ORIGINAL REPORT
Prognostic Factors Predicting Remission Following Rituximab Therapy for Pemphigus Vulgaris
Tal RAVIV1, Keren PEVZNER1, Aviv BARZILAI1,2, Felix PAVLOTSKY1,3 and Sharon BAUM1
1Department of Dermatology, Sheba Medical Center, Tel HaShomer, Ramat Gan, affiliated to the Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel2Institute of Pathology, Sheba Medical Center, Tel HaShomer, Ramat Gan, and 3Phototherapy Unit, Department of Dermatology, Sheba Medical Center, Tel HaShomer, Ramat Gan, Israel
Abstract
Pemphigus vulgaris is a chronic autoimmune blistering disease with significant morbidity. Rituximab, approved as its first-line treatment, effectively induces remission. However, few studies have analysed the prognostic factors for improved rituximab outcomes. Therefore, this study aimed to identify such factors in a cohort of pemphigus vulgaris patients. A total of 142 pemphigus vulgaris patients treated with rituximab at Sheba Medical Center, with data encompassing demographics, comorbidities, disease characteristics, and treatment outcomes, were retrospectively examined. Results showed that 61.9% of patients previously treated with mycophenolate mofetil achieved partial remission, whereas only 34.7% achieved complete remission. Patients with diabetes mellitus exhibited a significantly shorter median time to relapse compared with those without. Patients with a disease duration ≤ 16 months before rituximab therapy exhibited a shorter median time to relapse. Moreover, previous dapsone treatment extended time to relapse. Notably, sex, age at symptom onset and rituximab therapy, ethnicity, comorbidities, skin involvement, weight, rituximab dosing protocol, and other variables were not statistically significant between the complete remission and partial remission groups. These findings highlight the influence of specific patient characteristics and treatment histories on response to rituximab and time to relapse in pemphigus vulgaris patients. Understanding these factors can aid clinicians in predicting treatment outcomes and selecting the appropriate patient population for rituximab therapy.
SIGNIFICANCE
Pemphigus vulgaris is a chronic autoimmune blistering disease that manifests as cutaneous and mucous membrane blisters and erosions. First-line therapy with rituximab has been proven to be effective in inducing remission. Due to the few studies published, this study investigated possible prognostic factors for remission post-rituximab therapy in a cohort of pemphigus vulgaris patients. The findings revealed that a history of diabetes mellitus and a short disease duration before rituximab therapy were associated with a short time to relapse; however, previous dapsone treatment before rituximab therapy extended the time to relapse. These results may serve as a critical resource for clinicians.
Key words: pemphigus vulgaris; prognosis; rituximab.
Citation: Acta Derm Venereol 2025; 105: adv27140. DOI: https://doi.org/10.2340/actadv.v105.27140.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Nov 19, 2023; Accepted after revision: Sep 24, 2024. Published: Jan 3, 2025
Corr: Tal Raviv, MD, Department of Dermatology, Sheba Medical Center, Tel HaShomer, Ramat Gan, Israel. E-mail: tal.raviv7@gmail.com
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Pemphigus vulgaris (PV) is a chronic autoimmune blistering disease characterized by the formation of autoantibodies against intercellular adhesion proteins, which generate an intraepidermal split, manifesting clinically as cutaneous and mucous membrane blisters and erosions (1). If untreated, PV can induce possible complications, including dehydration, undernutrition/weight loss, and possible mortality from secondary infections (2).
Prompt systemic corticosteroid therapy is crucial at disease onset and flare-ups to alleviate symptoms and induce remission, which is maintained using steroid-sparing adjuvant treatments that induce general immunosuppression (3). Targeted therapy with rituximab, a monoclonal anti-CD20 antibody against B lymphocytes, originally indicated for non-Hodgkin’s lymphoma (NHL), was used off-label for PV before it gained approval as a first-line therapy in 2018 (USA) and 2019 (EU) (4). Rituximab has demonstrated efficacy in inducing disease remission in PV patients, with studies showing disease control in 90–95% of PV patients within ≤ 6 weeks of treatment initiation. Complete remission (CR) was observed within 3–4 months, whereas most patients remained on minimal steroid or immunosuppressive therapy (5). Nosrati et al. (6) also reported a remission rate of 74% at 5.5 months after the first rituximab cycle, whereas Sharma et al. (7) reported a CR rate of 83.6% at 5 weeks.
