ORIGINAL REPORT
Comorbidities and Medication Use in Finnish Patients with Psoriasis: A Population-Based Registry Study
Aino VESIKANSA1, Juha MEHTÄLÄ1, Marko PESU2,3, Jaakko AALTONEN2, Riikka KONTTINEN2, Kaisa TASANEN4 and Laura HUILAJA4
1MedEngine Oy, 2AbbVie Oy, Helsinki, 3Current address: Gilead Sciences Finland Oy, Vantaa and 4Department of Dermatology and Medical Research Center, Oulu University Hospital; Research Group of Clinical Medicine, University of Oulu, Oulu, Finland
Therapeutic options for psoriasis vulgaris have changed during recent decades with the introduction of biologics. Few nationwide studies are available on psoriasis treatment patterns, and those from Finland predate the use of biologics. The aim of this retrospective, population-based registry study was to identify patients with psoriasis vulgaris and their treatment patterns in the secondary care setting in Finland. The study cohort included 41,456 adults with a diagnosis of psoriasis vulgaris in the public secondary healthcare setting from 2012 through 2018. Data on comorbidities, pharmacotherapy, and phototherapy were collected from nationwide healthcare and drug registries. Patients in the cohort had a wide range of comorbidities, with 14.9% having psoriatic arthritis. Treatment was based largely on topical and conventional systemic medications. Conventional medications were used by 28.9% of patients, and methotrexate was the most common option (20.9%). Biologics were used by 7.3% of patients, mostly as second- and third-line treatment. The use of conventional systemic medications, topical treatments, and phototherapy decreased after the initiation of biologics. This study of psoriasis vulgaris in Finland provides a framework for the development of future care practices.
Key words: biologic; biological treatment; comorbidity; plaque psoriasis; psoriasis vulgaris; treatment.
SIGNIFICANCE
This population-based study identified adult patients with psoriasis vulgaris (psoriasis) and their treatment patterns in the secondary care setting in Finland. The results indicate that patients with psoriasis had a wide range of comorbidities, with 15% having psoriatic arthritis. Treatment was based largely on topical treatments. Conventional systemic (oral) medications were used by approximately 30% and biological treatments by 7% of patients. The results provide important information on psoriasis patients and their current treatment patterns and form a framework for the development of future care practices for psoriasis in Finland.
Citation: Acta Derm Venereol 2023; 103: adv00886. DOI https://doi.org/10.2340/actadv.v103.3491.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Accepted: Feb 1, 2023; Published: Mar 9, 2023
Corr: Aino Vesikansa, MedEngine Oy, Eteläranta 14, FIN-00130 Helsinki, Finland. E-mail: aino.vesikansa@medengine.fi
Competing interests and funding: LH has received educational grants from AbbVie, Janssen-Cilag, LEO, Novartis, and Takeda; honoraria from AbbVie, Boeringer Ingelheim, Lilly, Novartis, Orion, Pfizer, and Sanofi Genzyme for consulting and/or speaking; and is an investigator for AbbVie. AV and JM are employees of MedEngine Oy. RK and JA are employees of AbbVie and may or may not own AbbVie shares. MP was an employee of AbbVie during the study and is currently an employee of Gilead Sciences Oy. KT has received educational grants from Sanofi Genzyme and honoraria from AbbVie, Bristol Myers Squibb, Janssen-Cilag, Leo, Novartis, Sanofi Genzyme, and UCB for consulting and/or speaking.
INTRODUCTION
Psoriasis is a chronic, immune-mediated, inflammatory skin disease that affects 1–5% of the population in Europe (1, 2). Psoriasis can manifest at any age, but more often affects adults (3). Psoriasis vulgaris is the most common form of the disease, accounting for more than 80% of cases of psoriasis (3). During the last decades, rapid advancements have been made in understanding the pathogenesis and genetics of psoriasis vulgaris (henceforth termed psoriasis), including comorbidities associated with the disease (3).
Due to its chronicity and high prevalence, psoriasis represents a substantial burden for society (4, 5). Furthermore, with its disease-related discomfort and disability, psoriasis also represents a significant burden on the patient. Psoriasis is associated with significant comorbidities, including rheumatoid arthritis (RA) and psoriatic arthritis (PsA), metabolic syndrome, cardiovascular diseases, and inflammatory bowel disease (IBD) (6–8). Psoriasis has also negative psychosocial effects, and severe psoriasis is associated with reduced quality of life (QoL) (9). Moreover, patients with psoriasis are shown to have more mental disorders than individuals in the general population (10, 11).
Currently, there is no cure for psoriasis. Disease management aims to minimize the physical and psychological harm to patients, improve their QoL and functional ability, as well as prevent associated multimorbidity (3, 12–14). Overall treatment strategies for psoriasis should consider disease severity and disease outcomes, but also the presence of PsA and other comorbidities (12–14).
Topical therapies including corticosteroids, vitamin D analogues, calcineurin inhibitors, keratolytics, and various emollients are the main treatment options for mild and localized psoriasis. Targeted and/or full-body phototherapy is an effective alternative for moderate psoriasis. However, phototherapy use is limited by its accessibility and an increased risk of skin cancer associated with repeated and long-term treatment (3, 15). In addition, the burden of phototherapy treatment for the patients and society, due to travelling, absence from work, and other daily activities, can be considerable.
