Terbinafine, which targets squalene epoxidase (SQLE), has been used to treat dermatophyte infections for approximately 30 years. In 2017, a Swiss study reported that 1% (16/1,644) of Trichophyton rubrum and 0.2% (1/412) of T. interdigitale were resistant to terbinafine (1). In 2019, we presented the first Japanese case of tinea unguium caused by a terbinafine-resistant T. rubrum isolate (Phe397Leu substitution), which was deposited as IFM 65760 (2). Our clinic obtained 3 terbinafine-resistant T. rubrum strains (Leu393Phe substitution) from 95 dermatophyte clinical isolates including T. rubrum (n = 62) and T. interdigitale (n = 33) in June 2020 (3). One strain (T. rubrum N79) was derived from a group home for individuals with intellectual disabilities. In this study, we examined the residents of this facility using mycological and molecular techniques to detect terbinafine-resistant T. rubrum strains.
MATERIALS AND METHODS
The group home accommodates 54 individuals over 18 years of age and provides 24/7 care including bathing, toileting and meals. The facility is in Kumamoto, which has a subtropical climate (Köppen climate classification Cfa) with hot, humid summer at 32° north latitude. All patients diagnosed with dermatophytosis during a 6-month period (June to November 2020) were included in this study (n = 30 (20 males, 10 females); mean age 54.1 ± 17.7 years). Pathogens were identified in cultures on Sabouraud agar with chloramphenicol and cycloheximide (Mycosel agar; Kyokuto Pharmaceutical Industrial Co. Ltd, Tokyo, Japan) and/or by DNA-based detection for culture-negative onychomycosis in our clinic and Kahotechno Co., Ltd (Fukuoka, Japan). Molecular identifications, sequence analyses and antifungal susceptibility tests were performed at the Department of Veterinary Dermatology, Nihon University College of Bioresource Sciences (Kanagawa, Japan). The homology of the internal transcribed spacer region sequences in the rRNA gene of the strains was 100% (688/688 bp) identical to that of the T. rubrum reference strain IFM 63288 (GenBank, LC317851). The mutation hotspot of SQLE was determined based on the conserved sequence of T. rubrum SQLE (GenBank accession number XM_003233797) (3). The following primers were used: SQEL397S (5′- GTTGACTGGTGGCGGTATG; position 1002–1020) and SQEL397R (5′- GCTACGGAGTAAAAATGCCG; position 1315–1334) (Japanese patent application number 2021–2373). The antifungal susceptibility of the isolates to terbinafine, itraconazole, ravuconazole and luliconazole was evaluated by a broth microdilution assay according to the Clinical and Laboratory Standards Institute (CLSI) M38-A2 guidelines, with some modification (4).
RESULTS
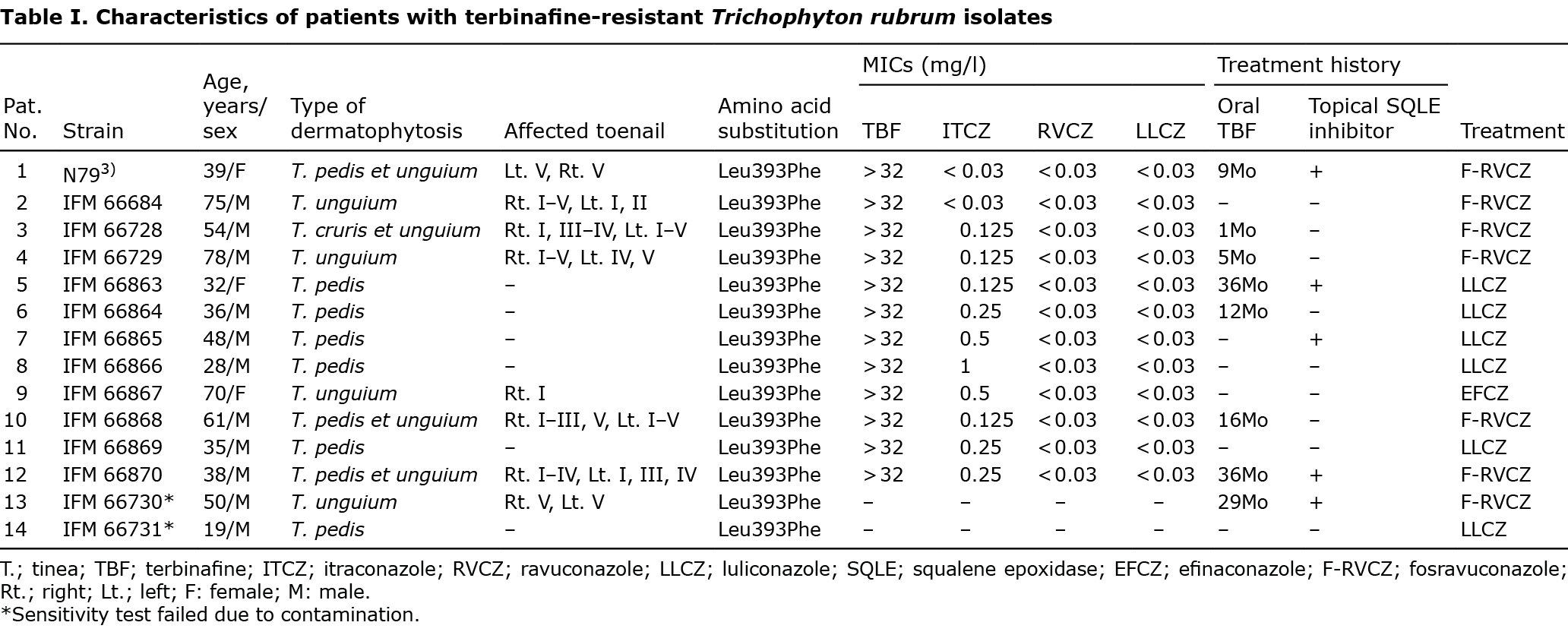