However, despite these results, relapse rates have been observed ranging from 10% at 12 months, to 42% at 18 months, and 55% at 24 months (8). Some patients may experience relapse years later, whereas others might be non-responsive to treatment.
Few studies have analysed prognostic factors for improved outcomes with rituximab treatment. In 2019, Kushner et al. identified factors associated with CR in PV patients post-rituximab therapy. Increasing age (> 65 years) significantly elevated the odds of achieving CR off therapy (CROT), a body mass index over 35 decreased the odds of achieving CROT, and lymphoma dosing correlated with 2.7 fold higher CROT likelihood than rheumatoid arthritis (RA) dosing (9). Saha et al. (10) supported these findings: younger onset age was associated with a worse prognosis regarding disease duration, and Indo-Asian patients exhibited significantly longer disease duration than White-British patients. A retrospective study of 29 patients noted no relapses with the oncologic dose group (lymphoma protocol), compared with the 50% observed in the rheumatologic dose group, further strengthening the findings of Kushner et al. (11). In 2017, a retrospective study by Kim et al. reported that CR rates at 6 months following rituximab treatment were significantly higher with 3–4 infusions per cycle than with 2 infusions per cycle (each infusion dose at 375 mg/m2) (12). Lunardon et al. (13) reported statistically significantly better outcomes with early rituximab treatment. Cho et al. (14) reported that patients with mucosal lesions exhibited increased relapse risk with rituximab treatment by 4.626 times compared with those without, affirming mucosal involvement as a negative predictor of remission in PV, with or without rituximab treatment.
Given the limited studies on prognostic factors for improved outcomes with rituximab therapy, in this study we aimed to investigate possible prognostic factors for remission in rituximab-treated PV patients.
MATERIALS AND METHODS
This retrospective study included 142 PV patients treated with rituximab at the Department of Dermatology and Dermatology Outpatient Clinic, Sheba Medical Center, Israel. Patient data collected between June 2009 and May 2023 were retrieved from a computerized medical records database. PV diagnosis relied on clinical findings of cutaneous and/or mucosal blisters or erosions consistent with the disease. Confirmatory histopathology demonstrated suprabasal epidermal acantholysis and evidence of intercellular IgG deposits (with or without C3 binding) in the epidermis/epithelium, with a net-like pattern as observed through direct immunofluorescence.
Before rituximab gained FDA approval as a first-line therapy for moderate-to-severe pemphigus vulgaris in 2018 (US) and 2019 (EU), dosing regimens standardly used for NHL and subsequently for RA were implemented in PV (15). In our cohort, dosing regimens changed with time, following prevalent practices. From 2009 to 2013, the NHL regimen comprised weekly intravenous infusions of 375 mg/m2 for 4 consecutive weeks. Since 2014, patients have received the RA regimen, consisting of 2 x 1,000 mg infusions spaced 2 weeks apart. Before treatment initiation, all patients received a detailed explanation concerning the drug (including infection prevention and control measures), underwent clinical and laboratory examinations, and were administered vaccinations/preventive treatments as necessary. All patients received infusions at the Dermatology Day Care Unit in the Department of Dermatology, Sheba Medical Center (16). During follow-up, patients were examined at least once in 3 months by 2 dermatology specialists who documented their clinical status.