The oral small-molecule immunosuppressants methotrexate, acitretin, and cyclosporine have been considered the primary systemic medications for moderate to severe psoriasis for decades (16). However, they are associated with multiple contraindications, and patient compliance with oral immunosuppressants is often suboptimal (17). Recent therapeutic advancements for moderate to severe psoriasis include biologics targeted at, for example, tumour necrosis factor-α (TNF-α), the p40 subunit of interleukin (IL)-12 and IL-23 (p40IL-12/23), IL-17, and the p19 subunit of IL-23 (p19IL-23), as well as a small molecule inhibitor of phosphodiesterase 4 (PDE4) (15,18).
When evaluating therapeutic options to provide cost-effective care it is crucial to have a thorough understanding of patient profiles. However, previous reports of psoriasis from Finland mostly predate the introduction of biologics, and, globally, only a few nationwide studies are available (19–21). The aim of this retrospective, population-based registry study was to identify patients with psoriasis and their treatment patterns in the secondary care setting in Finland. The prevalence of comorbidities and the use of treatments were assessed using national healthcare and drug reimbursement registries in a nationwide cohort of patients. In addition, a subgroup of patients who started their treatment with a biologic was analysed.
MATERIALS AND METHODS
Study cohort, data collection and subgroups
For this retrospective, register-based study, all adult patients (≥18 years of age) with a diagnosis of psoriasis (International Classification of Diseases, 10th Revision (ICD-10), diagnosis code L40.0) in the Finnish Care Register for Health Care (CRHC, secondary public healthcare) between 1 January 2012, and 31 December 2018, were identified.
For the identified study cohort (“total cohort”), individual-level data on the use of public healthcare services, diagnoses (ICD-10), phototherapy, and medications were further collected retrospectively from the CRHC (secondary public healthcare) and Register of Primary Health Care Visits (primary public healthcare), both of which are maintained by the Finnish Institute for Health and Welfare, and the Register of Reimbursed Drugs, which tracks the purchase of reimbursed drugs and is maintained by the Social Insurance Institution of Finland. Data were collected from January 2012 through December 2018 (observation period). Individual-level data from different registries were linked using unique personal social security numbers and analysed in a pseudonymized format. According to the law on the secondary use of health and social data (Act on the Secondary Use of Health and Social Data), retrospective non-interventional registry studies do not require ethics committee review.
The primary study group included all identified patients (total cohort, n = 41,456). For subgroup analyses, the total cohort was divided into 2 subgroups. Subgroup 1 (n = 14,337) comprised patients who had their first psoriasis diagnosis (ICD-10 code L40.0) in the secondary healthcare setting between 1 January 2013, and 31 December 2017, with no prior psoriasis diagnoses in primary or secondary care during the observation period (January 2012 onwards; a minimum of 1 year without psoriasis diagnoses). The date of the first psoriasis diagnosis during the observation period was defined as the index date for patients in subgroup 1. Subgroup 2 (n = 1,297) comprised biologic starters, those patients who initiated biologics during the period from January 2013 to December 2017 and had no prior use of biologics during the observation period (January 2012 onward). The index date for this subgroup was the date of biologic initiation. Treatment patterns were analysed in this subgroup separately from the period before and the period after the index date.
Outcome measures
The aim of this study was to identify the characteristics of patients with psoriasis and their treatment patterns in a Finnish population-based cohort. The prevalence of comorbid conditions was assessed based on ICD-10 codes in the CRHC and the Register of Primary Care Visits. In addition, healthcare specialty codes in the CRHC were used as a proxy for selected comorbidity groups (Table SI). Both the primary and secondary diagnoses recorded for a visit were included in the analyses.
The use of pharmacological treatments was assessed based on purchases of reimbursable prescription drugs from community pharmacies. The medication groups were based on Anatomical Therapeutic Chemical (ATC) classification codes (Table SII). Sequential ordering was analysed separately by treatment type (conventional systemic medications, biologics, or the small molecule inhibitor apremilast) and by individual medications belonging to each treatment type. Medications in the analyses only included treatments reimbursed in Finland during the observational period. This included, for conventional systemic treatment the oral immunosuppressants acitretin, cyclosporine, and methotrexate; for biologics adalimumab, brodalumab, certolizumab pegol, etanercept, ixekizumab, secukinumab, and ustekinumab; for small molecule inhibitors, apremilast. The first-line treatment was defined as the first treatment initiated after the index date. A change in treatment line was defined as the initiation of a medication not used during the observation period, that being conventional, biologic or apremilast (at the 7-digit ATC-code level). Two treatments initiated on the same day were considered a combination treatment.
Phototherapy was defined based on the Nordic Medico-Statistical Committee (NOMESCO) Classification of Surgical Procedures (WXQ20-1, WXQ24, WXQ26-7, WXQ40-4, WXQ99).
Statistical analyses
Demographic characteristics, comorbidities, and treatments in the total cohort were analysed using descriptive statistics. Categorical variables were presented as number of observations and proportions. Continuous variables were reported as mean with standard deviation (SD) and median [interquartile range].
Statistical comparisons of the prevalence of comorbidities in the subgroup of biologic starters and non-biologic starters were performed using the Pearson χ2 test for unpaired data. Statistical comparisons of the pharmacological treatments in the subgroup of biologic starters before and after the initiation of the first biologic were performed using the McNemar test for paired data. The statistical analyses were conducted using R (version 4.0.3., http://www.r-project.org).