The 30 patients with dermatophytosis included patients with tinea pedis (n = 10), tinea unguium (n = 12), tinea pedis et unguium (n = 6), and tinea cruris et unguium (n = 2). Fungal cultures were positive in 17 cases and DNA-based detection of culture-negative onychomycosis was positive in 6 cases. The causative fungi were T. rubrum (n = 22, 95.6%) and T. interdigitale (n = 1, 4.3%). Among these cases, 47% (14/30) were caused by terbinafine-resistant T. rubrum. In addition, 60% (8/14) of the patients with terbinafine-resistant dermatophyte had tinea unguium and 5.4 ± 3.2 nails were affected. Regarding the affected nails, 62.5% (n = 10), 43.8% (n = 7), 50% (n = 8), 50% (n = 8), and 62.5% (n = 10) of the lesions involved the big, 2nd, 3rd, 4th and 5th toenail, respectively. Most patients (8/14) with terbinafine-resistant dermatophytes received oral terbinafine (125 mg, daily) for a mean duration of 24.4 ± 14.3 months. Five patients (5/14) were treated with topical SQLE inhibitors, either alone or in combination with oral treatment. Topical regimens included terbinafine, bifonazole, butenafine and liranaftate. Five patients (5/14) had no history of oral terbinafine or topical SQLE inhibitor use. The characteristics of patients with terbinafine-resistant isolates are shown in Table I. Nucleotide substitution within SQLE (1177TTA→TTC) was consequently detected in all 14 terbinafine-resistant strains, leading to Leu393Phe substitution in T. rubrum SQLE proteins. These isolates were deposited in Chiba University with IFM numbers. The minimum inhibitory concentrations (MICs) for the mutant strains were > 32 mg/l for terbinafine, < 0.03–1 mg/l for itraconazole, < 0.03 mg/l for luliconazole and < 0.03 mg/l for ravuconazole.
DISCUSSION
Terbinafine is the most commonly prescribed oral antifungal medicine that is approved for the treatment of tinea unguium. Meanwhile, terbinafine-resistant tinea corporis due to prolonged terbinafine therapy has been reported in a 62-year-old man with Darier disease (5). In our study, cases 5 and 12 received oral terbinafine for 3 years. In particular, case 12, who had hyperkeratotic-type tinea pedis and severe tinea unguium, might have been an index patient. Because Japanese people remove their shoes and walk barefoot in tatami rooms, the infection may spread even in a living room (6).
Itraconazole resistance in T. rubrum depends not on mutation of the target enzyme (lanoconazole 14-α-demethylase), but on the overexpression of the TruNDR2 gene, which encodes multidrug transporters of the ABC family (7). Itraconazole-resistant T. rubrum (TIMM20092) was isolated from a tinea pedis patient in Switzerland with a minimum inhibitory concentration (MIC) of 0.5 mg/l for itraconazole (7, 8). In our study, the MIC for itraconazole ranged from <0.03 to 1 mg/l. The MICs for ravuconazole and luliconazole were <0.03 mg/l, suggesting separated mechanisms of resistance.