The collected data encompassed patient demographics (sex, year of birth, and ethnicity), weight, initial clinical presentation, comorbidities (before PV treatment), and clinical history, including cutaneous/mucosal disease involvement, degree of skin involvement, previous adjuvant therapies, and disease duration before rituximab treatment. Information on the first rituximab course was retrieved, including treatment dates and dosing, clinical response, time to remission, and TTR post-course. Treatment response was defined as complete response (CR), partial response (PR), or no response (NR). The CR and PR groups were further subdivided into CR on therapy (CR ON), CR off therapy (CR OFF), PR on therapy (PR ON), and PR off therapy (PR OFF). “Therapy” was defined as prednisone treatment at a dose of ≤ 10 mg, according to consensus guidelines. NR indicated treatment failure with continued lesion development, extension of old lesions, or failure to heal despite 3 weeks of corticosteroid therapy (0.75–1 mg/kg/day prednisone). A relapse or flare-up was defined as the appearance of ≥ 3 new lesions per month that did not spontaneously heal within 1 week or the extension of established lesions in previously controlled disease cases (17). Another endpoint assessed was the TTR, measured in months from the first day of the rituximab course to the relapse date. The studied rituximab course was the first ever administered to the patients.
This study adhered to the principles of the Declaration of Helsinki and was approved by the Institutional Review Board (reference number 7172-09-SMC). Informed consent was not required owing to the retrospective nature of the study.
Statistical analysis
Continuous variables are described as means and standard deviations (SD), and categorical variables are presented as proportions and percentages. A comparative analysis was performed between CR and PR groups using Student’s t-test for continuous variables and Pearson’s χ2 test for categorical variables. An additional comparative analysis was performed between CR OFF, CR ON, PR OFF, and PR ON subgroups using the ANOVA test. Time to first relapse was presented using Kaplan–Meier curves, and p-values were calculated using the log-rank test and Cox model for binary and continuous variables, respectively. The multivariable Cox regression model included baseline parameters of sex, age, and variables significant in the univariate analysis. All statistical tests were two-tailed, and p-values < 0.05 were considered statistically significant. Data were analysed using R software (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
In the cohort of 142 patients, 3 NR patients were excluded from the statistical calculations in the univariate analysis (Tables I–III) and the Kaplan–Meier curves representing the TTR (Figs 1–3). These 3 patients did not achieve remission by definition and, therefore, did not experience a relapse. Consequently, only the CR and PR groups were subjected to further analyses, leading to a statistical cohort comprising 139 patients.
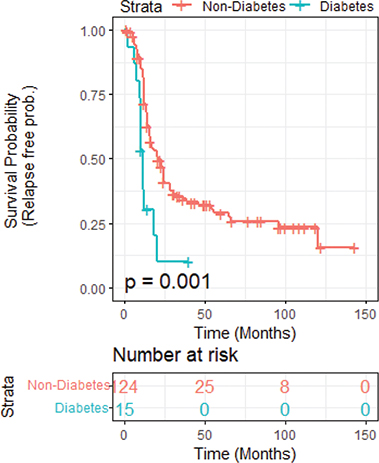
Fig. 1. Kaplan–Meier curve showing time to first relapse following rituximab therapy in pemphigus vulgaris patients with a history of diabetes mellitus.
Patient demographics and clinical characteristics are listed in Table I. Regarding sex distribution, the male-to-female ratio was 0.71:1, distributed as 59 males (41.55%) and 83 females (58.45%). Half of the patients identified as Ashkenazi (50.70%), and approximately one-third were Sephardic (37.32%). Owing to subjective definitions and variability associated with the term “mixed” background, 15 patients falling under this category were excluded from the statistical analysis. Similarly, 1 patient from an Arabic background, owing to the small sample size, was also excluded. The mean age at PV symptom onset was 50.3 years, whereas the mean age at first rituximab therapy was 56.8 years. One-third of the cohort (35.21%) exhibited cardiovascular comorbidities, including hypertension, ischaemic heart disease, and/or dyslipidaemia. One-tenth (10.56%) of the patients were diagnosed with diabetes mellitus (DM), and 9.15% with thyroid disease upon presentation. Regarding PV disease involvement, 71.13% exhibited skin and mucosal involvement, whereas 26.06% displayed mucosal involvement exclusively. Four patients with solely skin involvement were excluded from the statistical analysis because of the small sample size.
