ORIGINAL ARTICLE
Solar Urticaria: An Ambispective Study in a Long-term Follow-up Cohort with Emphasis on Therapeutic Predictors and Outcomes
David PESQUÉ1, Andrea CIUDAD2, Evelyn ANDRADES3, Dulce SOTO3, Ramon GIMENO3, Ramon M. PUJOL2 and Ana M GIMÉNEZ-ARNAU4
1Department of Dermatology, Hospital del Mar Research Institute, Department of Medicine, Autonomous University of Barcelona/Universitat Autonoma de Barcelona (UAB), 2Department of Dermatology, Hospital del Mar Research Institute, 3Department of Immunology, IMIM Hospital del Mar Research Institute, and 4Department of Dermatology, Hospital del Mar Research Institute. Universitat Pompeu Fabra, Barcelona, Spain
Solar urticaria is a rare photodermatosis with several unknown pathogenic, clinical and therapeutic aspects. This study analysed the clinical and therapeutic features of a long-term follow-up solar urticaria cohort, with a focus on omalizumab management and outcomes, and characterized omalizumab response with the use of the high-affinity immunoglobulin E (IgE) receptor (FcεRI) and the Urticaria Control Test. An observational, unicentric, ambispective study was conducted from 2007 to 2023. Solar urticaria was diagnosed in 41 patients with a median follow-up of 60 months. Thirteen patients were prescribed omalizumab, with a median treatment time of 48 months. A significant decrease in FcεRI baseline levels and subsequent median increase in Urticaria Control Test was evidenced after omalizumab prescription in all patients. Drug survival at 48 months was at 88.9%. Omalizumab stepping-down protocol led to sustained omalizumab discontinuation in only 1 patient. Median basal Urticaria Control Test was lower (p < 0.01) in patients who were prescribed omalizumab and in patients without remission. This study contributes to our knowledge of omalizumab outcomes in real-life clinical practice and highlights the pathogenic importance of IgE-mediated pathways in solar urticaria, where FcεRI emerges as a possible biomarker of omalizumab response.
Key words: chronic urticaria; inducible urticaria; omalizumab; predictor; solar urticaria; treatment.
SIGNIFICANCE
Solar urticaria is a rare type of chronic inducible urticaria with several clinical, laboratory and therapeutic aspects that need further elucidation. This study sheds light on the therapeutic features of solar urticaria in a real-life practice setting, including omalizumab management and outcomes in patients with severe solar urticaria and the emergence of the high-affinity immunoglobulin E receptor as a useful laboratory marker to predict response to omalizumab, which provides further clues to the pathogenesis of this condition.
Citation: Acta Derm Venereol 2024; 104: adv25576. DOI https://doi.org/10.2340/actadv.v104.25576.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Submitted: Nov 8, 2023; Accepted: Nov 17, 2023; Published Jan 8, 2024.
Corr: Ana M Giménez-Arnau, Department of Dermatology, Hospital del Mar Research Institute. Universitat Pompeu Fabra, Passeig Maritim 25-29, ES-08003 Barcelona, Spain. E-mail: anamariagimenezarnau@gmail.com
Competing interests and funding: AMG-A is, or recently was, a speaker and/or advisor for and/or has received research funding from Almirall, Amgen, AstraZeneca, Avene, Celldex, Escient Pharmaceutials, Genentech, GSK, Instituto Carlos III- FEDER, Leo Pharma, Menarini, Mitsubishi Tanabe Pharma, Novartis, Sanofi–Regeneron, Servier, Thermo Fisher Scientific, Uriach Pharma / Neucor, outside the submitted work. David Pesqué benefits from a research grant of Leo-Pharma, outside the submitted work. All other authors have no conflicts of interest to declare.
