Body dysmorphic disorder (BDD) is a mental health condition characterized by disproportional occupation with imagined or minimal defects in appearance (1). This obsession is associated with shame, anxiety, depression, and poor quality of life (2, 3). Although any body part may be of concern, preoccupation is concentrated mostly on the head, face or cutaneous appearance (4). BDD-affected individuals usually show impaired insight in the psychiatric origin of their concerns, and therefore typically visit plastic surgeons and dermatologists (4). Currently, the condition is often under-recognized and therefore underdiagnosed (1). There are no data on the prevalence of BDD in dermatology patients in Belgium, and data from other European countries are scarce. The aim of this study was to screen for BDD in general dermatology and dermato-cosmetic clinics in a university hospital. Furthermore, the study assessed associations between BDD and anxiety and depression.
MATERIALS AND METHODS
A cross-sectional study was conducted between September 2016 and October 2017 at the outpatient clinic of the dermatology department of the University Hospital Brussels (UZ Brussel). Participants were recruited from the cosmetic unit (cosmetic group, CosG) and the general outpatient clinic (control group, CtrG). Participants had to be female and >18 years old. Patients for the CosG had to consult for injections with botulinum toxin or dermal hyaluronic fillers. The CtrG had to present for a general check-up of naevi or for excision thereof on medical indication. Patients with contraindications to injection of Botox or fillers were excluded. Prior to treatment, participants completed 3 questionnaires: a questionnaire on demographics, the Body Dysmorphic Disorder Questionnaire (BDDQ- DV) (5) and the Hospital and Anxiety Depression scale (HADS) (6). The BDDQ-DV is a tool to screen for BDD and is considered positive if patients report the presence of a preoccupation with their appearance in combination with a moderate (≥ 3) score in distress or impairment in functioning related to this preoccupation. Dutch and French versions of this questionnaire were used and validated by multiple back-forth translations and reconciliation (linguistic validation). The HADS is a 14-item self-assessment Likert scale questionnaire that identifies symptoms of anxiety and depression in the previous week. Scores of 11 or more for both anxiety and depression are considered “positive”, while scores of 8–10 are considered “borderline”.
This study was approved by the ethics committee of UZ Brussel and conducted according to the principles of the Declaration of Helsinki and Good Clinical Practice.
The results are shown as mean or median with standard deviation (SD) or quartiles. Significance was tested using the Mann–Whitney U test for continuous variables and the χ2 (trend) test for categorical variables. IBM SPSS Statistics version 24.0.0 (IBM Corp., Armonk, NY, USA) was used for analyses.
RESULTS
From 181 participants, 8 questionnaires (CosG: 6, CtrG: 2) were excluded due to incomplete data. The final analysis included 173 participants; 74 in the CosG and 99 in the CtrG. Baseline characteristics of the groups are shown in Table I.

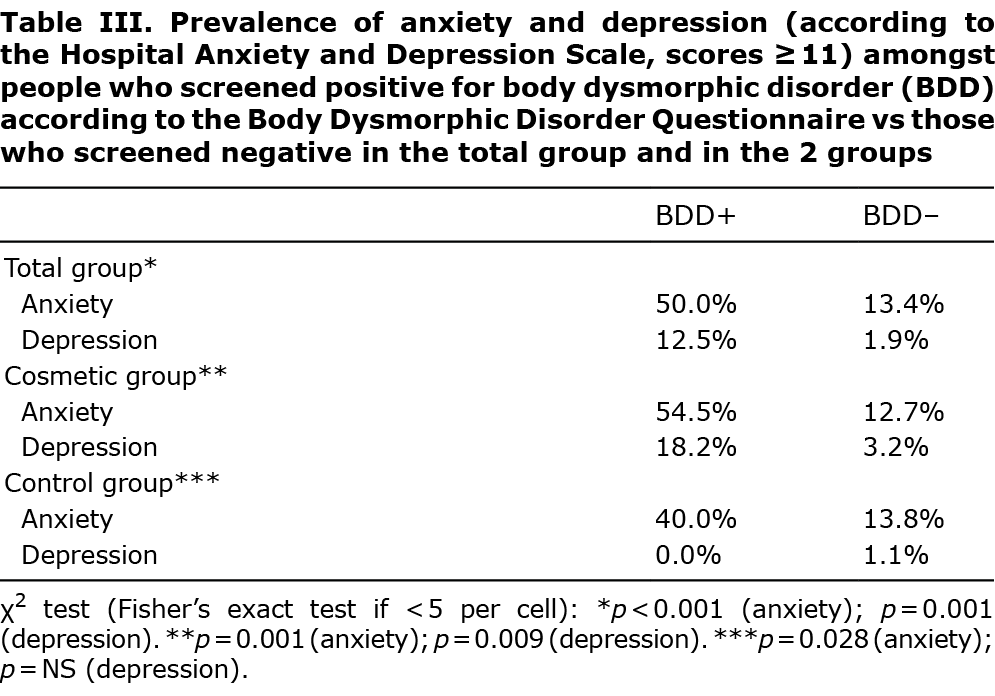
For the total group (n = 173), the BDDQ-DV was positive in 16.8%. Patients who scored BDD-positive often indicated more than 1 focus, e.g. skin plus body weight or specific body parts. When focusing on skin-related concerns only (wrinkles, pores, scars, pigmentation), 14.9% of the CosG and 5.1% of the CtrG (p < 0.05, Table II) scored BDD-positive. After stratification by age, this tendency remained; however, it was not significant (probably due to the limited sample size). Univariate analyses showed that only lower educational levels were significantly associated with positive BDDQ-DV. Anxiety and depression, i.e. HADS scores of 11 and higher on either HADS scale, were significantly more frequent amongst participants who scored positive on the BDDQ-DV in the total group, as well as in both study groups (Table III).