Responses to rituximab therapy according to demographics and clinical variables are presented in Table I. Most patients previously treated with mycophenolate mofetil (MMF) achieved PR (61.9%), whereas only 34.7% achieved CR (p = 0.0349). Following stratification into the subgroups CR OFF, CR ON, PR OFF, and PR ON, previous treatment with MMF remained a statistically significant parameter (p = 0.044). Similarly, regarding patients who had undergone plasmapheresis, a higher proportion achieved PR (14.3%) than those who achieved CR (1.7%) (p = 0.0265). Following the same stratification into the above subgroups, plasmapheresis remained statistically significant (p = 0.00374). In addition, the degree of skin involvement measured per patient was also statistically significant (p = 0.0188). However, sex, age at symptom onset and rituximab therapy, ethnicity, comorbidities, weight, rituximab dosing protocol, and other variables (Table I) were not statistically significant between the CR and PR groups.
Table II displays the median TTR calculated according to the binary demographic and clinical variables. Patients with a history of DM exhibited significantly shorter median TTR (11 months) than those without this comorbidity (21 months) (p = 0.001). Kaplan–Meier curves depicting this comparison are shown in Fig. 1.
Subanalysis of the DM patient group into those on and off steroid therapy showed that steroid therapy did not influence this finding, DM as a comorbidity remained statistically significant, regardless of concomitant steroid therapy (p = 0.002). Furthermore, patients who received prior adjuvant treatment with dapsone demonstrated a significantly longer TTR (36 months) post-rituximab therapy than patients who did not receive dapsone (16 months) (p = 0.025). The Kaplan–Meier curve illustrating this comparison is shown in Fig. 2. Student’s t-test was performed to compare the initial disease severity of patients who received dapsone vs those who did not. Disease severity, depicted in the number of cutaneous areas involved, was not statistically significant between the groups (p = 0.496). The other parameters (Table II) did not exert a statistically significant influence on TTR.
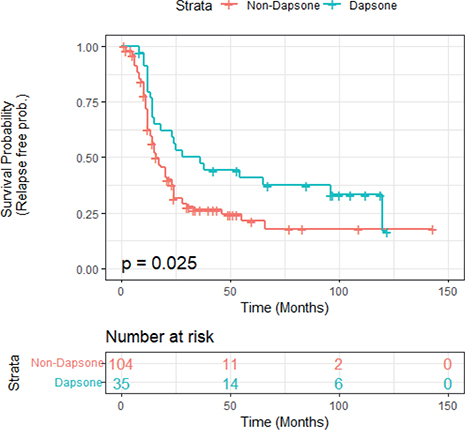
Fig. 2. Kaplan–Meier curve showing time to first relapse following rituximab therapy in pemphigus vulgaris patients previously treated with dapsone.
Table III displays the median TTR calculated for continuous demographic and clinical variables. The only statistically significant parameter was disease duration before rituximab therapy. This parameter is further illustrated in Fig. 3, where it is dichotomized into 2 groups: patients with a disease duration ≤ 16 months (median disease duration for the full cohort) and those with a disease duration of ˃16 months before rituximab therapy. Patients with a shorter disease duration (≤ 16 months) exhibited a shorter TTR than patients with a longer disease duration (p = 0.041). The Kaplan–Meier curve depicting this comparison is shown in Fig. 3.
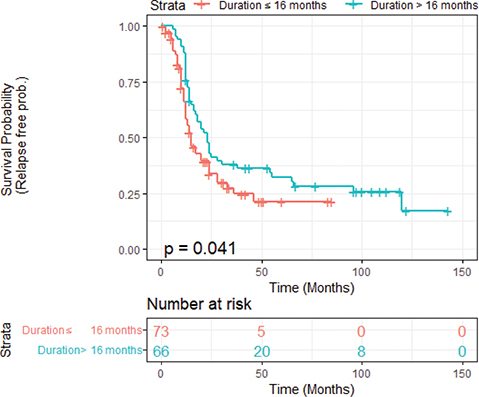
Fig. 3. Relapse-free probability based on disease duration prior to rituximab therapy.