INTRODUCTION
Solar urticaria (SU) is a rare chronic inducible urticaria (CIndU) which is triggered by different wavelengths of light. The pathogenetic mechanisms implicated in SU are unknown, but the possibility that specific immunoglobulin E (IgE) antibodies triggered by photoallergens could bind mast cells leading to hive formation, in analogy to a type I immediate allergy, has been hypothesized (1, 2). However, the precise cromophores that interact with light to form photoallergens, remain unknown. From a clinical perspective, there is still limited knowledge on the clinical features and natural history of SU (3), which impacts considerably on the quality of life and daily activities of patients (4). In terms of therapy, it has been proposed that half of CIndU patients are antihistamine-resistant even at higher doses (5). In addition, the Urticaria Control Test (UCT) has been suggested as a marker of poorer treatment response in chronic urticaria (6). However, antihistamine responsiveness has not been well characterized in SU. Furthermore, real-life data on the efficacy outcomes of omalizumab in SU is still limited, particularly in long-term follow-up cohorts (7–11). Moreover, there is a lack of studies evaluating biomarkers of response to omalizumab in SU. The role of FcεRI, a suggested predictor of response in chronic spontaneous urticaria (CSU) (12, 13), has not been characterized in SU. In addition, there is no consensus on how to manage the stepping up and down of omalizumab in SU.
The aim of this study is to analyse the clinical features and therapeutic characteristics in a long-term follow-up cohort of patients with SU, with a focus on evaluating the therapeutic management and outcomes, in terms of control and remission, of antihistamines and omalizumab. Furthermore, this study aims to assess predictors of omalizumab initiation, to assess omalizumab response with the characterization of successive FcεRI measurements after drug initiation, and to study predictors of remission.
MATERIALS AND METHODS
Patients
An observational, unicentric, ambispective study of adult patients with a diagnosis of SU was conducted from January 2007 to May 2023 at the Urticaria Unit of Hospital del Mar, Barcelona, Spain, a Urticaria Center of Reference and Excellence (UCARE) centre. As a reference unit, referral depends on specialists, mostly dermatologists. SU was diagnosed with clinical suspicion, photoprovocation to elicit the culprit waveband(s) of light and by ruling out other possible photodermatosis (antinuclear antibodies (ANA), porphyrins study). A total of 41 patients were diagnosed with SU during this period. Clinical and therapeutic variables were collected prospectively at the first visit and during follow-up and transferred to an anonymized database. Variables in relation to photobiology and clinical diagnostic suspicion at referral were collected retrospectively and transferred to an anonymized database. Complementary tests conducted in this study are aligned with real-life clinical practice. FcεRI expression tests were performed in the setting of a specialized centre. Ethics approval for the study was granted by the local Clinical Research Ethics Committee (2012/4913/I). An informed consent was signed by all patients.
Clinical parameters
Demographic data (age, sex, phototype), comorbidities (atopic dermatitis, contact dermatitis, other accompanying chronic urticaria forms, autoimmune diseases and other photodermatoses), clinical characteristics (clinical presentation, time to diagnosis, time of exposition, duration, perception of hardening) were collected prospectively. Photobiological data (type(s) of wavelengths), time of follow-up and referral diagnosis were retrospectively evaluated.
Therapeutic protocols and parameters
Basal UCT was collected for all patients. The use of antihistamines at double and 4-fold doses was evaluated. In accordance with guidelines of chronic urticaria, if no control with 4-fold doses of antihistamines was achieved after 4 weeks, omalizumab was started at 300 mg every 4 weeks. Clinical control of the disease was defined by a UCT ≥ 12 (14). Partial control was defined with UCT between 12 and 15, whereas complete control was achieved when UCT reached 16. Once omalizumab was started, antihistamines were kept, but doses were progressively reduced if complete control was achieved. An evaluation of patients who were using still antihistamines 6 months after initiating omalizumab was performed. If omalizumab had been administered, presence of discontinuation and reasons for discontinuation (remission, inefficacy or adverse effects) as well as stepping up or down omalizumab were evaluated. Since there are no specific guidelines for the stepping up or down of omalizumab in SU, the updosing or stepping-up protocol was based on previous CSU protocols (14). Candidates to follow the step-down protocol should have presented at least 3 months of complete control. If it occurred, dosage was progressively reduced to 300 mg every 6 weeks, and subsequently to 300 mg every 8 weeks. The therapeutic approach to drug discontinuation was different in both groups. In the group treated with antihistamines, when complete control had been maintained for 6 months with antihistamines at the licensed dose, treatment was stopped. Patients with omalizumab should be in complete control after 6 months of treatment with omalizumab at 300 mg every 8 weeks to discontinue the drug. Complete remission for both groups was defined as absence of symptoms for 12 months or more after drug discontinuation. Follow-up every 3–6 months was performed to detect relapses. If relapses occurred, time to relapse was measured in patients of the omalizumab group. Treatment duration of omalizumab and drug survival for omalizumab at 12, 24 and 48 months were evaluated. Finally, in patients treated with omalizumab, UCT and FcεRI were measured basally and then at weeks 4, 8, 12 and 24.
