QUIZ SECTION
Scattered Reddish-brown Nodules on the Head in an Elderly Man: A Quiz
Xuetong ZHANG, Jiali RUAN, Zhuangli TANG, Ru DAI and Zhongfa LV
Second Affiliated Hospital, School of Medicine, Zhejiang University, Zhejiang, China. E-mail: lzfskin@zju.edu.cn
Citation: Acta Derm Venereol 2023; 103: adv000857. DOI https://doi.org/10.2340/actadv.v102.2453.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Published: Jan 27, 2023
A Chinese 80-year-old man of yellow race developed scattered reddish-brown nodules on his head over a period of 4 months. The nodules were smooth and moderately hard, and ranged in diameter from 0.6 to 1 cm (Fig. 1). The patient had lanced and squeezed some nodules with a sharp tool 2 weeks previously, but the nodules did not resolve. He had no other symptoms, such as itching, burning sensation before treatment, and no intermittent fever, night sweats, or weight loss. Laboratory examination revealed leukocyte count 8.7×109/l (4.0–10.0/l), haemoglobin (Hb) 120 g/l (131–172 g/l), erythrocyte sedimentation rate (ESR) 27 mm/h (<15 mm/h), albumin 29.7 g/l (35.0–52.0 g/l), and immunoglobulins 27.3 g/l (15.0–30.0 g/l). Serological markers of hepatitis B, hepatitis C and HIV were negative. No other abnormalities were found in routine blood and biochemical tests. Ultra-sound radiography revealed enlarged lymph nodes in area III of the right side of the neck, with a size of approximately 1.58 × 0.99 cm. Chest computed tomography (CT) showed that the left upper lobe of the lung has been surgically removed. The patient had been diagnosed with lung adenocarcinoma 6 months previously and had completed surgical treatment. He also had a history of hypertension, diabetes and cerebral infarction.
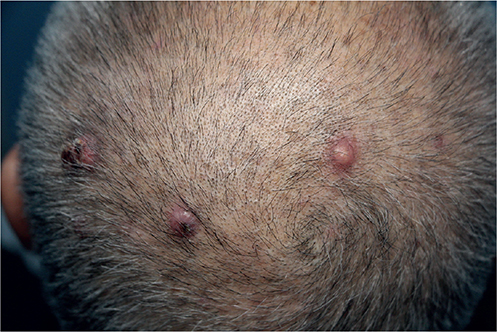
Fig. 1. Clinical image of scattered reddish-brown nodules on the head.
What is your diagnosis?
(A) Kimura disease (KD); (B) Angiolymphoid hyperplasia with eosinophilia (ALHE); (C) Metastatic carcinoma of skin; (D) Rosai-Dorfman-Destombes disease (RDD)?
See next page for answer.
ANSWERS TO QUIZ
Scattered Reddish-brown Nodules on the Head in an Elderly Man: A Commentary
Diagnosis: Rosai-Dorfman-Destombes disease (RDD)
Histopathological examination revealed emperipolesis, which was easily identifiable at different frequencies. The macrophages had open chromatin, distinct nucleoli and eosinophilic or foamy cytoplasm (Fig. 2A). Immunohistochemistry demonstrated infiltration of the tissues by plasma cells and a large number of histiocytes, the cytoplasm of which expresses S-100, CD-68 positivity and CD1a negativity, in contrast to Langerhans cell histiocytosis (LCH) (Fig. 2B, C, D). For isolated cutaneous nodules, electrocautery was performed on nodules 0.6 cm diameter and surgery on nodules >0.6 cm diameter (1). There has been no recurrence to date.
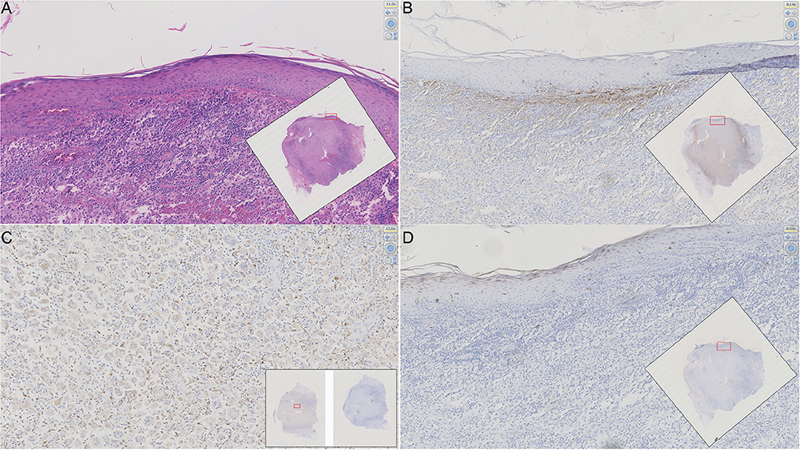
Fig. 2. Biopsy specimen of a nodule; original magnification ×40. (A) Cytology smear shows large histiocytes exhibiting emperipolesis and fragmented neutrophils (haematoxylin and eosin; H&E). Immunohistochemistry staining: (B) S100 positivity. (C) CD68 positivity. (D) CD1a negative.