Multivariate Cox regression analysis was conducted for the 3 statistically significant variables influencing TTR: DM, prior dapsone treatment, and the disease duration before rituximab, along with sex and age at the start of the rituximab course. The hazard ratio was 2.86 for patients with DM (confidence interval [CI], 1.49–5.5; p = 0.002), 0.61 for patients with prior dapsone treatment (CI, 0.37–0.997; p = 0.0048), and 0.79 for the disease duration before rituximab treatment (CI, 0.63–0.98; p = 0.03) (Table IV).
DISCUSSION
This retrospective study, conducted at a prominent tertiary centre in Israel, offers valuable insights into the prognostic factors associated with remission in rituximab-treated PV patients.
Comorbidities
Pemphigus is often associated with other diseases. For instance, Parameswaran et al. indicated a higher incidence of autoimmune thyroid diseases, RA, and type 1 DM in pemphigus patients than in the general population (18). In a Spanish hospital-based registry encompassing 1,950 PV patients, hypertension (40.19%) and DM(28.57%) emerged as predominant comorbidities, and thyroiditis, among others, was recorded in 0.3% of cases (19). In our study, approximately one-third of the cohort exhibited cardiovascular comorbidities (35.21%), including hypertension, ischaemic heart disease, and/or dyslipidaemia. Additionally, 10.56% of patients had DM, and 9.15% had thyroid disease at the time of presentation. Given the consistent reports, these comorbidities should be considered during the planning and monitoring of PV treatment. This is especially relevant when tapering corticosteroid therapy. For instance, a mode of prevention/exacerbation, such as routine monitoring of glucose levels and blood pressure, coupled with early intervention when values are out of range, can help mitigate the impact of these comorbidities on PV patients.
Previous adjuvant therapies
Upon evaluating the response to rituximab therapy based on previous adjuvant treatments, interesting patterns were observed. Patients previously treated with MMF achieved PR more frequently (61.9%) than CR (34.7%), suggesting that prior MMF therapy may be associated with a slightly reduced likelihood of achieving CR with rituximab. Conversely, in a previous study on repeated rituximab courses in PV patients, we observed reduced relapse rates upon completion of rituximab cycles in patients previously treated with MMF compared with those previously treated with other adjuvants (p = 0.001) (8). Although the endpoint calculated differed, MMF was associated with a positive disease outcome following rituximab therapy. Conversely, in the current study, MMF was identified as a negative predictor of rituximab success (at the standard dosing protocol of 2g/day). A potential explanation for this finding is the robust immunosuppressive effect of MMF on the disease, which might have led to a state of disease exhaustion before rituximab treatment. Similarly, patients who underwent plasmapheresis before rituximab treatment exhibited a higher proportion of PR (14.3%) than CR (1.7%). However, it is important to approach the significance of this finding with caution, given the limited sample size of patients who underwent plasmapheresis. In contrast, a study involving 155 PV patients treated with a single cycle of rituximab reported that adjuvant plasma exchange or immunoadsorption was associated with an extended TTR (20).
Time to relapse
The analysis of TTR following rituximab therapy revealed significant associations with specific variables. Patients with DM exhibited a significantly shorter TTR (11 months) than those without (21 months). All but 1 patient with DM had non-insulin-dependent diabetes mellitus (NIDDM), which was diagnosed before corticosteroid treatment initiation. This finding suggests that DM may negatively affect long-term remission achieved with rituximab. Notably, there are no previous analyses of diabetes as a prognostic factor for rituximab response in PV. One plausible explanation for our finding could be attributed to the known impaired wound healing and immune responses observed in diabetic patients, which may negatively affect the effectiveness of rituximab in managing the cutaneous wounds associated with PV.