Blood test parameters
All complementary tests were common to the cohort. Baseline tests included total IgE, FCεRI, ANA, IgG anti-thyroid peroxidase (TPO), tryptase, and D-dimer. FcεRI expression in blood basophils was measured by flow cytometry. Standard procedures were followed to perform flow cytometry analyses. 12 FcεRI expression in basophils was assessed by mean fluorescence intensity (MFI). To ensure consistency of analysis, the same investigator processed and analysed all samples. Baseline total IgE in serum and IgG anti-TPO levels in serum were analysed by a chemiluminescence immunoassay with IMMULITE 2000 XPi System (Siemens, Munich, Germany). All other laboratory values were measured by automated analysers in the local central laboratory.
Photobiological study
All patients underwent phototesting according to the consensus protocols published by the Spanish Photobiology Group (15–17). Phototest procedures were performed on the back of patients, using ultraviolet A (UVA) (6 J/cm2), UVB (60 mJ/cm2) and visible light (slide projector) with threshold testing to obtain the minimal urticarial dose (MUD) for each band. Sources of light used were a solar simulator (UVA and UVB) and a slide projector (visible light). Readings were performed immediately, at 10, 30 and 60 min, as well as a late reading 24 h later. If phototesting was negative, a short exposition to natural light was suggested to patients before the consultation to evaluate the flare.
Statistical analysis
Demographic characteristics of patients with CSU were reported using descriptive statistics. Results are expressed as median and interquartile range (IQR) for quantitative variables or number and percentage for qualitative variables. Groups were compared using C2 test of homogeneity (categorical variables) or the Mann–Whitney U test (continuous variables) for the categories of main treatment (only antihistamines/omalizumab), remission (yes/no), dichotomized UCT (≤ 11/ ≥ 12) . If the conditions to apply C2 test were not fulfilled, Fisher’s test was used. A p-value < 0.05 was considered statistically significant. Statistical analyses were performed with Stata-17 (StataCorp, College Station, TX, USA).
RESULTS
Clinical and photobiological features
SU was diagnosed in 41 patients during this period. The cohort presented a median onset at 34.0 years-old, with female predominance (n = 26, 63.4%). Accompanying contact allergic dermatitis, atopic dermatitis and other subtype(s) of CIndU were common comorbidities, whereas the association of CSU or autoimmune disease(s) were uncommon (both below 5%). Median time to reach diagnosis in the cohort was 24 months. At referral to the Urticaria Unit, most patients had been diagnosed with SU, with little referral misdiagnosis (n = 3, 7.3%).
Flares of SU associated hives (n = 41, 100%), itch (n = 39, 95.1%), burning sensation (n = 11, 26.8%), or even angioedema (n = 3, 7.3%). No associated systemic symptoms were noted. Skin symptoms were reported to appear within a median of 5 min after exposition and with a median duration of 60 min.
In terms of photobiological features, patient-referred hardening was an almost constant feature (n = 40, 97.6%). Most patients elicited a positive reaction to photoprovocation (n = 38, 92.7%), with the most common triggering waveband being the combination of UVA and visible light (n = 11, 29.7%). Table I shows in depth clinical and photobiological characteristics of the cohort.