RESULTS
Demographics of the study cohort
The total cohort consisted of 41,456 patients ≥ 18 years old who received a diagnosis of psoriasis in the secondary public healthcare setting in Finland from 2012 through 2018 (Table I), representing 0.9% of the total Finnish adult population. Slightly more than half of the patients were men (54.1%). The follow-up time in the total cohort was 7.0 years, and the mean (SD) age was 59.2 (17.2) years.
| Characteristics | Total cohort (n = 41,456) | Biologic starters (n = 1,297) | p - valuea |
| Sex, n (%) | |||
| Female | 19,012 (45.9) | 471 (36.3) | – |
| Male | 22,444 (54.1) | 826 (63.7) | – |
| Age – continuous, mean (SD) | 59.24 (17.22) | 51.83 (13.84) | – |
| Median [IQR] | 61.23 [47.50, 71.55] | 52.58 [41.80, 62.11] | – |
| Selected comorbidities, n (%) | |||
| Based on ICD-10 codes | |||
| Essential (primary) hypertension | 13,356 (32.2) | 358 (27.6) | < 0.001 |
| Arthropathy | 13,195 (31.8) | 419 (32.3) | 0.731 |
| Dorsopathies | 12,205 (29.4) | 443 (34.2) | < 0.001 |
| Acute upper respiratory infections | 10,185 (24.6) | 379 (29.2) | < 0.001 |
| Dermatitis and eczema | 8,574 (20.7) | 228 (17.6) | 0.006 |
| Type 2 diabetes mellitus | 7,420 (17.9) | 192 (14.8) | 0.004 |
| Osteoarthritis | 7,326 (17.7) | 207 (16.0) | 0.108 |
| Severe ischaemic arrhythmias | 5,848 (14.1) | 115 (8.9) | < 0.001 |
| Hypercholesterolaemia | 5,761 (13.9) | 148 (11.4) | 0.010 |
| Influenza and pneumonia | 5,412 (13.1) | 142 (10.9) | 0.025 |
| Arthropathic psoriasis | 6,186 (14.9) | 651 (50.2) | < 0.001 |
| Distal interphalangeal psoriatic arthropathy | 376 (0.9) | 49 (3.8) | <0.001 |
| Other lower respiratory infections | 5,198 (12.5) | 156 (12.0) | 0.602 |
| Cancer | 5,089 (12.3) | 68 (5.2) | < 0.001 |
| Asthma | 4,101 (9.9) | 119 (9.2) | 0.405 |
| Major depressive disorder | 4,046 (9.8) | 152 (11.7) | 0.018 |
| Any mental disorder | 11,325 (27.3) | 328 (25.3) | 0.102 |
| Heart failure | 2,745 (6.6) | 39 (3.0) | < 0.001 |
| Haemorrhagic or embolic stroke | 2,711 (6.5) | 45 (3.5) | < 0.001 |
| Chronic obstructive pulmonary disease | 2,290 (5.5) | 44 (3.4) | < 0.001 |
| Gout | 1,781 (4.3) | 50 (3.9) | 0.468 |
| Kidney diseases | 1,647 (4.0) | 34 (2.6) | 0.014 |
| Crohn disease | 476 (1.1) | 43 (3.3) | < 0.001 |
| Ulcerative colitis | 736 (1.8) | 37 (2.9) | 0.004 |
| Crohn’s disease or ulcerative colitis | 1,077 (2.6) | 64 (4.9) | < 0.001 |
| Rheumatoid arthritis | 1,374 (3.3) | 108 (8.3) | < 0.001 |
| Based on healthcare specialty code, n (%) | |||
| Skin and allergy | 23,487 (56.7) | 1,127 (86.9) | < 0.001 |
| Psychiatry | 5,070 (12.2) | 176 (13.6) | 0.146 |
| Internal medicine | 24,353 (58.7) | 1019 (78.6) | < 0.001 |
| Oncology | 2,210 (5.3) | 30 (2.3) | < 0.001 |
| Ophthalmology | 9,648 (23.3) | 261 (20.1) | 0.007 |
| ap-value refers to a comparison between biologic starters and non-biologic starters (n=40,159). | |||
| ICD-10: International Classification of Diseases, 10th Revision; IQR: interquartile range. | |||
The most common comorbidities in the total cohort were essential hypertension, arthropathy, dorsopathy, acute respiratory infections, dermatitis and eczema (prevalence 20.7–32.2%). PsA was diagnosed in 14.9% of the cohort patients, IBD were diagnosed in 2.6%, with ulcerative colitis comprising 1.8% and Crohn’s disease 1.1%.
Treatment patterns in the total cohort
Conventional systemic medications were used by 28.9% of the patients in secondary care during the whole observation period (Table II). Methotrexate was the most common treatment, followed by acitretin. Cyclosporine was the least common. Biologics were used by 7.3% of patients, with adalimumab being the most used. Ustekinumab, etanercept, and secukinumab were used in nearly equal percentages of patients. Of the biologics certolizumab pegol was the least commonly used treatment. Apremilast was used by 0.8% of the patients in the cohort.