Patients with prior adjuvant treatment with dapsone (at an initial dose of 50–100 mg/day and continued at 100 mg/day) exhibited a significantly longer TTR (36 months) than those without prior dapsone treatment (16 months). This finding suggests that dapsone treatment may have a positive effect on the maintenance of remission post-rituximab therapy. Previous studies have not explored previous adjuvant treatments as prognostic factors in the rituximab response. Theoretically, one could hypothesize that patients who had received prior dapsone treatment in our cohort might have presented with initially milder disease severity, given that dapsone, unlike other immunosuppressive alternatives, is normally administered to individuals with milder PV manifestations. Therefore, following this assumption, these patients would demonstrate a longer disease-free period than patients who had received other immunosuppressive adjuvants. However, Student’s t-test was performed to investigate this theory and it proved otherwise: there was no statistical difference in the total number of skin areas involved, meaning the 2 groups were not statistically different in terms of initial clinical severity. This disproves the theory that dapsone might have been administered to clinically milder patients. Further research should be conducted to inspect dapsone’s effect as a previous adjuvant treatment to rituximab therapy. The multivariate Cox regression analysis further confirmed the association between DM and a shorter TTR, as well as the influence of prior dapsone treatment on a longer TTR.
Another significant finding was the influence of disease duration preceding rituximab treatment on TTR. Patients with shorter disease duration (< 16 months) exhibited a shorter TTR, although the p-value (p = 0.054) indicated borderline significance. This finding suggests that initiating rituximab therapy earlier in the disease course may be associated with earlier relapse. This discovery is inconsistent with pertinent published studies. For instance, a recent retrospective study involving 99 PV patients revealed decreased remission rates associated with increased time to rituximab treatment (21). Furthermore, 2 retrospective studies on PV patients by Balighi et al. demonstrated that early administration of rituximab in the treatment of pemphigus results in better outcomes, including a higher remission rate, a longer disease-free period, a lower relapse rate, and a significant reduction in the requirement for corticosteroids and other immunosuppressants (22, 23). Similarly, Amber et al. (20) and Anandan et al. (24) showed that increased disease duration before rituximab administration correlated with failure to achieve CR and a significantly increased relapse rate. This finding is attributable to 2 possible reasons. First, regarding the natural course of PV, exacerbations occur mostly in the first 2 years, after which disease activity decreases with time (25). Second, it is assumed that patients with prolonged disease duration before rituximab also received prior adjuvant therapies, potentially contributing to better outcomes owing to overall immunosuppression. This emphasizes the importance of recently reported maintenance regimens involving subsequent rituximab administration every 6–12 months following the initial treatment (26, 27). Alternatively, to prevent prolonged B-cell depletion, treatment during exacerbations aligns with the notion that repeated rituximab courses prolong the remission period (8). However, the precise modality awaits further elucidation through randomized controlled studies.
Prior adjuvant dapsone treatment increased the remission period post-rituximab therapy. Conversely, DM may negatively affect the remission period in patients treated with rituximab. Notably, patient sex, age at symptom onset and at rituximab therapy, ethnicity, other comorbidities, degree of skin involvement, weight, and rituximab dosing protocol did not serve as prognostic factors for predicting remission following rituximab therapy. Overall, this study highlights the importance of considering specific factors in the management of PV and the selection of appropriate treatment strategies. Understanding these factors can aid clinicians in predicting treatment outcomes, selecting the appropriate patient population for rituximab therapy, and providing patients with up-to-date information on the success and limitations of rituximab treatment. However, further research with a larger cohort is required to validate these findings. Furthermore, a limitation to our study was its retrospective nature. A disadvantage to this form was the use of the total number of cutaneous areas involved as the disease severity, thus not providing exact disease severity scores. A prospective study with a more standardized severity scoring system would be more informative.