| Clinical characteristics | |
| Age of onset, yeats, median (IQR) | 34.0 (46.0–26.0) |
| Women, n (%) | 26 (63.4) |
| Phototype, n (%) 2 3 4 |
–9 (22.0) –28 (68.2) –4 (9.8) |
| Allergic contact dermatitis, n (%) | 10 (24.4) |
| Chronic inducible urticaria, n (%) | 8 (19.5) |
| Chronic spontaneous urticaria, n (%) | 1 (2.4) |
| Autoimmune disease, n (%) | 2 (4.9) |
| Atopic dermatitis, n (%) | 9 (22.0) |
| Time to diagnosis, months, median (IQR) | 24.0 (48.0–12.0) |
| Diagnostic pitfall, n (%) | 3 (7.3) |
| Hives, n (%) | 41 (100) |
| Itch, n (%) | 39 (95.1) |
| Burning sensation, n (%) | 11 (26.8) |
| Angioedema, n (%) | 3 (7.3) |
| Time to flare (min), median (IQR) | 5.0 (10.0–4.2) |
| Flare duration (min), median (IQR) | 60.0 (90.0–30.0) |
| Photobiological characteristics | |
| Hardening, n (%) | 40 (97.6) |
| UVA, n (%)* | 26 (63.4) |
| UVB, n (%)* | 13 (31.7) |
| Visible light, n (%)* | 29 (70.7) |
| One waveband, n (%) | 16 (39.0) |
| Two or more wavebands, n (%) | 22 (53.7) |
| MUD-UVA (J/cm2), median (IQR) | 5.5 (5.0–6.0) |
| MUD-UVB (mJ/cm2), median (IQR) | 43.0 (74.0–34.0) |
| Laboratory characteristics | |
| IgE, IU/ml, median (IQR) | 136.5 (338.5–50.5) |
| FcεRI, MFI, median (IQR) | 11040 (17230.0–8867.0) |
| Positive antinuclear antibodies, n (%) | 4 (9.8) |
| Positive anti-TPO, n (%) | 4 (9.8) |
| Tryptase, ng/ml, median (IQR) | 3.81 (5.70–2.99) |
| D-dimer, mg/dl, median (IQR) | 235 (360–190) |
| FcεRI: high-affinity IgE receptor; IQR: interquartile range; UVA: ultraviolet A; UVB: ultraviolet B; MUD: minimal urticarial dose; anti-TPO: anti-thyroid peroxidase antibodies. | |
| *Indicates positive reaction to this waveband, independently of reaction to other wavebands. | |
Laboratory characteristics
Median baseline IgE serum level was 136.5 UI/mL (IQR 338.5–50.5 UI/mL). Autoimmunity markers (ANA and anti-TPO) were detected in a small fraction of patients (9.8%). Studies of porphyrins were unremarkable. All other parameters are shown in Table I.
Therapeutic features
The cohort presented a median follow-up of 60.0 months. Photoprotection was used by the vast majority of patients (n = 40, 97.6%). Antihistamines were the first-line treatment in all patients, initially at a 2-fold dose. If this dose was insufficient to reach control, a 4-fold dose was prescribed (n = 18, 43.9%). In antihistamines-resistant SU, omalizumab was commenced (n = 13, 31.7%). During follow-up, 15 patients (15/41, 36.6%) presented remission. Global therapeutic data is found in Table II.
Furthermore, factors related to prescription of omalizumab and to remission were investigated and the only baseline variable that was different between the groups of main treatment (only antihistamines vs omalizumab) and remission (presence vs absence) was basal UCT (p < 0.01, in both). Table III shows the characteristics of patients according to the main treatment, basal UCT (≤ 11/ ≥ 12) and remission.
Analysis of patients treated only with antihistamines
Patients who were treated only with antihistamines had a median treatment of 33.8 (13.7–71.9) months. The number of patients who only required 2-fold dose to reach control was n = 23/28 (82.1%), and an increase to 4-fold dose was seen in only 5 patients. Half of this group of patients (14/28) presented complete remission.
