Hidradenitis suppurativa (HS) is a chronic, recurrent, inflammatory skin disease of the apocrine gland-bearing areas, characterized by painful nodules, abscesses, fistulas and scarring. The pathophysiology has not been clearly defined, but HS is considered a multifactorial disease with the involvement of several immunological factors.
An upregulation of various cytokines, such as tumour necrosis factor (TNF)-α, interleukin (IL)-1, IL-17, IL-23 contribute to the genesis of the inflammatory component characteristic of the disease (1). Adalimumab, a TNF-α inhibitor, is the only US Food and Drug Administration (FDA) approved biologic agent for moderate-to-severe HS (2), but new therapeutic options are being studied, targeting different specific cytokines involved in HS pathogenesis. The aim of this study is to provide an overview of the efficacy and safety of risankizumab, an anti-IL-23 agent, in the treatment of HS.
MATERIALS AND METHODS
A retrospective study was conducted at the Dermatology clinic of the Turin University Hospital during November 2020 to December 2021.
Patients with moderate to severe HS (Hurley stage II or III) who were prescribed risankizumab, at the approved dosage for psoriasis, were included. Among them, 2 distinct groups were identified: group 1 included patients who received risankizumab therapy after approval for off-label use by the Committee on Rare Diseases (due to no response to adalimumab); group 2 included patients who were given risankizumab after the onset of paradoxical psoriasis during adalimumab therapy, which did not resolve even after discontinuation of the anti-TNF-α drug. Efficacy was evaluated by identifying HS clinical response rate (Hi-SCR) and Hidradenitis Suppurativa Severity Score System (IHS4) by clinical evaluation and objective examination every 3 months; ultrasound survey could not be used due to difficult radiological collaboration during the COVID-19 pandemic. Drug response in terms of quality of life was assessed by self-completion of the Dermatology Quality of Life Index (DLQI) questionnaire.
RESULTS
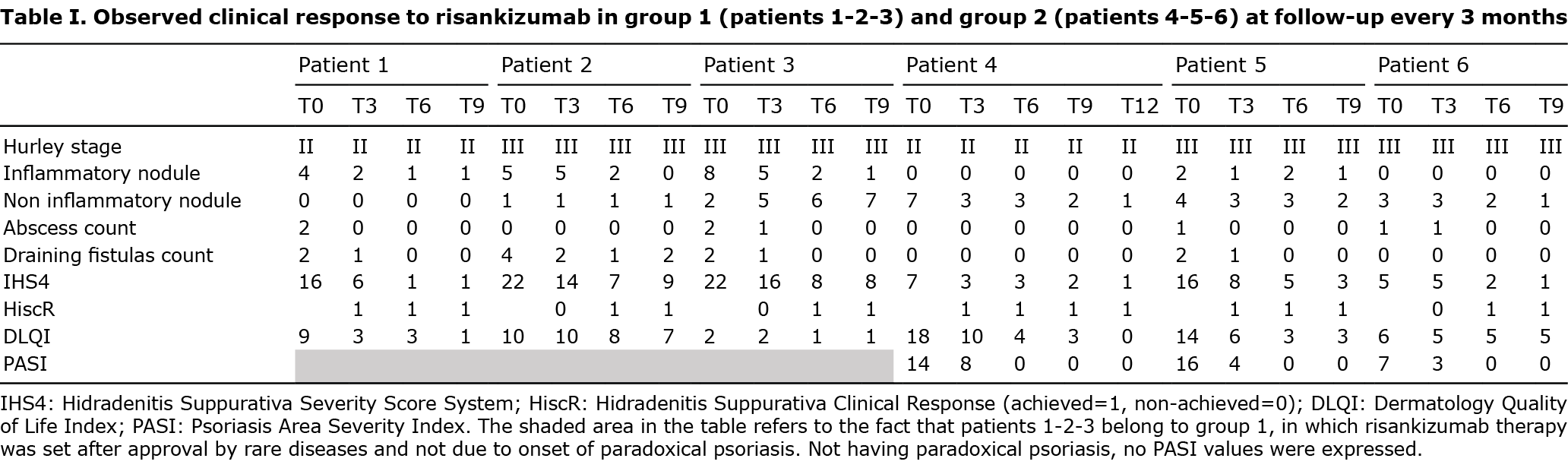
A total of 6 patients with HS, 5 males and 1 female, were included. The overall mean age of the patients was 44.17 years (range 25–79 years). Mean body mass index (BMI) was 28.3 kg/m2 (range 22.3–40.1 kg/m2). Four patients were in Hurley stage III and 2 were in Hurley stage II. Two of them were active smokers, while 2 reported having quit smoking for at least 1 year. All patients had been previously treated with systemic antibiotics with relapse upon discontinuation, one of them with oral retinoids, all patients had previously received treatment with adalimumab, none was bio-naive. Two of the patients had undergone surgery, one a partial axillary excision and one a radical axillary surgery. All previously prescribed medications for HS had been discontinued at least 2 months before starting risankizumab. Three patients were included in group 1, and 3 patients in group 2. No systemic therapy was prescribed concurrently with risankizumab biologic therapy, only topical antibiotic therapy when needed. All patients showed clinical improvement in HS, with a progressive reduction in the number of inflammatory lesions and a reduction in IHS4 assessed by clinical examination at