ACKNOWLEDGEMENTS
The authors would like to thank Editage (www.editage.com) for English-language editing.
REFERENCES
- Schmidt E, Kasperkiewicz M, Joly P. Pemphigus. Lancet 2019; 394: 882–894. https://doi.org/10.1016/S0140-6736(19)31778-7
- Kasperkiewicz M, Ellebrecht CT, Takahashi H, Yamagami J, Zillikens D, Payne AS, et al. Pemphigus. Nat Rev Dis Primer 2017; 3: 17026. https://doi.org/10.1038/nrdp.2017.26
- Harman KE, Brown D, Exton LS, Groves RW, Hampton PJ, Mohd Mustapa MF, et al. British Association of Dermatologists’ guidelines for the management of pemphigus vulgaris 2017. Br J Dermatol 2017; 177: 1170–1201. https://doi.org/10.1111/bjd.15930
- Frampton JE. Rituximab: a review in pemphigus vulgaris. Am J Clin Dermatol 2020; 21: 149–156. https://doi.org/10.1007/s40257-019-00497-9
- Ahmed AR, Shetty S. A comprehensive analysis of treatment outcomes in patients with pemphigus vulgaris treated with rituximab. Autoimmun Rev 2015; 14: 323–331. https://doi.org/10.1016/j.autrev.2014.12.002
- Nosrati A, Hodak E, Mimouni T, Oren-Shabtai M, Levi A, Leshem YA, et al. Treatment of pemphigus with rituximab: real-life experience in a cohort of 117 patients in Israel. Dermatol Basel Switz 2021; 237: 450–456. https://doi.org/10.1159/000513515
- Sharma VK, Gupta V, Bhari N, Singh V. Rituximab as an adjuvant therapy for pemphigus: experience in 61 patients from a single center with long-term follow-up. Int J Dermatol 2020; 59: 76–81. https://doi.org/10.1111/ijd.14546
- Baum S, Raviv T, Gilboa S, Pavlotsky F, Barzilai A. Efficacy of repeated courses of rituximab as treatment for pemphigus vulgaris. Acta Derm Venereol 2020; 100: adv00286. https://doi.org/10.2340/00015555-3649
- Kushner CJ, Wang S, Tovanabutra N, Tsai DE, Werth VP, Payne AS. Factors associated with complete remission after rituximab therapy for pemphigus. JAMA Dermatol 2019; 155: 1404–1409. https://doi.org/10.1001/jamadermatol.2019.3236
- Saha M, Bhogal B, Black MM, Cooper D, Vaughan RW, Groves RW. Prognostic factors in pemphigus vulgaris and pemphigus foliaceus. Br J Dermatol 2014; 170: 116–122. https://doi.org/10.1111/bjd.12630
- Loi C, Magnano M, Ravaioli GM, Sacchelli L, Patrizi A, Bardazzi F. Rituximab therapy in pemphigus: a long-term follow-up. Dermatol Ther 2019; 32: e12763. https://doi.org/10.1111/dth.12763
- Kim TH, Choi Y, Lee SE, Lim JM, Kim SC. Adjuvant rituximab treatment for pemphigus: a retrospective study of 45 patients at a single center with long-term follow up. J Dermatol 2017; 44: 615–620. https://doi.org/10.1111/1346-8138.13757
- Lunardon L, Tsai KJ, Propert KJ, Fett N, Stanley JR, Werth VP, et al. Adjuvant rituximab therapy of pemphigus: a single-center experience with 31 patients. Arch Dermatol 2012; 148: 1031–1036. https://doi.org/10.1001/archdermatol.2012.1522
- Cho SI, Kim JW, Lim JS, Chung JH. Mucosal involvement is a risk factor for poor clinical outcomes and relapse in patients with pemphigus treated with rituximab. Dermatol Ther 2019; 32: e12814. https://doi.org/10.1111/dth.12814
- Ran NA, Payne AS. Rituximab therapy in pemphigus and other autoantibody-mediated diseases. F1000Research 2017; 6: 83. https://doi.org/10.12688/f1000research.9476.1