Analysis of patients treated with omalizumab
In the group treated with omalizumab (n = 13), median time of omalizumab treatment was 51.4 (73.1–27.4) months. Omalizumab was initiated between 2015 and 2018 in 5 patients, in 2019 in 5 patients, and between 2020 and 2021 in 3 patients. Median basal UCT equalled 6 (8–4). All patients started at a dose of 300 mg every 4 weeks. Drug survival of omalizumab at 12, 24 and 48 months was 100% (13/13), 100% (12/12) and 88.9% (8/9), respectively. In this cohort, only 2 patients discontinued omalizumab. Reasons for discontinuation were 1 complete remission and 1 loss of follow-up. Stepping up omalizumab up to 450 mg every 4 weeks was necessary in 3 patients with a subsequent partial/complete control. No patient needed updosing to 600 mg every 4 weeks. Stepping down omalizumab was essayed in 8 patients, but only 5 patients could totally discontinue omalizumab. Four of these 5 patients presented relapses of SU after omalizumab discontinuation with a median of 7 (8.8–3.8) months. Patients with an interval prolongation of omalizumab are significant in the cohort and correspond to patients who either relapsed or could not follow completely the step-down protocol due to worsening of control. In total, 4 patients are still being treated at 300 mg every 6 weeks and 3 at 300 mg every 8 weeks. Use of antihistamines at 6 months was seen in only 5/13 patients at doses of licensed dose (1/5), 2-fold (3/5) or 3-fold (1/5).
After omalizumab initiation, 11 patients had UCT and FcεRI measurements at weeks 4, 8, 12 and 24. These measurements could only be done in 11/13 patients, since 2/13 did domiciliary treatment and were unable to do output follow-up with the desired frequency. In terms of UCT, a fast and marked increase of the median values was evidenced, indicating an improvement of the control of symptoms of patients treated with omalizumab. In fact, achievement of UCT ≥ 12 at week 4 was 4/11, with an increase at weeks 8, 12 and 24 with 9/11, 9/11 and 11/11, respectively. At week 24, 7/11 patients had a UCT = 16, indicating complete control. Furthermore, change in FcεRI expression in basophils after initiation of omalizumab, in the same timeline, showed a clear-cut decrease from baseline at week 4, which was sustained until week 24. No adverse effects of omalizumab were evidenced in any patient. Figs 1 and 2 show the median values of UCT and percentage decrease from baseline in FcεRI expression, respectively.
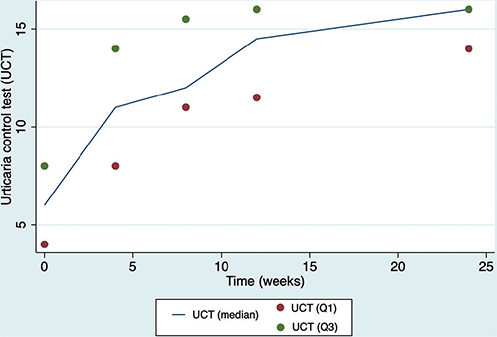
Fig. 1. Urticaria Control Test (UCT) variation (median and interquartile range) of patients after initiation of omalizumab at weeks 0, 4, 8, 12 and 24. Q1 (first quartile); Q3 (third quartile).
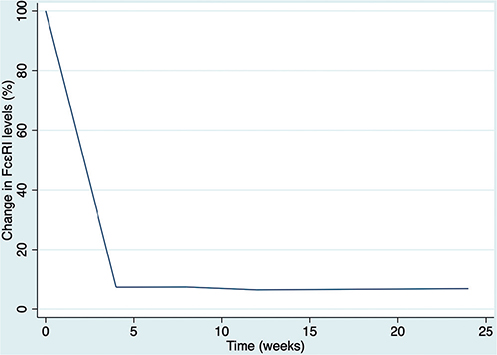
Fig. 2. Percentage reduction in high-affinity immunoglobulin E (IgE) receptor (FcεRI) baseline levels in patients after omalizumab initiation at weeks 0, 4, 8, 12 and 24.
DISCUSSION
Demographic features of the cohort are in line with previous research (18–20), reinforcing that the condition is most commonly encountered among young, adult women. In terms of comorbidities, this study also supports that atopic dermatitis and other CIndU may be more frequent in SU. Furthermore, a significant number of patients had history of allergic contact dermatitis, which has not been described in previous publications. In contrast to CSU, the association of autoimmune disorders was rare, and only 1 patient presented with CSU and SU, within different time-periods. No other photodermatoses were evidenced in this group of patients, in contrast with previous literature (21). The median time to diagnosis for patients with SU was 2 years; however, the referral misdiagnoses among specialists were low. Despite the factors that contributed to the diagnostic delay were not evaluated, the high proportion of referral diagnostic accuracy may reflect that specialists (dermatologists/allergologists) are familiar with SU. The clinical features of SU and the photoprovocation results are similar to previous studies, possibly strengthening the representativity of this cohort of patients with SU. In terms of laboratory features, baseline blood tests showed an elevated median IgE (136.5, IQR 338.5–50.5). Inflammatory markers were mostly unremarkable in the cohort and the serological presence of autoimmunity was scarce. Despite there is a limited number of studies on the laboratory baseline features of SU, these results suggest the absence of an autoimmune and/or inflammatory serological background, as has been suggested for other types of chronic urticaria, such as autoimmune CSU (22).
