapies, as well as newer systemic therapies, such as janus kinase (JAK) inhibitors and more targeted antibodies that neutralize a specific cytokine or block its receptors, such as tralokinumab and dupilumab, respectively (7, 8). The efficacy, safety and administration profile of these treatments vary (9), and determining the optimal treatment strategy may require weighing the benefits and drawbacks of therapies with diverse characteristics.
There is a discrepancy between patients’ preferences and those of physicians acting on behalf of patients (10, 11), emphasizing the importance of incorporating patient perspectives in decision-making processes (11, 12). The concept of patient-centred care has gained increasing recognition among stakeholders. To improve shared decision-making in AD patient care, it is crucial to understand how patients value different attributes of systemic treatment options and to what extent these factors influence their preferences (7, 11, 12). Furthermore, treatment adherence is closely tied to patient preferences, indicating that understanding patient preferences may contribute to improved adherence (13).
Discrete choice experiments (DCEs) can be employed to elicit patients’ preferences for various treatment attributes, such as efficacy, associated risk and mode of administration (14, 15). DCE results can quantify the importance patients place on each attribute and estimate the trade-offs they are willing to make. This study aimed to investigate patients’ preferences in the treatment of moderate-to-severe AD by assessing the treatment attributes most valued by patients.
MATERIALS AND METHODS
This study investigated patient preferences related to different product characteristics of hypothetical treatments for AD using a patient survey and DCE technique.
Study population
The target population for this survey comprised adults with moderate-to-severe AD. The study included patients aged 18 years or older, who had a Patient-Oriented Eczema Measure (POEM) score of > 7, or who had currently or previously used systemic treatment. POEM is a subjective disease severity score commonly used in clinical practice to monitor treatment response. The POEM score ranges from 0 to 28, with a POEM score > 7 signifying at least moderately severe AD (16, 17). Respondents not meeting these inclusion criteria were screened out during the survey.
The survey was distributed to a random, demographically balanced sample of people living in Denmark, France, the UK, or Canada. People who had previously agreed to answer online surveys were identified via existing e-mail panels held by professional e-mail panel service providers. The use of online panels enabled tracking of respondents and the demographic balance, as well as targeting of surveys to specific countries, if needed.
The survey was developed using the online survey software SurveyXact (18), ensuring complete participant anonymity. Before starting the survey, all participants provided informed consent, and they could withdraw from the survey at any time.
Discrete choice experiment
Attributes. The DCE is a stated preference method that estimates individuals’ preferences for services, policies, and interventions by presenting several paired alternatives. Participants choose the alternative they prefer for each pair. Each alternative consists of a combination of attributes with multiple levels (19–21). The attributes included in the alternatives should represent the product characteristics, and each attribute’s established levels should ideally cover all possible or hypothetical outcomes (19). However, this may be impractical, as the number of choice sets required increases with the addition of more attributes and levels.
The DCE used in this study presented participants with different hypothetical treatment options for AD, composed of varying levels of the included attributes. Based on the decisions that participants made regarding the different alternatives and attribute levels, it is possible to measure the relative preference for different attributes (i.e. product characteristics) and the trade-off individuals are willing to make among these attributes, such as preferring a treatment with a higher risk of adverse events, but improved efficacy (19–21). DCEs serve as a method of generating a rich data source for healthcare decision-making, and the stated preference method has been recognized as valuable in understanding patient preferences (14, 15).
Treatment attributes were defined based on characteristics of currently approved treatments for moderate-to-severe AD and their treatment effects. They were determined through a thorough review of results from existing randomized controlled trials. Three medical experts selected the final attributes after an extensive discussion. To ensure the DCE design’s manageability, only severe adverse events were included in the DCE design, while additional questions were added to capture direct preferences for non-severe adverse events.
Participants were introduced to all treatment attributes before responding to the DCE survey questions. The survey included a DCE consisting of 6 treatment attributes, as follows:
- Mode of administration
- Time until full effect
- Level of itch
- Effect on appearance
- Monitoring due to the risk of severe adverse events
- Risk of severe adverse events that cannot be monitored.
Each attribute was assessed at 2–4 levels to capture variations in each attribute and reveal preferences in AD treatment. The attributes, including their levels and attribute descriptions, are listed in Table I.
Design of the DCE survey. A complete factorial choice design would result in (2×3×4×4×2×2) = 384 potential attribute combinations and 384×384 = 147,456 possible choice sets combinations with 2 alternatives. To create a manageable number of choice sets, a D-efficient design with Bayesian priors was employed, generating 24 choice sets using the NGENE software.