| Total cohort (n = 41,456) n (%) | Biologic starters (n = 1,297) | p-valuea | ||
| Before biologic n (%) | After biologic n (%) | |||
| Conventional or biologic | 12,827 (30.9) | 1,083 (83.5) | 1,297 (100.0) | – |
| Conventional | 11,987 (28.9) | 1,083 (83.5) | 516 (39.8) | < 0.001 |
| Methotrexate | 8,645 (20.9) | 907 (69.9) | 469 (36.2) | < 0.001 |
| Acitretin | 5,042 (12.2) | 426 (32.8) | 28 (2.2) | < 0.001 |
| Cyclosporine | 907 (2.2) | 276 (21.3) | 43 (3.3) | < 0.001 |
| Biologicb | 3,030 (7.3) | 0 (0.0) | 1,297 (100.0) | – |
| Adalimumab | 1,515 (3.7) | 0 (0.0) | 576 (44.4) | – |
| Ustekinumab | 954 (2.3) | 0 (0.0) | 461 (35.5) | – |
| Etanercept | 817 (2.0) | 0 (0.0) | 249 (19.2) | – |
| Secukinumab | 810 (2.0) | 0 (0.0) | 425 (32.8) | – |
| Certolizumab pegol | 177 (0.4) | 0 (0.0) | 68 (5.2) | – |
| Apremilast | 321 (0.8) | 29 (2.2) | 27 (2.1) | 0.8918 |
| Topical treatments | 35,889 (86.6) | 1,228 (94.7) | 1,084 (83.6) | < 0.001 |
| Antipsoriatics | 20,926 (50.5) | 935 (72.1) | 491 (37.9) | < 0.001 |
| Calcitriol | 3,301 (8.0) | 200 (15.4) | 33 (2.5) | < 0.001 |
| Calcipotriol | 18,831 (45.4) | 803 (61.9) | 473 (36.5) | < 0.001 |
| Corticosteroids, dermatological preparations | 31,597 (76.2) | 1,075 (82.9) | 875 (67.5) | – |
| Corticosteroids, weak (group I) | 3,573 (8.6) | 99 (7.6) | 69 (5.3) | 0.009 |
| Corticosteroids, moderately potent (group II) | 12,608 (30.4) | 442 (34.1) | 318 (24.5) | < 0.001 |
| Corticosteroids, potent (group III) | 22,767 (54.9) | 686 (52.9) | 485 (37.4) | < 0.001 |
| Corticosteroids, very potent (group IV) | 10,829 (26.1) | 452 (34.8) | 335 (25.8) | < 0.001 |
| Betamethasone-salicylic acid | 13,765 (33.2) | 583 (44.9) | 362 (27.9) | < 0.001 |
| Emollients | 24,200 (58.4) | 916 (70.6) | 867 (66.8) | 0.011 |
| Other treatments | ||||
| Antiemetics and antinauseants | 936 (2.3) | 13 (1.0) | 19 (1.5) | 0.327 |
| Antifungals for dermatologic use | 7,703 (18.6) | 253 (19.5) | 206 (15.9) | 0.006 |
| Antibacterials for systemic use | 35,425 (85.5) | 977 (75.3) | 939 (72.4) | 0.080 |
| Anti-infectives for systemic use | 4,285 (10.3) | 99 (7.6) | 103 (7.9) | 0.794 |
| Phototherapyc | 3,549 (8.6) | 262 (20.2) | 37 (2.9) | < 0.001 |
| ap - value refers to a comparison between biologic starters before and after the initiation of the biologic. bAdalimumab, brodalumab, certolizumab pegol, etanercept, ixekizumab, secukinumab, ustekinumab were the medications that were reimbursable for the treatment of psoriasis in Finland during the observation period. cNordic Medico-Statistical Committee (NOMESCO) Classification of Surgical Procedures (WXQ20-1,WXQ24, WXQ26-7, WXQ40-4, WXQ99). | ||||
Of topical treatments, antipsoriatics (vitamin D analogues) were used by 50.5% of the patients, with calcipotriol being more commonly used than calcitriol. Topical corticosteroid preparations were used by approximately 3 in 4 patients in the cohort (76.2%). Of the group receiving topical corticosteroid preparations, group III corticosteroids and betamethasone-salicylic acid were the most frequently used groups of corticosteroid preparations (54.9%), and 1 in 4 patients used very potent (group IV) corticosteroids (26.1%). Reimbursable emollients were used by 58.4% of the patients in the total cohort. Phototherapy was used by 8.6% of patients in the total cohort.
Treatment sequences in the secondary healthcare setting
A total of 14,337 patients had their first diagnosis of psoriasis in the secondary healthcare setting between 1 January 2013, and 31 December 2017 (34.7% of the total cohort; subgroup 1). The mean follow-up time before (2012 onwards) and after (until the end of 2018) the psoriasis diagnosis were 3.3 and 3.8 years, respectively. Of the subgroup 1 patients, 14.2% had used conventional medications and 2.9% had used biologics before the psoriasis diagnosis. The proportions increased to 34.3% (conventional) and 7.1% (biologic) after the psoriasis diagnosis. Conventional medications were the most frequently used medications in the first (90.3% of the subgroup patients) and second (65.4%) treatment lines (Fig. 1). Biologics were used by 30.0% and 71.3% of the subgroup patients in the second and third treatment lines, respectively. Of individual medications, methotrexate was the most used medication in the first and second treatment lines, followed by acitretin. The medication most used in the third treatment line was secukinumab (Fig. 2).