Therapeutic characteristics in the current study indicate that a significant number of patients is properly controlled with 2-fold dose of antihistamines, without further therapeutic requirements during follow-up. With a median follow-up of 60 months, SU presented sustained complete remission in approximately one-third of the patients. Most patients who presented complete remission (14/15) had previously presented control only with antihistamines. In addition, a lower basal UCT was a significant differential baseline clinical feature (p < 0.01) for omalizumab administration and for remission, possibly highlighting both its importance in daily clinical practice and its role as a possible predictor of lack of responsiveness to antihistamines and subsequent omalizumab prescription, as well as more persistent urticaria.
In terms of the clinical and laboratory follow-up of patients who started with omalizumab, the study of UCT and FcεRI has revealed a fast clinical response in 11 patients, accompanied by a sharp baseline reduction in FcεRI. The observation of a reduction in the FcεRI in patients treated with omalizumab has been made before for other conditions (allergic rhinitis, allergic asthma and CSU) (12, 23, 24). The hypothesis underlying this observation is based on the initial lowering of IgE, which is followed by a reduction in FcεRI. In fact, an IgE-free FcεRI may be structurally unstable, which could lead to internalization and degradation (25, 26). To our knowledge, this investigation is the most extensive evaluation of FcεRI in patients with SU to date. Previous publications have highlighted that SU symptoms are triggered with the participation of an IgE pathway (1–3, 7). The association of clinical improvement with lowering FcεRI in omalizumab responders may reinforce the importance in pathophysiology of an IgE type 1 hypersensitivity in SU in real-life clinical practice. In terms of clinical response, these results show that response to omalizumab in a real-life setting is rapidly perceived by patients, according to UCT measurements. Therefore, this study gives value to the role of omalizumab when failure to antihistamines occur. These results are in line with previously published studies (27, 28), highlighting that partial/total control with omalizumab may be achieved relatively rapidly after initiation of therapy. It is important to note that the initiation of omalizumab was accompanied by a sharp decrease in the use of antihistamines after 6 months of treatment, which further reveals the clinical benefits of omalizumab. In regard to non-responders to omalizumab or late responders to omalizumab signalled in the literature (11, 29), this study has failed to observe these situations, even if some cases of up-dosing were evidenced during follow-up. However, results also suggest that omalizumab is not curative, but rather treats the symptoms, and that patients tend to present with flares or relapses if the dose is lowered or the treatment stopped, which results in long-term therapy schemes. It has been proposed that patients with presence of CIndU have a lower probability of remission and, thus, a longer need for omalizumab treatment, which can explain longer drug survival related to well-controlled disease activity (30), as also seen our case. Furthermore, it is important to enhance the therapeutic difficulty linked to the loss of clinical improvement when omalizumab is stopped (8, 28).
Limitations
Limitations of this study are related to its unicentric nature, with a reduced number of patients. Despite this, the cohort size is still relevant, taking into account previous literature and the very low prevalence of this disease.
Conclusion
The analysis of this cohort suggests common clinical and photobiological features in patients with SU without particular inflammatory or autoimmune laboratory features. In terms of treatment, baseline UCT was the only clinical or laboratory baseline feature that was significantly lower in patients who were later treated with omalizumab and also in the group of patients who did not present remission. The probability to reach complete remission seemed higher in patients who responded to antihistamines. In this regard, this study could suggest the presence of a different natural course and prognosis of SU depending on the initial response to antihistamines, with shorter disease courses for this group. If omalizumab was initiated, clinical response was rapid and was accompanied by a significant percentage reduction in baseline FcεRI levels, reinforcing a significant pathogenic role of IgE-mediated pathways through the observation of treatment response. In addition, it suggests FcεRI as a possible biomarker of response to omalizumab in patients with SU. Despite being a safe treatment and reaching complete control in a significant number of patients, omalizumab was not curative and loss of control or relapses were seen if the dose was lowered or stopped.