To prevent participant fatigue from too many questions while maintaining a wide range of attribute combinations, participants were randomly assigned to 1 of 3 blocks in the survey. To enable investigation of all 24 choice sets, each block included 8 choice sets with 2 alternatives that were unique for the block. Participants therefore only received questions from the block they were assigned.
The survey comprised 23 screening and disease history questions followed by the patient preference section. The latter included 2 administration-related questions, 8 discrete choice questions, a question specifically about other adverse events, 11 questions from the Dermatology Life Quality Index, 2 questions on healthcare service delivery in respective countries, 3 time-preference questions, and 5 socio-economic questions.
Data collection
A pilot phase was conducted in December 2020 with 70 adults to test the survey’s functionality and accuracy. This pilot study led to minor changes in the questionnaire and a change in the inclusion criteria. Participants from the pilot study were not included in the final analyses. The main data collection took place between July and August 2021.
Data validation
Participants who completed the DCE module in less than 30 s were excluded from preference estimation. Data were validated prior to statistical analysis by checking for consistency and errors.
Statistical analyses
Survey question data were analysed using univariate descriptive statistics (means, medians, modes, and frequencies). A conditional logit model was used to determine the coefficients of the 6 included attributes and respective levels in terms of preferred product characteristics. The probability of choosing alternative j from nj choices in the choice scenario i can be described as:
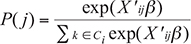
Since the estimates from the conditional logit model were calculated as ratios of 2 stochastic variables, 95% confidence intervals (95% CI) could not be derived directly from these estimates. Instead, 95% CI was established using bootstrapping, with 10,000 replications performed to estimate the 95% CI.
Sub-analyses stratified based on age, sex, disease severity, itch level and Investigator Global Assessment (IGA) level were conducted to investigate whether preference patterns differed between subgroups. To compare the relative importance of different attributes within subgroups, each attribute was compared with the mean of all attributes for each subgroup.
In addition to the preferences identified with the DCE, participants answered 2 questions regarding other (non-severe) adverse events prevalent among AD treatments. A review of the safety profile of all clinical trials within AD treatments was conducted to identify product-specific adverse events and their risk percentages. Based on this, participants were asked to choose the worst and second worst adverse event among:
- 15% risk of common cold
- 15% risk of pink eye
- 10% risk of acne
- 5% risk of herpes
All statistical analyses were carried out using SAS Version 9.4 (SAS Institute Inc., Cary, NC, USA).
Patient and public involvement
This study did not involve patients or the public in the design, conduct, reporting or dissemination plans of the research.
RESULTS
Sample
Out of 1,221 adults with AD who received the survey, 413 (34%) had a POEM score ≤ 7 and were naïve to systematic treatment. Consequently, these participants were excluded. Participants naïve to systemic treatment were included if they had a POEM score > 7. Moreover, 95 participants were excluded due to partial completion of the survey. Fig. 1 presents a flowchart of the study population.
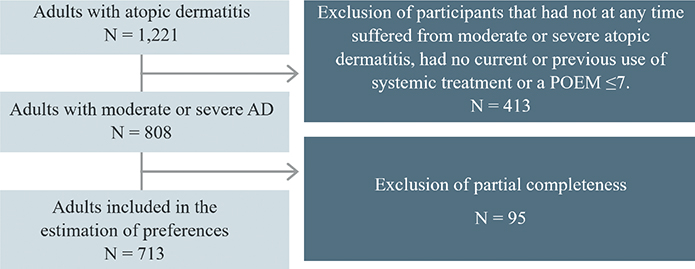
Fig. 1. Flowchart of the study population. POEM: Patient Oriented Eczema Measure.
A total of 713 adults (58%) with a POEM score > 7, or current or previous use of systemic treatment, completed the survey and were included in the analysis. The included participants had mean age of 40 years, with 64% being female, and a mean POEM score of 12.4. Out of these participants, 30% were currently on systemic treatment, 38% had previously received systemic treatment, and 32% were naïve to systemic treatment. Out of these participants, the mean ± standard deviation (SD) POEM scores forPOEM scores for those currently on systemic treatment, previously on systemic treatment, and naïve to systemic treatment were 13.2 ± 6.7, 10.1 ± 7.6, and 14.2 ± 5.1, respectively.