subsequent clinical re-evaluations. Of the 6 patients, 3 achieved Hi-SCR at month 3; all patients achieved Hi-SCR at month 6. Similarly, a benefit in quality of life was observed. In group 1 all achieved Hi-SCR at month 6. Group 2 patients presented a lower IHS4 score at baseline due to good control during previous therapy with adalimumab and maintained HS control with further reduction in IHS4 during follow-up; in this group progressive improvement in their psoriasis was documented, with achievement of PASI 0 at month 6.
PASI, lesions count, IHS4, HISCR and DLQI regarding patients in group 1 and group 2 at the enrolment and follow-up are shown in Table I. IHS4 and DLQI values during the follow-up is shown in Fig. 1. None of the patients experienced adverse events. Exacerbation of patients’ comorbidities was not reported. Changes in patients’ risk factors (smoking, BMI, wearing tight clothing, etc.) were not observed.

DISCUSSION
The pathogenesis of HS is not yet well understood, but involves multiple factors, such as genetics, environment, host-microbe interactions, and immune dysregulation. Proinflammatory cytokines IL-1β, IL-17 and IL-23 have been demonstrated to be increased in HS-affected subjects and IL-17 and IL-23 overexpression has been detected in lesional and perilesional HS skin, promoting differentiation of Th17 cells and thus being involved in the pathogenesis of HS (1, 3, 4).
Based on this evidence, new therapeutic options for HS targeting different specific cytokines are being investigated. Regarding anti IL-23 biological drugs, data on their use in the treatment of HS mainly include ustekinumab, guselkumab, and risankizumab (5). In literature response rates to ustekinumab, anti-IL-12/23 agents, have been variable in several case reports and small series (6, 7); in most cases psoriasis dosages have been administered, but it is considered that higher doses might be necessary for HS (8). Some case reports (8, 9) have reported good results in treating recalcitrant HS with guselkumab, anti-IL-23 agent, at the approved dosage for psoriasis, while one case series reported poor results with higher doses of guselkumab (10). Among the anti-IL-23 drugs the current study focused on the safety and efficacy of risankizumab, a humanized immunoglobulin G1 monoclonal antibody that binds the p19 subunit of IL-23 and selectively blocks IL-23, in patients with HS. So far, only 3 cases of HS successfully treated with risankizumab have been described in the literature (12, 13), and there is only one mention of the use of risankizumab as an effective treatment option in patients with concomitant psoriasis and HS (14). All of these patients had been treated previously with different drugs, including oral antibiotics, steroids and adalimumab, with failure. The case reported by Caposiena et al. (13) had also been treated previously with secukinumab, while ciclosporin and methotrexate had been administered in the single case described by Licata et al. (14) because of his concomitant psoriasis.
To the best of our knowledge this is the largest case series of patients affected with HS and treated with risankizumab. All of the patients had received adalimumab as biological treatment for HS, similar to what was previously described in the literature: no patient was bio-naive.