ACKNOWLEDGEMENTS
This work was carried out in the Department of Medicine of Autonomous University of Barcelona, Barcelona, Spain.
Ethics approval for the study was granted by the local Clinical Research Ethics Committee (2012/4913/I). An informed consent was signed by all patients.
REFERENCES
- Goetze S, Elsner P. Solar urticaria. J Dtsch Dermatol Ges 2015; 13: 1250–1253.
- McSweeney SM, Sarkany R, Fassihi H, Tziotzios C, McGrath JA. Pathogenesis of solar urticaria: Classic perspectives and emerging concepts. Exp Dermatol 2022; 31: 586–593.
- McSweeney SM, Kloczko E, Chadha M, Sarkany R, Fassihi H, Tziotzios C, et al. Systematic review of the clinical characteristics and natural history of solar urticaria. J Am Acad Dermatol 2023; 89: 138–140.
- Haylett AK, Koumaki D, Rhodes LE. Solar urticaria in 145 patients: assessment of action spectra and impact on quality of life in adults and children. Photodermatol Photoimmunol Photomed 2018; 34: 262–268.
- Yu M, Terhorst-Molawi D, Altrichter S, Hawro T, Chen YD, Liu B, et al. Omalizumab in chronic inducible urticaria: a real-life study of efficacy, safety, predictors of treatment outcome and time to response. Clin Exp Allergy 2021; 51: 730–734.
- Maurer M, Raap U, Staubach P, Richter-Huhn G, Bauer A, Oppel EM, et al. Antihistamine-resistant chronic spontaneous urticaria: 1-year data from the AWARE study. Clin Exp Allergy 2019; 49: 655–662.
- Maurer M, Church MK, Gonçalo M, Sussman G, Sánchez-Borges M. Management and treatment of chronic urticaria (CU). J Eur Acad Dermatol Venereol 2015; 29: 16–32.
- Aubin F, Avenel-Audran M, Jeanmougin M, Adamski H, Peyron JL, Marguery MC, et al. Omalizumab in patients with severe and refractory solar urticaria: a phase II multicentric study. J Am Acad Dermatol 2016; 74: 574–575.
- Maurer M, Metz M, Brehler R, Hillen U, Jakob T, Mahler V, et al. Omalizumab treatment in patients with chronic inducible urticaria: a systematic review of published evidence. J Allergy Clin Immunol 2018; 141: 638–649.
- Snast I, Kremer N, Lapidoth M, Enk CD, Tal Y, Rosman Y, et al. Omalizumab for the treatment of solar urticaria: case series and systematic review of the literature. J Allergy Clin Immunol Pract 2018; 6: 1198–1204.e3.
- Navarro-Triviño FJ, Prados-Carmona A, Aguilera J, de Gálvez MV, Ruiz-Villaverde R. Treatment of refractory solar urticaria: could dupilumab fill the current gap? J Dtsch Dermatol Ges 2023; 21: 652–653.
- Deza G, Bertolín-Colilla M, Pujol RM, Curto-Barredo L, Soto D, García M, et al. Basophil FcεRI expression in chronic spontaneous urticaria: a potential immunological predictor of response to omalizumab therapy. Acta Derm Venereol 2017; 97: 698–704.
- Moñino-Romero S, Kolkhir P, Ohanyan T, Szépfalusi Z, Weller K, Metz M, et al. Elevated baseline soluble FcεRI may be linked to early response to omalizumab treatment in chronic spontaneous urticaria. J Eur Acad Dermatol Venereol 2024; 38: 167–174.
- Spertino J, Curto-Barredo L, Rozas-Muñoz E, Figueras-Nart I, Gimenez-Arnau A, Serra-Baldrich E, et al. Algorithm for treatment of chronic spontaneous urticaria with omalizumab. Actas Dermosifiliogr (Engl Ed) 2018; 109: 771–776.