Participants were affected by AD in 1 or more body regions, with all body regions being reported as affected by AD across the sample. Table II present baseline demographics and treatment- and disease-specific characteristics.
| Baseline demographics | n (%) | |
| Total population | 713 (100) | |
| Systemic treatment | ||
| Currently on systemic treatment | 214 (30) | |
| Previously on systemic treatment | 269 (38) | |
| Systemic treatment naive | 230 (32.3) | |
| Country | ||
| Canada | 173 (24) | |
| Denmark | 180 (25) | |
| France | 194 (27) | |
| UK | 166 (23) | |
| Age, years | ||
| 18–29 | 207 (29) | |
| 30–44 | 253 (35) | |
| 45–59 | 150 (21) | |
| 60 and older | 103 (14) | |
| Age, mean (SD) | 40.3 (15.2) | |
| Sex | ||
| Male | 256 (36) | |
| Female | 457 (64) | |
| Self-perceived rating of atopic dermatitis | ||
| Mild | 220 (31) | |
| Moderate | 372 (52) | |
| Severe | 83 (12) | |
| Do not know | 38 (5) | |
| POEM score (total population), mean (SD) | 12.4 (6.8) | |
| POEM score (currently on systemic treatment) | 13.2 (6.7) | |
| POEM score (previously on systemic treatment) | 10.1 (7.6) | |
| POEM score (naïve to systemic treatment)a | 14.2 (5.1) | |
| The onset of symptoms, age mean (SD) | 19.3 (15.5) | |
| Diagnosis, age mean (SD) | 22.3 (15.9) | |
| Other diseases | ||
| Hay fever | 287 (40) | |
| Allergic conjunctivitis | 90 (13) | |
| Food allergy | 190 (27) | |
| Other allergies | 166 (23) | |
| Asthma | 209 (29) | |
| Depression | 192 (27) | |
| Skin infections | 134 (19) | |
| None of the above | 151 (21) | |
| Baseline symptoms, n (%) | ||
| Body parts usually affected | Mildly affected | Severely affected |
| Face | 244 (34) | 85 (12) |
| Scalp | 276 (39) | 144 (20) |
| Arms | 304 (43) | 191 (27) |
| Hands | 247 (35) | 196 (27) |
| Torso | 197 (28) | 96 (13) |
| Back | 214 (30) | 99 (14) |
| Crotch/genitals | 160 (22) | 75 (11) |
| Legs/feet | 284 (40) | 177 (25) |
| Baseline treatment use, n (%) | ||
| Treatments | Current use | Previous use |
| Antihistamines | 212 (30) | 223 (31) |
| Antibiotics | 106 (15) | 249 (35) |
| Oral steroids | 90 (13) | 210 (29) |
| Oral systemic therapies (such as immunosuppressants and retinoids) | 86 (12) | 167 (23) |
| Biologic treatment (injections) | 83 (12) | 101 (14) |
| Light therapy or phototherapy | 79 (11) | 193 (27) |
| Emollient or moisturizers | 418 (59) | 166 (23) |
| Calcineurin inhibitor | 89 (12) | 126 (18) |
| Potent or very potent corticosteroids | 210 (29) | 229 (32) |
| Other treatments | 105 (15) | 140 (20) |
| aPatients naïve to systemic treatment could only participate in the study if they had a POEM score > 7. | ||
| SD: standard deviation; POEM: Patient-Oriented Eczema Measure. | ||
Preferences
The statistical analyses revealed that the participants rated the attribute risk of severe adverse events as most important relative to the other included attributes, with a coefficient of 0.42 (95% CI 0.36–0.49). However, the attribute mode of administration was deemed to be almost as important as the risk of severe adverse events, with a coefficient of 0.41(95% CI 0.35–0.48). At the same time, reduced time to full effect was considered one of the least important attributes, with a coefficient of 0.04 (95% CI 0.02–0.06) for a 4-week reduction in time to onset of action, while avoiding monitoring for severe adverse events had a coefficient of 0.02 (95% CI –0.03–0.07). In order of importance, the DCE identified a significant preference for avoiding the risk of severe adverse events, pills taken daily instead of injections every second week, reduced itching (0.25 (95% CI 0.19–0.30)), effect on appearance (0.16 (95% CI 0.10–0.21)), and reduced time to full effect. The attribute to avoid monitoring for severe adverse events was not statistically significant. Results of the entire study population are presented as the relative importance of the included treatment attributes in Fig. 2.