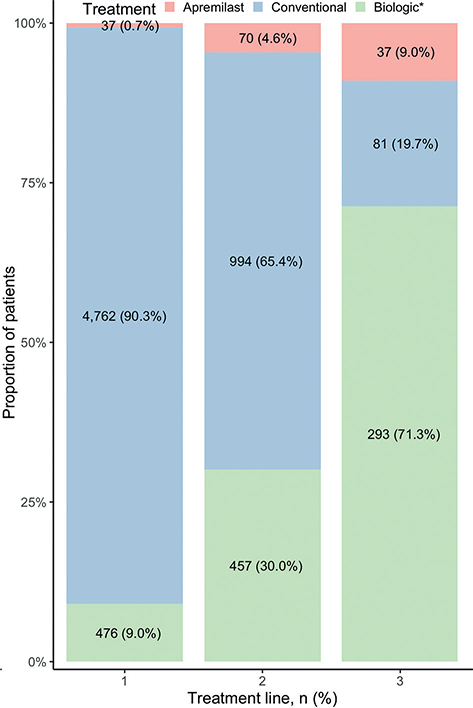
Fig. 1. Treatment lines in the subgroup of patients with their first psoriasis diagnosis (International Classification of Diseases, 10th Revision, code L40.0) in the secondary healthcare setting between 1 January 2013 and 31 December 2018, and with a minimum of 1 year without psoriasis diagnoses. *Biologic includes the combination of biologics with other treatments.
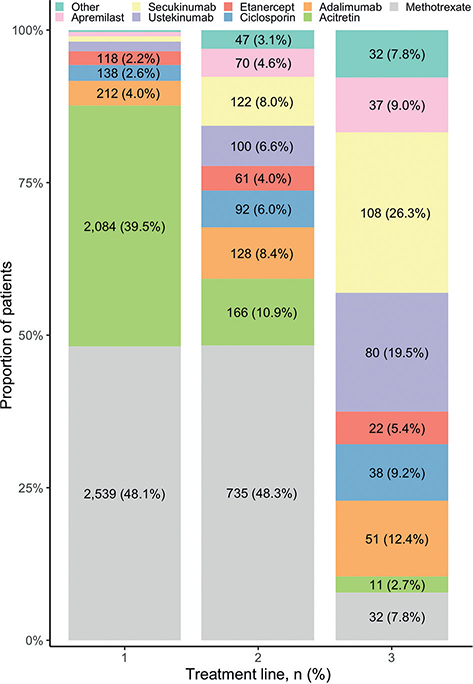
Fig. 2. Individual medications by treatment line on a detailed level in the subgroup of patients with their first psoriasis diagnosis (International Classification of Diseases, 10th Revision, code L40.0) in the secondary healthcare setting between 1 January 2013 and 31 December 2018, and a minimum of 1 year without psoriasis diagnoses. For treatment line 1, the number and proportion of patients using ustekinumab were 83 (1.6%), for secukinumab 47 (0.9%), for apremilast 37 (0.7%), and for other 17 (0.3%). Note: apremilast and combinations of biologics with other treatments were categorized into the use of the specific biologic.
Adalimumab was the most used biologic in the first and second treatment line (44.5% and 28.0% of biologic users, respectively). In the second treatment line both secukinumab and ustekinumab were commonly used biologics. Ustekinumab and secukinumab were the most used biologics in the third treatment line.
Demographics of biologic starters and their treatment patterns
A total of 1,297 patients (3.1% of the total cohort; subgroup 2 biologic starters) initiated a biologic during the observation period (Table I). Biologic starters were younger (mean age 51.8 years) and more often men (63.7%) than patients in the total cohort. The mean follow-up time before and after the initiation of the biologic was 3.6 and 3.4 years, respectively.
The prevalence of PsA, Crohn’s disease, ulcerative colitis, RA, dorsopathies, acute upper respiratory infections, and major depressive disorder (MDD) was higher in the biologic starter group compared with the total cohort (p < 0.001, except p = 0.004 for ulcerative colitis and p = 0.018 for major depressive disorder; Table I and Table SIII). The biologic starters also had more healthcare resource-use related to skin or allergy specialties as well as to internal medicine than did patients in the total cohort (p < 0.001).
Adalimumab (44.4%), ustekinumab (35.5%), and secukinumab (32.8%) were the most used biologics in subgroup 2 biologic starters during the observation period. Among the biologic starters, 83.5% of patients had used a conventional medication before the initiation of a biologic. After the initiation of the biologic, the use of conventional medication decreased to 39.8% (p < 0.001), as did the use of antipsoriatics, corticosteroids preparations, and emollients. Furthermore, the use of phototherapy decreased from 20.2% to 2.9% (p < 0.001; Table II).
DISCUSSION
This is the first nationwide study of patients with psoriasis and their treatment patterns in real-world clinical practice in Finland. The population-based cohort included 41,456 adults with a diagnosis of psoriasis in the secondary healthcare setting from 2012 through 2018, providing a comprehensive representation of patients with moderate to severe psoriasis in Finland. Patients in the cohort had a wide range of comorbidities. The treatment of psoriasis in this cohort was largely based on topical and conventional systemic medications. Biologics were used by 7.3% of patients, mostly in second- and third-line treatment.
The reported prevalence of psoriasis varies widely (1–5% in Europe) depending on the geographical area, definition, and methodology used for estimation (2). In Finland, the prevalence of psoriasis in the adult population was estimated at 2.1% based on the Northern Finland Birth Cohort 1966 (22). The cohort in this study represented 0.9% of the Finnish adult population. Overall, the ICD-10 code L40.0 has been shown to be a valid approach for identifying patients with psoriasis in the Finnish registries (23). As data in this study were from the secondary healthcare setting, the cohort represents mainly patients with moderate to severe disease. The reason for this is that patients with milder disease tend to be treated within the primary care setting and thus not included in the CRHC.