DISCUSSION
Because epidemiological knowledge concerning BDD in Belgium has focused mainly on rhinoplastic surgery, reporting a 33% prevalence of at least moderate BDD (7), the current study screened for BDD in patients consulting for dermatological and cosmetic care. Focusing on skin-related concerns only, BDDQ-DV was identified as positive in 14.9% of the patients in the CosG, which was significantly different compared with 5.1% in the CtrG.
The current data are comparable with other data describing BDD in dermatology patients. One study reported a prevalence of, respectively, 14.0% and 6.7% for cosmetic and general dermatology settings (8), while a systematic review found a BDD prevalence of 11.3% for general dermatology outpatients vs 9.2% for cosmetic dermatology outpatients (2). Variations in inclusion criteria and the use of different screening tools could explain these differences (9).
The current study found an association between lower level of education and positive screening with the BDDQ-DV, which is in line with previous data (10). Amongst those who scored positive with the BDDQ-DV, anxiety scores of 11 and higher were also more frequent. Indeed, anxiety disorders frequently coexist with BDD (3).
A limitation of the current study is that it only identified those with positive scores on the BDDQ-DV. As this instrument has specificity of 94.7%, these patients should be referred for an additional interview and/or objective assessment of their preoccupation (5). The screening used in the current study may therefore over-diagnose BDD. On the other hand, some experts suggest that patients may be more honest when using anonymous questionnaires (11). Other limitations are response bias, which is inherent to the current study sampling procedure, and selection bias, as it is now known exactly how many patients declined to participate. Moreover, only female patients were included, as they comprised the vast majority of patients seeking cosmetic care.
In conclusion, dermatologists and others dealing with patients for cosmetic care need to be aware of BDD as a disease and its high prevalence. Currently, many of these patients are being treated suboptimally without psychiatric care. This study was performed in a large multicultural environment, and therefore we consider the findings to be generalizable to other Western European cities. Finally, these results also emphasize the need for multidisciplinary collaboration or psychodermatology units for dermatology patients seeking minor or non-surgical cosmetic interventions.
The authors have no conflicts of interest to declare.
REFERENCES
- Phillips KA. The broken mirror: understanding and treating body dysmorphic disorder. Oxford: Oxford University Press; 2005: p. 5.
- Veale D, Gledhill LJ, Christodoulou P, Hodsoll J. Body dysmorphic disorder in different settings: a systematic review and estimated weighted prevalence. Body Image 2016; 18: 168–186.
- Veale D, Bewley A. Body dysmorphic disorder. BMJ 2015; 350: h2278.
- Phillips KA, Dufresne RG. Body dysmorphic disorder: a guide for dermatologists and cosmetic surgeons. Am J Clin Dermatol 2000; 1: 235–243.
- Dufresne RG, Phillips KA, Vittorio CC, Wilkel CS. A screening questionnaire for body dysmorphic disorder in a cosmetic dermatologic surgery practice. Dermatol Surg 2001; 27: 457–462.
- Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand 1983; 67: 361–370.
- Picavet VA, Prokopakis EP, Gabriëls L, Jorissen M, Hellings PW. High prevalence of body dysmorphic disorder symptoms in patients seeking rhinoplasty. Plast Reconstr Surg 2011; 128: 509–517.
- Conrado LA, Hounie AG, Diniz JB, Fossaluza V, Torres AR, Miguel EC, et al. Body dysmorphic disorder among dermatologic patients: prevalence and clinical features. J Am Acad Dermatol 2010; 63: 235–243.
- Vulink NC, Rosenberg A, Plooij JM, Koole R, Bergé SJ, Denys D. Body dysmorphic disorder screening in maxillofacial outpatients presenting for orthognathic surgery. Int J Oral Maxillofac Surg 2008; 37: 985–991.
- Mataix-Cols D, de la Cruz LF, Isomura K, Anson M, Turner C, Monzani B, Krebs G. A pilot randomised controlled trial of cognitive-behavioural therapy for adolescents with body dysmorphic disorder. J Am Acad Child Adolesc Psychiatry 2015; 54: 895–904.
- Phillips KA. The broken mirror: understanding and treating body dysmorphic disorder. Oxford: Oxford University Press; 2005: p. 379–381.