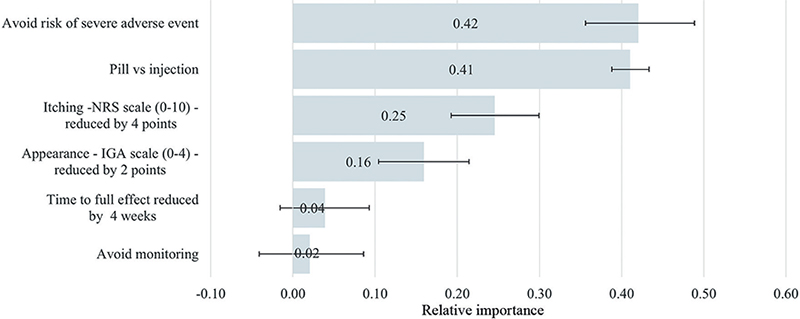
Fig. 2. Relative importance. IGA: Investigator Global Assessment, NRS: The Itch Numeric Rating Scale.
Results from the partial sub-analyses stratified on age, sex, disease severity, itch level and IGA level for appearance did not reveal any significant difference in preference pattern when different subgroups were compared.
The assessment of other adverse events commonly associated with AD treatments revealed the following preferences among participants: 57% thought a 5% risk of herpes was the worst or second-worst adverse event, 49% considered a 15% risk of pink eye as the worst or second-worst adverse event, 39% ranked a 10% risk of acne as the worst or second-worst adverse event, and 28% identified a 15% risk of common cold as the worst or second-worst adverse event (Fig. 3).
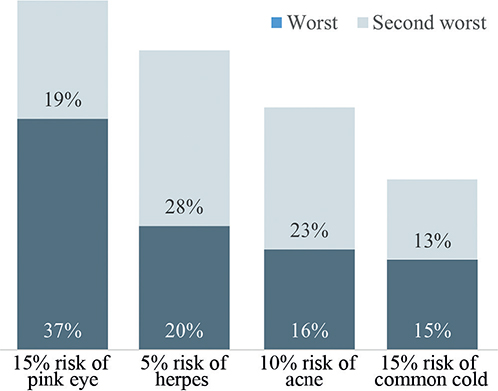
Fig. 3. Combination of adverse events and risk percentage considered to be worst or second worst.
DISCUSSION
This study on adults with moderate-to-severe AD revealed that safety was the most important product characteristic of AD treatments, suggesting that patients with moderate-to-severe AD have a strong preference for avoiding the risk of severe adverse events. This was closely followed by a preference for pills taken daily over injections every second week. In addition, the study showed that reduced itching was considered more important by patients than the effect on the appearance of symptoms, although this DCE did not find a significant difference in the relative importance of the 2 attributes. The least important product characteristics were reduced time to full effect and avoiding monitoring of severe adverse events. These results suggest that patients with moderate-to-severe AD are willing to accept a slower onset of action for effect in exchange for safer treatments, with lower or no risk of severe adverse events. There was no statistically significant difference between the preferences for the 2 attributes of risk of severe adverse events and administration, meaning that the relative importance of reducing the risk of severe adverse events and oral administration compared with bi-weekly injection is similar, for patients with moderate-to-severe AD in the included countries.
The sample spans across multiple countries and matches the AD patient population in terms of the distribution within age and sex. According to a systematic literature review from 2020 the prevalence of AD is higher in females than males; however, no trend exists for the age distribution (22). The current study sample includes a comparable number of patients across the 4 age groups although there are fewest participants from the oldest age group (> 60 years). Females constitute 64% of the study sample. This suggests that conclusions from the present study can be generalized across the broader patient group.
The attribute regarding the risk of adverse events was constructed to only include the risk of severe adverse events. As a result, the relative importance identified for this attribute might be influenced by participants’ perceptions of which adverse events are considered severe. The categorization considered in this study may differ from that considered by participants. As an add-on to the DCE, the study identified the worst and second worst non-severe adverse event associated with existing AD treatments. The risk of experiencing each of the 4 adverse events was established based on clinical trial safety profiles. However, newer real-world data has demonstrated that the prevalence of dupilumab-associated pink eye is 26%, almost a doubling of the risk from the clinical safety profiles (23). Therefore, this disparity between clinical trial and real-world data could mean that patients’ responses to the questions regarding non-severe adverse events may have been different if the presented associated risks had been higher. It is important to note that the administration attribute in this DCE contained only 2 levels: pills every day or injections every second week. While the approved dosing for dupilumab is every second week, tralokinumab is also approved for a maintenance dose of every 4 weeks injections for patients who achieve clear or almost clear skin after 16 weeks of treatment (10, 24). Patient preferences regarding treatment administration might have been different if participants were given the option of subcutaneous injections at other intervals, such as every 4 weeks.