Psoriasis is not only a disease affecting skin and joints, but a systemic inflammatory disorder that has been associated with various comorbidities (8, 15). Patients with psoriasis are often multimorbid, although the relationship and the direction of causality between psoriasis and associated comorbidities is not well understood (15). In this cohort, the most common comorbidities during the observation period were essential hypertension (32.2%), arthropathy (31.8%), and dorsopathy (29.4%). The association between hypertension and psoriasis has also been identified in previous studies (24, 25). PsA was diagnosed in 14.9% of the patients in the total cohort. In previous studies, PsA has been observed in 10–40% of patients with psoriasis, but the diagnostic criteria varied (26, 27). IBD, for which patients with psoriasis may be at 4 times the risk compared with the general population (28), were diagnosed in 2.6% of the patients. In comparison, the prevalence of IBD in the general population was 0.75% in Finland in 2008 (29).
Previous studies have shown an association between psoriasis and mental disorders (10, 11). A meta-analysis estimated that more than 10% of patients with psoriasis are diagnosed with clinical depression, and that twice as many have depressive symptoms (10). In this cohort, 27.3% of the patients were diagnosed with a mental disorder, with MDD being the most common diagnosis (9.8%). In a previous Finnish registry study, at least 1 mental disorder was diagnosed in 19.1% of patients with psoriasis (30). The prevalence of MDD in the total cohort was almost identical to the estimated prevalence of MDD in Finland in 2011 (31). Thus, the prevalence of schizophrenia was also similar to estimates in the general Finnish population, although previous studies have suggested an association between schizophrenia and psoriasis (32, 33).
It should be noted that the prevalence estimates of comorbidities in the study were based on ICD-10 codes recorded as primary or secondary causes for a healthcare visit. It is well known that some diseases are underdiagnosed, e.g. metabolic syndrome components and mental disorders. Therefore the true prevalence of those conditions in patients with psoriasis may be higher. In addition, the prevalence of many comorbidities increases with patient age. Thus, the prevalence in the cohort (mean age 59 years) cannot be directly compared with the general Finnish population (mean age 43 years). Furthermore, it is expected that the prevalence of comorbidities in the study population increases during the observation period.
Although several reports on real-world treatment patterns in patients with psoriasis using biologics have been published, limited nationally representative data exist on psoriasis treatment patterns in general (34–37). In Finland, the recommended first-line systemic treatments for severe psoriasis are oral immunosuppressants acitretin, cyclosporine, and methotrexate (14). In this cohort, these medications were used by 28.9% of the patients during the observation period. In the subgroup of patients with the first psoriasis diagnosis occurring from 2013 to 2018 and having a mean of 3.3 years without a psoriasis diagnosis (n = 14,337), conventional medications were the most frequently used systemic treatments in first- and second-line treatments. In comparison, a Danish registry study including patients with psoriasis of all severities indicated that 15% used conventional medications between 2003 and 2012 (38). The observed differences in medication use can be explained by the local care guidelines and varying reimbursement practices between countries.
According to the Finnish Current Care Guidelines for Psoriasis and the reimbursement criteria by the Social Insurance Institution of Finland, biologics can be used for patients with severe psoriasis who have not responded to first-line systemic treatments or phototherapy (14). However, the order in which individual biologics should be taken is not defined (14). In the total cohort, biologics were used by 7.3% of the patients and 1,297 patients (3.1%) initiated a biologic during the observation period. Adalimumab and ustekinumab were the most frequently used biologics, in line with studies reported from Denmark, the UK and the Republic of Ireland (37, 39). Secukinumab became reimbursable for the psoriasis treatment several years later than adalimumab and ustekinumab, likely explaining why it is most often used in the third line. As expected, biologics were mostly used as second- and third-line treatment, although some patients (9.0%) used a biologic as the first-line treatment. It should be noted that we did not have data available on the indication for the use of the biologic (i.e. some patients may use biologics for indications other than psoriasis). This is also supported by the finding that biologic starters had more comorbidities for which biologics are typically prescribed (PsA, IBD, and RA) than did patients in the total cohort.
The use of conventional medications was more common in biologic starters (83.5% before the initiation of the biologic) than in the total cohort. However, this decreased significantly after the initiation of a biologic (39.8%). The conventional medications most frequently used by patients who later initiated biologics were methotrexate (69.9%), acitretin (32.8%), and cyclosporine (21.3%). Methotrexate is also reported to be the most widely used conventional treatment in other European studies (39, 40). The use of cyclosporine before a biologic was more common in a study conducted in the Netherlands, although its use has decreased in recent years (40).
Remarkably, the use of all topical treatments decreased significantly after the initiation of a biologic. The use of phototherapy also decreased from 20.2% before to 2.9% after the initiation of a biologic. In addition, healthcare resource utilization related to specialty skin or allergy treatments decreased significantly after the initiation of a biologic. This suggests that biologics not only effectively treat psoriasis symptoms, but also reduce the burden of disease for patients in terms of decreasing the need for other laborious and time-consuming treatments.