In addition, this case series confirms the safety data for risankizumab, as proven from psoriasis registration studies. The main limitations of the current study are the short follow-up period and the small number of patients enrolled; these are preliminary data that need further studies to be confirmed.
In conclusion, these preliminary data confirm, in the largest case series to date, the safety and efficacy of risankizumab in the treatment of HS. Risankizumab may be an additional treatment option for patients in whom other therapies had been ineffective, including other biologics.
Risankizumab could also represent an alternative in patients with HS with concomitant psoriasis, particularly when this occurs as an adverse event during therapy with adalimumab and persists despite discontinuation of the drug.
The authors have no conflicts of interest to declare.
REFERENCES
- Jiang SW, Whitley MJ, Mariottoni P, Jaleel T, MacLeod AS. Hidradenitis suppurativa: host-microbe and immune pathogenesis underlie important future directions. JID Innov 2021; 1: 100001.
- Kimball AB, Okun MM, Williams DA, Gottlieb AB, Papp KA, Zouboulis CC, et al. Two phase 3 trials of adalimumab for hidradenitis suppurativa. N Engl J Med 2016; 375: 422–434.
- Kelly G, Hughes R, McGarry T, van den Born M, Adamzik K, Fitzgerald R, et al. Dysregulated cytokine expression in lesional and non lesional skin in hidradenitis suppurativa. Br J Dermatol 2015; 173: 1431–1439.
- Schlapbach C, Hänni T, Yawalkar N, Hunger RE. Expression of the IL-23/Th17 pathway in lesions of hidradenitis suppurativa. J Am Acad Dermatol 2011; 65: 790–798.
- Amat-Samaranch V, Agut-Busquet E, Vilarrasa E, Puig L. New perspectives on the treatment of hidradenitis suppurativa. Ther Adv Chronic Dis 2021; 12: 20406223211055920.
- Montero-Vilchez T, Pozo-Román T, Sánchez-Velicia L, Vega-Gutiérrez J, Arias-Santiago S, Molina-Leyva A. Ustekinumab in the treatment of patients with hidradenitis suppurativa: multicenter case series and systematic review. J Dermatolog Treat 2022; 33: 348–353.
- Sharon VR, Garcia MS, Bagheri S, Goodarzi H, Yang C, Ono Y, Maverakis E. Management of recalcitrant hidradenitis suppurativa with ustekinumab. Acta Derm Venereol 2012; 92: 320–321.
- Blok JL, Li K, Brodmerkel C, Horvátovich P, Jonkman MF, Horváth B. Ustekinumab in hidradenitis suppurativa: clinical results and a search for potential biomarkers in serum. Br J Dermatol 2016; 174: 839–846.
- Kovacs M, Podda M. Guselkumab in the treatment of severe hidradenitis suppurativa. J Eur Acad Dermatol Venereol 2019; 33: e140–e141.
- Burzi L, Repetto F, Ramondetta A, Rozzo G, Licciardello M, Ribero S, et al. Guselkumab in the treatment of severe hidradenitis suppurativa, a promising role? Dermatol Ther 2021; 34: 14930.
- Montero-Vilchez T, Martinez-Lopez A, Salvador-Rodriguez L, Arias-Santiago S, Molina-Leyva A. The use of guselkumab 100 mg every 4 weeks on patients with hidradenitis suppurativa and a literature review. Dermatol Ther 2020; 33: 13456.
- Marques E, Arenberger P, Smetanová A, Gkalpakiotis S, Zimová D, Arenbergerová M. Successful treatment of recalcitrant hidradenitis suppurativa with risankizumab after failure of anti-tumour necrosis factor alpha. Br J Dermatol 2021; 184: 966–967.
- Caposiena Caro RD, Pensa C, Lambiase S, Candi E, Bianchi L. Risankizumab effectiveness in a recalcitrant case of hidradenitis suppurativa after anti-TNF and anti-interleukin-17 failures. Dermatol Ther 2021; 34: 15116.
- Licata G, Gambardella A, Buononato D, De Rosa A, Calabrese G, Pellerone S, et al. A case of moderate hidradenitis suppurativa and psoriasis successfully treated with risankizumab. Int J Dermatol 2021; 61: 126–129.