In line with the findings of the current DCE, Thomas et al. (25) found that the mode of administration significantly impacted patients’ preferences. Participants in their study prioritized increased efficacy and reduced risk, but were willing to accept reduced efficacy to receive treatment orally every day instead of as injections every second week (25). In a qualitative study from 2022, Ervin et al. (26) investigated the importance of treatment administration in patients with AD. Overall, the study found that convenient and easy administration was a key driver of patient preferences. Orally administered therapies were considered easy and rapid to take, although participants expressed a concern about taste and formulation. Injectable administrations were also considered relatively easy; however, most participants preferred oral administration due to fear of needles. As with the mode of administration, participants preferred the treatment frequency that was least intrusive, meaning the least frequent (26).
Boeri et al. (7) published a DCE including 320 adults with moderate-to-severe AD, which included 3 attributes related to reduced safety risk: risk of serious infection, risk of venous thromboembolism, and risk of malignancy. In addition, attributes of time to onset of itch relief, probability of skin clearance at 16 weeks, and mode of administration were included in the DCE. The annual risk of malignancy was identified as the most important attribute across all attributes, highlighting the importance of safety in the view of the patients (7, 25).
The qualitative study by Ervin et al. (26) explored treatment preferences across different age groups. Their study, which included adults, adolescents and children (using caregivers as proxy), revealed differences in the relative importance of attributes across age groups: safety was more important for adults and caregivers than for adolescents, while the administration attribute was more important for caregivers and adolescents compared with adults. Therefore, the results of adult studies, including our own, cannot be extrapolated to children and adolescents, and further studies of these younger age groups will help to identify their treatment priorities.
The results from this study add to the existing literature on patients’ preferences for various attributes of AD treatments. Understanding patients’ preferences is of great importance, since accounting for this when initiating treatments has the potential to improve the quality of care provided and patients’ adherence to treatment (13).
In conclusion, this study suggests that safety is the most important attribute for adults with moderate-to-severe AD when choosing among hypothetical AD treatments, followed by treatment administration. Conversely, time to full effect and monitoring requirements were the least important attributes.
ACKNOWLEDGEMENTS
The author(s) disclosed receipt of the following financial support for the research and publication of this article: This work was supported by LEO Pharma (grant number is not applicable).
Institutional Review Board approval status: Originating from Denmark, this study does not necessitate ethical approval provided that participants remain anonymous, their participation is voluntary, and they can withdraw without repercussions. It should be noted that all of these conditions were duly met in the conduct of this study.
REFERENCES
- Vakharia PP, Chopra R, Sacotte R, Patel KR, Singam V, Patel N, et al. Burden of skin pain in atopic dermatitis. Ann Allergy Asthma Immunol 2017; 119: 548–552.e3.
- Nutten S. Atopic dermatitis: global epidemiology and risk factors. Ann Nutrit Metab 2015; 66: 8–16.
- Silverberg JI, Gelfand JM, Margolis DJ, Boguniewicz M, Fonacier L, Grayson MH, et al. Pain is a common and burdensome symptom of atopic dermatitis in United States adults. J Allergy Clin Immunol Pract 2019; 7: 2699–2706.e7.
- Boguniewicz M, Leung DYM. Atopic dermatitis: a disease of altered skin barrier and immune dysregulation: Immune response in atopic dermatitis. Immunol Rev 2011; 242: 233–246.
- Boguniewicz M, Fonacier L, Guttman-Yassky E, Ong PY, Silverberg JI. Atopic dermatitis yardstick update. Ann Allergy Asthma Immunol 2023; 130: 811–820.
- Weidinger S, Novak N. Atopic dermatitis. The Lancet 2016; 387: 1109–1122.
- Boeri M, Sutphin J, Hauber B, Cappelleri JC, Romero W, Di Bonaventura M. Quantifying patient preferences for systemic atopic dermatitis treatments using a discrete-choice experiment. J Dermatol Treat 2020; 33: 1449–1458.