The major strengths of this registry study include the large cohort size and nationwide coverage. Furthermore, all Finnish citizens have equal access to tax-funded, high-quality public healthcare, and individual-level data on treatment (e.g. healthcare visits and drug purchases) are available from nationwide registries. Thus, there is a minimal selection bias, and the results are generalizable to the population level. Limitations of the study include lack of detailed clinical information e.g. data on disease severity and treatment outcomes. It should be noted that phototherapy may not be systematically recorded by operation codes, which will result in a possible underestimation of the number of patients using phototherapy. In addition, the 7-year follow-up period is relatively short for assessing the comorbidity burden associated with psoriasis and observing uncommon comorbidities. Analyses on pharmacological treatments and emollients were based on purchases of nationally reimbursed prescription medicines, and thus exclude over-the-counter drugs and drugs funded by municipalities e.g. drugs administered in hospitals, such as intravenous infliximab. Overall, the treatment landscape has changed during the most recent years with the introduction of new biologics and biosimilar drugs. Thus, the current treatment patterns may differ from the results presented in this study.
This study provides a population-based overview of patients with moderate to severe psoriasis during a period overlapping the introduction of several new biologics for the treatment of psoriasis. These results form a framework for the evaluation and development of care practices in the changing treatment landscape of psoriasis. With the increasing number of new treatment options available and accumulation of evidence for their use in clinical practice, psoriasis treatment is expected to shift toward more targeted care based on each patient’s individual needs.
ACKNOWLEDGEMENTS
Heidi Loponen from MedEngine Oy is acknowledged for medical writing.
The design, study conduct, and financial support for the study were provided by AbbVie. AbbVie participated in the interpretation of data, review, and approval of the publication. No honoraria or payments were made for authorship.
REFERENCES
- Boehncke WH, Schön MP. Psoriasis. Lancet Lond Engl 2015; 386: 983–994.
- Parisi R, Iskandar IYK, Kontopantelis E, Augustin M, Griffiths CEM, Ashcroft DM. National, regional, and worldwide epidemiology of psoriasis: systematic analysis and modelling study. BMJ 2020; 369: m1590.
- Armstrong AW, Read C. Pathophysiology, clinical presentation, and treatment of psoriasis: a review. JAMA 2020; 323: 1945–1960.
- AlQassimi S, AlBrashdi S, Galadari H, Hashim MJ. Global burden of psoriasis – comparison of regional and global epidemiology, 1990 to 2017. Int J Dermatol 2020; 59: 566–571.
- Peng C, Xu X, Chen W, Li X, Yi X, Ding Y, et al. Epidemiological variations in the global burden of psoriasis, an analysis with trends from 1990 to 2017. Front Med 2021; 8: 24.
- Yeung H, Takeshita J, Mehta NN, Kimmel SE, Ogdie A, Margolis DJ, et al. Psoriasis severity and the prevalence of major medical comorbidity: a population-based study. JAMA Dermatol 2013; 149: 1173–1179.
- Augustin M, Reich K, Glaeske G, Schaefer I, Radtke M. Co-morbidity and age-related prevalence of psoriasis: analysis of health insurance data in Germany. Acta Derm Venereol 2010; 90: 147–151.
- Takeshita J, Grewal S, Langan SM, Mehta NN, Ogdie A, Van Voorhees AS, et al. Psoriasis and comorbid diseases: epidemiology. J Am Acad Dermatol 2017; 76: 377–390.
- Bhosle MJ, Kulkarni A, Feldman SR, Balkrishnan R. Quality of life in patients with psoriasis. Health Qual Life Outcomes 2006; 4: 35.
- Dowlatshahi EA, Wakkee M, Arends LR, Nijsten T. The prevalence and odds of depressive symptoms and clinical depression in psoriasis patients: a systematic review and meta-analysis. J Invest Dermatol 2014; 134: 1542–1551.
- Dalgard FJ, Gieler U, Tomas-Aragones L, Lien L, Poot F, Jemec GBE, et al. The psychological burden of skin diseases: a cross-sectional multicenter study among dermatological out-patients in 13 European countries. J Invest Dermatol 2015; 135: 984–991.
- Menter A, Korman NJ, Elmets CA, Feldman SR, Gelfand JM, Gordon KB, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: section 6. Guidelines of care for the treatment of psoriasis and psoriatic arthritis: case-based presentations and evidence-based conclusions. J Am Acad Dermatol 2011; 65: 137–174.
- Pathirana D, Ormerod AD, Saiag P, Smith C, Spuls PI, Nast A, et al. European S3-guidelines on the systemic treatment of psoriasis vulgaris. J Eur Acad Dermatol Venereol 2009; 23: 1–70.
- Psoriasis and Psoriatic Arthritis. Current Care Guidelines. Working group set up by the Finnish Medical Society Duodecim, the Finnish Dermatological Society and the Finnish Society for Rheumatology. Helsinki: The Finnish Medical Society Duodecim, 2022 (cited 2022, November 25). Available from: www.kaypahoito.fi/hoi50062.
- Griffiths CEM, Armstrong AW, Gudjonsson JE, Barker JNWN. Psoriasis. The Lancet 2021; 397: 1301–1315.
- Sbidian E, Chaimani A, Garcia-Doval I, Do G, Hua C, Mazaud C, et al. Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis. Cochrane Database Syst Rev 2017; 12: CD011535.
- Feldman SR, Kaura S, Li S, Tencer T. Treatment persistence in psoriasis patients initiated on apremilast, oral systemics, or biologic therapies. Value Health 2017; 20: A805.
- Rønholt K, Iversen L. Old and new biological therapies for psoriasis. Int J Mol Sci 2017; 18: 2297.