Rosai-Dorfman-Destombes disease (RDD) and angiolymphoid hyperplasia with eosinophilia (ALHE) are not easy to distinguish based on the clinical manifestation of cutaneous nodules. The cutaneous nodules on the head of this elderly male patient were misdiagnosed as ALHE, but pathological examination corrected the preliminary diagnosis. Pathology is therefore important for dermatological diagnoses.
RDD is an uncommon non-Langerhans cell histiocytosis characterized by the infiltration of activated histiocytes into the affected tissues. The disease was first described by the French pathologist Pierre Paul Louis Lucien Destombes in 1965. More than 1,000 reports describing various aspects of the disease have been published (1). RDD is most frequently seen in children and young adults (mean age 20.6 years), although it has been reported up to age 74 years. The clinical manifestations of RDD are diverse, including progressive, painless, massive cervical lymphadenopathy, fever, leukocytosis, elevated ESR, hypogammaglobulinaemia and occasional anaemia. In 43% of patients, extranodal sites, such as the skin, central nervous system, lung, cardiothoracic area, subcutaneous tissue, salivary gland, orbit, bone marrow, breast, thyroid, cervix and kidney, are also affected. Ten percent of extranodal RDD cases involve the skin, and isolated skin diseases are rare (1, 2). The current patient had cutaneous manifestations and enlarged lymph nodes approximately 1.58 × 0.99 cm in area III of the right neck,.
Cutaneous lesions are usually slow-growing, painless, non-pruritic nodules, plaques or papules, ranging in colour from yellow to red to brown (3). RDD cells are polyclonal, reactive and non-neoplastic. They have abundant eosinophilic cytoplasm, central round nuclei and obvious nucleoli. The characteristic pathological changes are emperipolesis to varying degrees. Immunohistochemical staining showed S100+, CD68+ and CD1a– (4).
Differential diagnosis of RDD includes ALHE, Kimura disease (KD) and skin metastasis. ALHE is a rare benign angioproliferative disease that usually manifests as single or multiple pink to reddish-brown dome-shaped papules or nodules, most often on the head and neck. Lesions on the trunk, limbs and genitalia are rare. ALHE may be asymptomatic, itching, painful or bleed spontaneously. Histologically, ALHE shows vascular proliferation and infiltration of lymphocytes and eosinophils around epithelioid endothelial cells (5).
KD is a chronic inflammatory process that occurs mainly in young men in Asia. The lesion of the disease has a deeper location. Its clinical manifestation is a large subcutaneous mass, which usually affects the main salivary glands in the periauricular or submandibular region. KD is associated with peripheral blood eosinophilia and elevated serum total IgE. The most important pathological feature of KD is hyperplastic follicles with germinal centres surrounded by abundant eosinophilic infiltrations (6).
In addition, the current patient had a history of lung adenocarcinoma for 6 months, and metastatic tumours should be considered in the differential diagnosis. The scalp is a common site of skin metastasis of visceral malignant tumours. These often manifest as hard nodules with skin colour, red, violet or excessive pigmentation. However, other manifestations can occur, such as patches or plaques and ulcers. Pathological examination did not find characteristics of primary malignancy; hence metastatic cancer was excluded (7).
Treatment for RDD should be customized according to individual clinical conditions. Observation and follow-up are applicable for patients with simple lymphadenopathy or asymptomatic skin RDD. Surgical resection is curative for unifocal extranodal disease, and debulking may be warranted for upper airway obstruction, spinal cord compression, or large lesions causing end-organ compromise. Drug treatment should be selected according to the patient’s condition, including corticosteroids, sirolimus and chemotherapy, immunomodulatory medicine, such as thalidomide, and targeted medicine, such as cobimetinib (1).
This case suggests that, after excluding infection and cutaneous tumours, RDD should be considered in the diagnosis of elderly patients with multiple pink to reddish-brown dome nodules on the head and neck. Immunohistochemical examination is necessary.
REFERENCES
- Abla O, Jacobsen E, Picarsic J, Krenova Z, Jaffe R, Emile JF, et al. Consensus recommendations for the diagnosis and clinical management of Rosai-Dorfman-Destombes disease. Blood 2018; 131: 2877–2890.
- Rajyalakshmi R, Akhtar M, Swathi Y, Chakravarthi R, Bhaskara Reddy J, Beulah Priscilla M. Cytological diagnosis of Rosai-Dorfman disease: a study of twelve cases with emphasis on diagnostic challenges. J Cytol 2020; 37: 46–52.
- Al-Khateeb TH. Cutaneous Rosai-Dorfman disease of the face: a comprehensive literature review and case report. J Oral Maxillofac Surg 2016 74: 528–540.
- Cai Y, Shi Z, Bai Y. Review of Rosai-Dorfman disease: new insights into the pathogenesis of this rare disorder. Acta Haematol 2017; 138: 14–23.
- Buder K, Ruppert S, Trautmann A, Bröcker EB, Goebeler M, Kerstan A. Angiolymphoid hyperplasia with eosinophilia and Kimura’s disease – a clinical and histopathological comparison. J Dtsch Dermatol Ges 2014; 12: 224–228.
- Abuel-Haija M, Hurford MT. Kimura disease. Arch Pathol Lab Med 2007; 131: 650–651.
- Hu S, Chen G, Lu Y, Wu C-S, Lan C-CE. Cutaneous metastases from different internal malignancies: a clinical and prognostic appraisal. J Eur Acad Dermatol Venereol 2010; 22: 735–740.