- Bieber T, Paller AS, Kabashima K, Feely M, Rueda MJ, Ross Terres JA, et al. Atopic dermatitis: pathomechanisms and lessons learned from novel systemic therapeutic options. Acad Dermatol Venereol 2022; 36: 1432–1449.
- Silverberg JI, Thyssen JP, Fahrbach K, Mickle K, Cappelleri JC, Romero W, et al. Comparative efficacy and safety of systemic therapies used in moderate-to-severe atopic dermatitis: a systematic literature review and network meta-analysis. Acad Dermatol Venereol 2021; 35: 1797–1810.
- Adtralza EMA label. [cited 2023 Apr 3]. Available from: https://www.ema.europa.eu/en/documents/product-information/adtralza-epar-product-information_en.pdf
- de Bekker-Grob EW, Berlin C, Levitan B, Raza K, Christoforidi K, Cleemput I, et al. Giving patients’ preferences a voice in medical treatment life cycle: the PREFER Public–Private Project. Patient 2017; 10: 263–266.
- Li A, Zhang M, Yang Y, Zhang J, Xie X, Li X, et al. Patient-reported outcome (PRO) instruments for disease severity and quality of life in patients with atopic dermatitis: a systematic review of English and Chinese literature. Ann Transl Med; 2022; 10: 906.
- Laba TL, Essue B, Kimman M, Jan S. Understanding patient preferences in medication nonadherence: a review of stated preference data. Patient 2015; 8: 385–395.
- Guidance for Industry, Food and, Drug Administration Staff, and, Other Stakeholders. Patient Preference Information – Voluntary Submission, Review in Premarket Approval Applications, Humanitarian Device Exemption Applications, and De Novo Requests, and Inclusion in Decision Summaries and Device Labeling. 2016 [cited 2022 Nov 18]. Available from: https://www.fda.gov/media/92593/download
- Lancsar E, Louviere J. Conducting discrete choice experiments to inform healthcare decision making: a user’s guide. Pharmacoeconomics 2008; 26: 661–677.
- Charman CR, Venn AJ, Williams HC. The Patient-Oriented Eczema Measure: development and initial validation of a new tool for measuring atopic eczema severity from the patients’ perspective. Arch Dermatol 2004; 140: 1513–1519.
- Charman CR, Venn AJ, Ravenscroft JC, Williams HC. Translating Patient-Oriented Eczema Measure (POEM) scores into clinical practice by suggesting severity strata derived using anchor-based methods. Br J Dermatol 2013; 169: 1326–1332.
- Ramboll. SurveyXact. [cited 2022 Nov 24]. Available from: https://www.surveyxact.dk/
- Bridges JFP, Hauber AB, Marshall D, Lloyd A, Prosser LA, Regier DA, et al. Conjoint analysis applications in health – a checklist: a report of the ISPOR Good Research Practices for Conjoint Analysis Task Force. Value in Health 2011; 14: 403–413.
- Ryan M. Using conjoint analysis to elicit preferences for health care. BMJ 2000; 320: 1530–1533.
- Reed Johnson F, Lancsar E, Marshall D, Kilambi V, Mühlbacher A, Regier DA, et al. Constructing experimental designs for discrete-choice experiments: report of the ISPOR Conjoint Analysis Experimental Design Good Research Practices Task Force. Value Health 2013; 16: 3–13.
- Bylund S, Kobyletzki L, Svalstedt M, Svensson Å. Prevalence and incidence of atopic dermatitis: a systematic review. Acta Derm Venereol 2020; 100: adv00160.
- Halling AS, Loft N, Silverberg JI, Guttman-Yassky E, Thyssen JP. Real-world evidence of dupilumab efficacy and risk of adverse events: a systematic review and meta-analysis. J Am Acad Dermatol 2021; 84: 139–147.
- Drugs.com. [cited 2023 Mar 7]. Tralokinumab FDA label. Available from: https://www.drugs.com/dosage/tralokinumab.html
- Thomas C, Raibouaa A, Wollenberg A, Capron JP, Krucien N, Karn H, et al. Patient preferences for atopic dermatitis medications in the UK, France and Spain: a discrete choice experiment. BMJ Open 2022; 12: e058799.
- Ervin C, Crawford R, Evans E, Feldman SR, Zeichner J, Zielinski MA, et al. Patient and caregiver preferences on treatment attributes for atopic dermatitis. J Dermatolog Treat 2022; 33: 2225–2233.