- Ragnarson Tennvall G, Hjortsberg C, Bjarnason A, Gniadecki R, Heikkilä H, Jemec GBE, et al. Treatment patterns, treatment satisfaction, severity of disease problems, and quality of life in patients with psoriasis in three Nordic countries. Acta Derm Venereol 2013; 93: 442–445.
- Mustonen A, Mattila K, Leino M, Koulu L, Tuominen R. Psoriasis causes significant economic burden to patients. Dermatol Ther 2014; 4: 115–124.
- Könönen M, Torppa J, Lassus A. An epidemiological survey of psoriasis in the greater Helsinki area. Acta Derm Venereol 1986; Suppl 124: 1–10.
- Sinikumpu SP, Huilaja L, Jokelainen J, Koiranen M, Auvinen J, Hägg PM, et al. High prevalence of skin diseases and need for treatment in a middle-aged population. A Northern Finland Birth Cohort 1966 study. PloS One 2014; 9: e99533.
- Haverinen S, Vihervaara A, Löyttyniemi E, Peltonen S, Koulu L, Tasanen K, et al. Validation of psoriasis diagnoses recorded in Finnish biobanks. Acta Derm Venereol 2020; 100: adv00297.
- Warren RB, Smith CH, Yiu ZZN, Ashcroft DM, Barker JNWN, Burden AD, et al. Differential drug survival of biologic therapies for the treatment of psoriasis: a prospective observational cohort study from the British Association of Dermatologists Biologic Interventions Register (BADBIR). J Invest Dermatol 2015; 135: 2632–2640.
- Duan X, Liu J, Mu Y, Liu T, Chen Y, Yu R, et al. A systematic review and meta-analysis of the association between psoriasis and hypertension with adjustment for covariates. Medicine (Baltimore) 2020; 99: e19303.
- Ritchlin CT, Colbert RA, Gladman DD. Psoriatic arthritis. N Engl J Med 2017; 376: 957–970.
- Gladman DD, Antoni C, Mease P, Clegg DO, Nash P. Psoriatic arthritis: epidemiology, clinical features, course, and outcome. Ann Rheum Dis 2005; 64: ii14–17.
- Fu Y, Lee CH, Chi CC. Association of psoriasis with inflammatory bowel disease: a systematic review and meta-analysis. JAMA Dermatol 2018; 154: 1417–1423.
- Jousimaa J, Alenius H, Atula S, Kattainen A, Kunnamo I, Pelttari H, et al. [Phisicians’ Handbook]. Duodecim; 2017.
- Huilaja L, Tiri H, Jokelainen J, Timonen M, Tasanen K. Patients with hidradenitis suppurativa have a high psychiatric disease burden: a Finnish nationwide registry study. J Invest Dermatol 2018; 138: 46–51.
- Markkula N, Suvisaari J, Saarni SI, Pirkola S, Peña S, Saarni S, et al. Prevalence and correlates of major depressive disorder and dysthymia in an eleven-year follow-up – results from the Finnish Health 2011 Survey. J Affect Disord 2015; 173: 73–80.
- Perälä J, Suvisaari J, Saarni SI, Kuoppasalmi K, Isometsä E, Pirkola S, et al. Lifetime prevalence of psychotic and bipolar I disorders in a general population. Arch Gen Psychiatry 2007; 64: 19–28.
- Ungprasert P, Wijarnpreecha K, Cheungpasitporn W. Patients with psoriasis have a higher risk of schizophrenia: a systematic review and meta-analysis of observational studies. J Postgrad Med 2019; 65: 141–145.
- Svedbom A, Dalén J, Mamolo C, Cappelleri JC, Petersson IF, Ståhle M. Treatment patterns with topicals, traditional systemics and biologics in psoriasis – a Swedish database analysis. J Eur Acad Dermatol Venereol 2015; 29: 215–223.
- Murage MJ, Kern DM, Chang L, Sonawane K, Malatestinic WN, Quimbo RA, et al. Treatment patterns among patients with psoriasis using a large national payer database in the United States: a retrospective study. J Med Econ 2018; 1–9.
- Hjalte F, Carlsson KS, Schmitt-Egenolf M. Sustained Psoriasis Area and Severity Index, Dermatology Life Quality Index and EuroQol-5D response of biological treatment in psoriasis: 10 years of real-world data in the Swedish National Psoriasis Register. Br J Dermatol 2018; 178: 245–252.
- Egeberg A, Ottosen MB, Gniadecki R, Broesby-Olsen S, Dam TN, Bryld LE, et al. Safety, efficacy and drug survival of biologics and biosimilars for moderate-to-severe plaque psoriasis. Br J Dermatol 2018; 178: 509–519.
- Egeberg A, Andersen YMF, Thyssen JP. Prevalence and characteristics of psoriasis in Denmark: findings from the Danish skin cohort. BMJ Open 2019; 9: e028116.
- Davison NJ, Warren RB, Mason KJ, McElhone K, Kirby B, Burden AD, et al. Identification of factors that may influence the selection of first-line biological therapy for people with psoriasis: a prospective, multicentre cohort study. Br J Dermatol 2017; 177: 828–836.
- van den Reek JMPA, Seyger MMB, van Lümig PPM, Driessen RJB, Schalkwijk CJM, Berends MAM, et al. The journey of adult psoriasis patients towards biologics: past and present – results from the BioCAPTURE registry. J Eur Acad Dermatol Venereol 2018; 32: 615–623.