- De Argila D, Aguilera J, Sánchez J, García-Díez A. Study of idiopathic, exogenous photodermatoses, part II: photobiologic testing. Actas Dermosifiliogr 2014; 105: 233–242.
- Pérez-Ferriols A, Aguilera J, Aguilera P, de Argila D, Barnadas MA, de Cabo X, et al. Determination of minimal erythema dose and anomalous reactions to UVA radiation by skin phototype. Actas Dermosifiliogr 2014; 105: 780–788.
- Magerl M, Altrichter S, Borzova E, Giménez-Arnau A, Grattan CE, Lawlor F, et al. The definition, diagnostic testing, and management of chronic inducible urticarias – the EAACI/GA(2) LEN/EDF/UNEV consensus recommendations 2016 update and revision. Allergy 2016; 71: 780–802.
- Morgado-Carrasco D, Fustà-Novell X, Podlipnik S, Combalia A, Aguilera P. Clinical and photobiological response in eight patients with solar urticaria under treatment with omalizumab, and review of the literature. Photodermatol Photoimmunol Photomed 2018; 34: 194–199.
- Snast I, Lapidoth M, Uvaidov V, Enk CD, Mazor S, Hodak E, et al. Real-life experience in the treatment of solar urticaria: retrospective cohort study. Clin Exp Dermatol 2019; 44: e164–e170.
- Photiou L, Foley P, Ross G. Solar urticaria – an Australian case series of 83 patients. Australas J Dermatol 2019; 60: 110–117.
- Kishimoto I, Uetsu N, Tanimura H, Fujii H, Okamoto H. Solar urticaria with a wide action spectrum from UVB to visible light complicated with UVA-induced polymorphous light eruption. Photodermatol Photoimmunol Photomed 2017; 33: 172–175.
- Pesqué D, March-Rodríguez Á, Curto-Barredo L, Soto D, Gimeno R, Pujol RM, et al. Autoimmune diseases and low baseline immunoglobulin E in chronic spontaneous urticaria: a clinical and therapeutic prospective analysis in real clinical practice. J Allergy Clin Immunol Pract 2023; 11: 3763–3771.e5
- Lin H, Boesel KM, Griffith DT, Prussin C, Foster B, Romero FA, et al. Omalizumab rapidly decreases nasal allergic response and FcεRI on basophils. J Allergy Clin Immunol 2004; 113: 297–302.
- Oliver JM, Tarleton CA, Gilmartin L, Archibeque T, Qualls CR, Diehl L, et al. Reduced FcεRI-mediated release of asthma-promoting cytokines and chemokines from human basophils during omalizumab therapy. Int Arch Allergy Immunol 2010; 151: 275–284.
- Wright JD, Chu HM, Huang CH, Ma C, Chang TW, Lim C. Structural and physical basis for anti-IgE therapy. Sci Rep 2015; 5: 11581.
- Prussin C, Griffith DT, Boesel KM, Lin H, Foster B, Casale TB. Omalizumab treatment downregulates dendritic cell FcεRI expression. J Allergy Clin Immunol 2003; 112: 1147–1154
- Kocatürk E, Can PK, Akbas PE, Copur M, Degirmentepe EN, Kızıltac K, et al. Management of chronic inducible urticaria according to the guidelines: a prospective controlled study. J Dermatol Sci 2017; 87: 60–69.
- Morgado-Carrasco D, Giácaman-Von der Weth M, Fustá-Novell X, Podlipnik S, Pérez-Ferriols A, Aguilera P. Clinical response and long-term follow-up of 20 patients with refractory solar urticaria under treatment with omalizumab. J Am Acad Dermatol 2023; 88: 1110–1111.
- Vollono L, Bianchi L, Piccolo A, Mazzilli S, Campione E, Diluvio L Good things come to those who wait: Successful response of solar urticaria to omalizumab after 1 year of treatment. Photodermatol Photoimmunol Photomed 2020; 36: 408–411.
- Spekhorst LS, van den Reek JMPA, Knulst AC, Röckmann H. Determinants of omalizumab drug survival in a long-term daily practice cohort of patients with chronic urticaria. Allergy 2019; 74: 1185–1187.