Fosravuconazole, which was approved for tinea unguium treatment by the Japanese government in 2018 (9), is a novel triazole antifungal drug developed as a water-soluble prodrug for ravuconazole (10). Its excellent oral absorbability and systemic bioavailability have resulted in high serum drug concentrations and a long half-life (10). We treated 7 severe cases of tinea unguium with oral fosravuconazole and 1 mild case with efinaconazole 10% solution (11). Six patients with tinea pedis were treated with luliconazole 1% cream. As of July 2021, among the 7 fosravuconazole-treated patients with tinea unguium, 3 had been successfully cured, while 2 were showing a positive improvement. In addition, one patient treated with efinaconazole was also found to be improving. Among the 6 luliconazole-treated patients with tinea pedis, 5 had been successfully cured, while the other patient with a hyperkeratotic type had begun a treatment regimen with oral fosravuconazole.
A questionnaire survey of antifungal-resistant dermatophytes in representatives from European countries revealed that 85% of all countries (17/20) observed clinical and/or mycological confirmed resistance to terbinafine in 64% (61/96) and to itraconazole in 41% (39/96), while also observing resistance to fluconazole in 16% (15/96) (12). The 3 prevalent species were T. rubrum (33/95), Microsporum canis (23/95), and T. mentagrophytes (17/95) (12). Dermatologists should focus on the increasing numbers of terbinafine-resistant dermatophytes.
ACKNOWLEDGEMENTS
This work was partly supported by the Japan Agency for Medical Research and Development, AMED under Grant Number JP21fk0108094. The authors thank Dr. Yoshiharu Ohsato (Kahotechno Co., Ltd., Fukuoka, Japan) for the genetic diagnosis of onychomycosis.
REFERENCES
- Yamada T, Maeda M, Alshahni MM, Tanaka R, Yaguchi T, Bontems O, et al. Terbinafine resistance of Trichophyton clinical isolates caused by specific point mutations in the squalene epoxidase gene. Antimicrob Agents Chemother 2017; 61: e00115–e00117.
- Noguchi H, Matsumoto T, Hiruma M, Kimura U, Kano R, Yaguchi T, et al. Tinea unguium caused by terbinafine-resistant Trichophyton rubrum successfully treated with fosravuconazole. J Dermatol 2019; 46: e446–e447.
- Hiruma J, Noguchi H, Hase M, Tokuhisa Y, Shimizu T, Ogawa T, et al. Epidemiological study of terbinafine-resistant dermatophytes isolated from Japanese patients. J Dermatol 2021; 48: 564–567.
- Itoi S, Kano R, Hasegawa A, Hasegawa A, Kamata H. In vitro activities of antifungal agents against clinical isolates of dermatophytes from animals. J Vet Med Sci 2012; 74: 1067–1069.
- Digby SS, Hald M, Arendrup MC, Hjort SV, Kofoed K. Darier disease complicated by terbinafine-resistant Trichophyton rubrum: a case report. Acta Derm Venereol 2017; 97: 139–140.
- Maruyama R, Katoh T, Nishioka K. Demonstration of dermatophyte dissemination from the infected soles using the foot-press method. Mycoses 1998; 41: 145–151.
- Yamada T, Yaguchi T, Tamura T, Pich C, Salamin K, Feuermann M, et al. Itraconazole resistance of Trichophyton rubrum mediated by the ABC transporter TruMDR2. Mycoses 2021; 64: 936–946.
- Monod M, Feuermann M, Salamin K, Fratti M, Makino M, Alshahni MM, et al. Trichophyton rubrum azole resistance mediated by a new ABC transporter, TruMDR3. Antimicrob Agents Chemother 2019; 63: e00863–e00819.
- Yamaguchi H. Potential of ravuconazole and its prodrugs as the new oral therapeutics for onychomycosis. Med Mycol J 2016; 57: E93–E110.
- Watanabe S, Tsubouchi I, Okubo A. Efficacy and safety of fosravuconazole L-lysine ethanolate, a novel oral triazole antifungal agent, for the treatment of onychomycosis: a multicenter, double-blind, randomized phase III study. J Dermatol 2018; 45: 1151–1159.
- Foley K, Gupta AK, Versteeg S, Mays R, Villanueva E, John D. Topical and device-based treatments for fungal infections of the toenails. Cochrane Database Syst Rev 2020; 1: CD012093.
- Saunte DML, Pereiro-Ferreirós M, Rodríguez-Cerdeira C, Sergeev AY, Arabatzis M, Prohić A, et al. Emerging antifungal treatment failure of dermatophytosis in Europe: take care or it may become endemic. J Eur Acad Dermatol Venereol 2021; 35: 1582–1586.