- Buch MH, Smolen JS, Betteridge N, Breedveld FC, Burmester G, Dörner T, et al. Updated consensus statement on the use of rituximab in patients with rheumatoid arthritis. Ann Rheum Dis 2011; 70: 909–920. https://doi.org/10.1136/ard.2010.144998
- Murrell DF, Dick S, Ahmed AR, Amagai M, Barnadas MA, Borradori L, et al. Consensus statement on definitions of disease, end points, and therapeutic response for pemphigus. J Am Acad Dermatol 2008; 58: 1043–1046. https://doi.org/10.1016/j.jaad.2008.01.012
- Parameswaran A, Attwood K, Sato R, Seiffert-Sinha K, Sinha AA. Identification of a new disease cluster of pemphigus vulgaris with autoimmune thyroid disease, rheumatoid arthritis and type I diabetes. Br J Dermatol 2015; 172: 729–738. https://doi.org/10.1111/bjd.13433
- Sánchez-García V, Pérez-Alcaraz L, Belinchón-Romero I, Ramos-Rincón JM. Comorbidities in patients with autoimmune bullous disorders: hospital-based registry study. Life 2022; 12: 595. https://doi.org/10.3390/life12040595
- Amber KT, Hertl M. An assessment of treatment history and its association with clinical outcomes and relapse in 155 pemphigus patients with response to a single cycle of rituximab. J Eur Acad Dermatol Venereol 2015; 29: 777–782. https://doi.org/10.1111/jdv.12678
- Nosrati A, Mimouni T, Hodak E, Gdalevich M, Oren-Shabtai M, Levi A, et al. Early rituximab treatment is associated with increased and sustained remission in pemphigus patients: a retrospective cohort of 99 patients. Dermatol Ther 2022; 35: e15397. https://doi.org/10.1111/dth.15397
- Balighi K, Daneshpazhooh M, Akbari Z, Tavakolpour S, Azimi P, Azizpour A. Comparing the short-term therapeutic effects and safety profiles of rituximab therapy in pemphigus vulgaris patients either early treated or later than six months. J Dermatol Treat 2019; 30: 346–349. https://doi.org/10.1080/09546634.2018.1509049
- Balighi K, Daneshpazhooh M, Mahmoudi H, Badakhsh M, Teimourpour A, Ehsani AH, et al. Comparing early and late treatments with rituximab in pemphigus vulgaris: which one is better? Arch Dermatol Res 2019; 311: 63–69. https://doi.org/10.1007/s00403-018-1881-1
- Anandan V, Jameela WA, Sowmiya R, Kumar MMS, Lavanya P. Rituximab: a magic bullet for pemphigus. J Clin Diagn Res JCDR 2017; 11: WC01–WC06. https://doi.org/10.7860/JCDR/2017/21868.9717
- Kyriakis KP, Tosca AD. Epidemiologic observations on the natural course of pemphigus vulgaris. Int J Dermatol 1998; 37: 215–219. https://doi.org/10.1046/j.1365-4362.1998.00317.x
- Joly P, Maho-Vaillant M, Prost-Squarcioni C, Hebert V, Houivet E, Calbo S, et al. First-line rituximab combined with short-term prednisone versus prednisone alone for the treatment of pemphigus (Ritux 3): a prospective, multicentre, parallel-group, open-label randomised trial. Lancet Lond Engl 2017; 389: 2031–2040. https://doi.org/10.1016/S0140-6736(17)30070-3
- Mignard C, Maho-Vaillant M, Golinski ML, Balayé P, Prost-Squarcioni C, Houivet E, et al. Factors associated with short-term relapse in patients with pemphigus who receive rituximab as first-line therapy: a post hoc analysis of a randomized clinical trial. JAMA Dermatol 2020; 156: 545–552. https://doi.org/10.1001/jamadermatol.2020.0290