A wide range of symptoms associated with COVID-19 infection and vaccinations have been reported (1). Due to the increasing number of patients with cutaneous symptoms associated with COVID-19, dermatologists may misdiagnose such symptoms as COVID-19-related. We report here a case of Cronkhite-Canada syndrome (CCS), which was overlooked for several months because of its similarity to COVID-19-related symptoms.
CASE REPORT
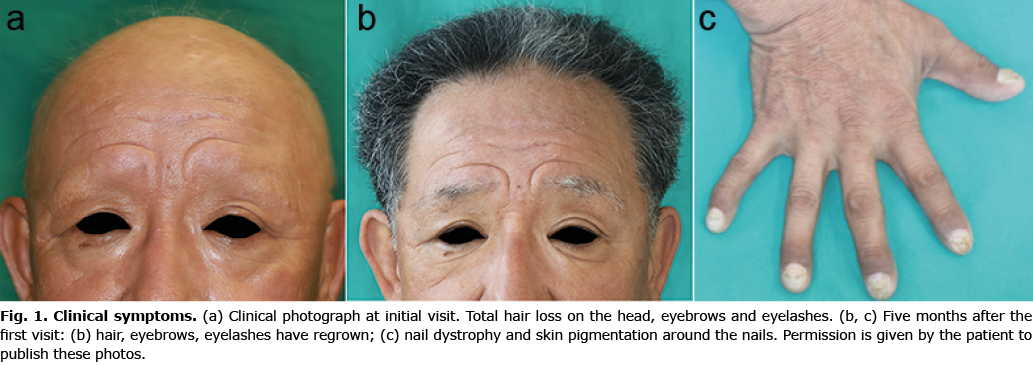
A 65-year-old male with a medical history of chronic gastritis was referred to our department due to generalized alopecia. Hair loss had started on his head, eyebrows, eyelashes, and pubic hair 2 months before the visit and evolved into complete hair loss over a period of 2 months (Fig. 1a). He reported simultaneous development of nail dystrophy and dysgeusia. Laboratory analysis showed a decrease in albumin (3.2, normal range; 4.1–5.1 g/dl), total protein (5.9, normal range; 6.6–8.1 g/dl) and elevation of C-reactive protein (CRP) (3.386, normal range; 0–0.14 mg/dl). Autoantibody or abnormalities of the thyroid gland was not evident. He had been vaccinated with the second dose of COVID-19 mRNA vaccine (BNT162b2 (Pfizer–BioNTech)) approximately 4 weeks before the onset of hair loss. Reverse transcription-polymerase chain reaction (RT-PCR) for COVID-19 was negative at his first visit to our hospital. Because alopecia and dysgeusia were common symptoms in COVID-19 infection (although rarely seen with vaccination), he was diagnosed with a COVID-19 vaccination-related condition. Treatment with 14 days of 20 mg/day of oral prednisolone was started, and was tapered off gradually over a period of 5 months, resulting in almost complete hair regrowth (Fig. 1b). After his hair regrew and oral prednisolone was tapered, abdominal pain developed and colonoscopy revealed multiple polyposes of his entire colon. Based on these symptoms, CCS was considered. Re-evaluation of his skin showed pigmentation around the nails (Fig. 1c). There was no family history of colonic polyposis. The patient was diagnosed with CCS 5 months after he first visited our department. Although the 20 mg of oral prednisolone improves his hair symptoms completely and it did not relapse after tapering, his dysgeusia did not improve with this dose of prednisolone. After we diagnose him with Cronkhite-Canada syndrome, he was treated with 30 mg of oral prednisolone. After several days of up-dosing, his dysgeusia ameliorated completely. Oral prednisolone was tapered to 5 mg over a half year, and his dysgeusia did not relapse.
DISCUSSION
CCS is a rare disease characterized by non-hereditary, non-tumorigenic gastrointestinal polyposis. Patients usually have chronic gastrointestinal symptoms, dysgeusia, hair loss, nail dystrophy, and skin pigmentation (2). To date, several hundred cases of CCS have been reported worldwide. Among these, Asian middle-aged male patients are relatively frequent (2). Although no consensus treatment for CCS is established, it is reported that approximately 85% of patients respond to treatment with over 30 mg/day prednisolone (2). The onset of CCS is often in patients in their 60s, and its pathogenesis has not yet been revealed. In the current case, the patient showed all the typical symptoms and characteristics of CCS, but this condition was not considered in the differential diagnosis at the initial visit due to hair loss and dysgeusia being common in patients with COVID-19 (1). Although nail dystrophy is rarely reported as a symptom of COVID-19, it sometimes occurs with generalized alopecia (4); hence these symptoms were overlooked at the initial visit. Several reports indicate a relationship between COVID-19 vaccination and hair loss, but the causation is not clear (4). COVID-19 vaccination-related dysgeusia or nail dystrophy has not been reported. The current case exemplifies that clinicians may be biased in making a diagnosis, especially in the midst of the COVID-19 pandemic.
The authors have no conflicts of interest to declare.
REFERENCES
- Alkodaymi MS, Omrani OA, Fawzy NA, Shaar BA, Almamlouk R, Riaz M, et al. Prevalence of post-acute COVID-19 syndrome symptoms at different follow-up periods: a systematic review and meta-analysis. Clin Microbiol Infect 2022; 28: 657–666.
- Wu ZY, Sang LX, Chang B. Cronkhite-Canada syndrome: from clinical features to treatment. Gastroenterol Rep (Oxf) 2020; 8: 333–342.
- Chelidze K, Lipner SR. Nail changes in alopecia areata: an update and review. Int J Dermatol 2018; 57: 776–783.
- Gallo G, Mastorino L, Tonella L, Ribero S, Quaglino P. Alopecia areata after COVID-19 vaccination. Clin Exp Vaccine Res 2022; 11: 129–132.