ORIGINAL REPORT
The Impact of Atopic Dermatitis on Sexual Function and Reproductive Desires in Women
Juan-Angel RODRIGUEZ-POZO1, Trinidad MONTERO-VILCHEZ1,2, Pablo DIAZ CALVILLO1, Raquel SANABRIA DE LA TORRE2, Clara UREÑA-PANIEGO1, Arena RAMIREZ-MUÑOZ2 and Salvador ARIAS-SANTIAGO1,2,4
1Dermatology Department, Virgen de las Nieves University Hospital, Granada, 2Instituto de Investigación Biosanitaria ibs.GRANADA, Granada, 3Biochemistry Department, Faculty of Medicine, University of Granada, Granada, and 4Dermatology Department, Faculty of Medicine, University of Granada, Granada, Spain
Atopic dermatitis is a prevalent skin condition that affects up to 17% of adult population. It can lead to itching, pain, and other symptoms such as sleep disturbance, anxiety, and depression. Due to its high prevalence and limiting symptoms, atopic dermatitis often has a great impact on patients’ quality of life but there is scarce information regarding how atopic dermatitis affects women’s sexual health and reproductive desires. The purpose of this article was to assess the impact of atopic dermatitis on sexual function and reproductive wishes in women. A cross-sectional study was conducted from February to March 2022. A total of 102 women with atopic dermatitis were recruited through online questionnaires sent through the Spanish Atopic Dermatitis Association; 68.6% of the patients acknowledged impairment in sexual function, especially those with more severe disease and those with genital and gluteal involvement. In addition, 51% of the women considered that atopic dermatitis may have an influence on their gestational desire, particularly those with gluteal involvement. In conclusion, atopic dermatitis has a great impact on sexual function and reproductive desires in women.
SIGNIFICANCE
Atopic dermatitis (AD) has a great impact on patients’ quality of life (QoL) but little is known about the impact of this disease on women’s sexual health and reproductive desires. In this article it is observed that AD disrupts sexual function and has a negative influence on reproductive desires. Greater disease severity and the presence of lesions on the gluteal and genital area are related to poorer QoL, sexual dysfunction, and lower reproductive desires. This article highlights the need to address these issues in the dermatological consultation and to provide patient-oriented treatment.
Key words: atopic dermatitis; sexual function; reproductive desire; quality of life.
Citation: Acta Derm Venereol 2024; 104: adv35107. DOI https://doi.org/10.2340/actadv.v104.35107.
Copyright: 2024 © The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Dec 18, 2023; Accepted: Apr 29, 2024; Published: Jun 11, 2024
Corr: Trinidad Montero-Vilchez, Dermatology Department. Avenida de Madrid, 15, ES-18012, Granada, Spain. E-mail: tmonterov@gmail.com
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Atopic dermatitis (AD) is a prevalent skin condition that affects up to 17% of the adult population (1, 2). It can lead to itching, pain, and other symptoms such as sleep disturbance, anxiety, and depression (3).
Due to its high prevalence and limiting symptoms, AD often has a great impact on patients’ quality of life (4, 5). This disease results in severe impairments of functionality across all levels (social, familial, sexual, and occupational) (6), which leads to a decrease in productivity amongst other dramatic consequences (7).
Furthermore, like other skin diseases such as hidradenitis suppurativa, it has been linked to sexual dysfunction (SD) (8). SD encompasses a broad category of organic and psychological conditions characterized by clinically significant impairments in the ability to respond sexually or to experience sexual pleasure (9). However, little is known about the relationship between AD and SD.
Moreover, AD also impacts on the reproductive health of women. It is the most common dermatosis during pregnancy (10, 11), and many patients are undertreated during this period due to fear of side effects (12).
The objective of this study was, thus, to assess the impact of AD on sexual function and reproductive health.
MATERIALS AND METHODS
Design
A cross-sectional study was conducted from February to March 2022. Women patients were recruited through online questionnaires sent to potential participants through the Spanish AD Association (AADA).
Inclusion and exclusion criteria
Women over the age of 18 years were invited to participate. The selection criterion was self-referred diagnosis of AD. Participants were aware of the questionnaire’s anonymity and the use of their data for research purposes. In addition to sexual function, because the study addressed very specific aspects such as gestational desires, the questionnaire was sent only to female patients, excluding men. It was also verified that only women answered the survey asking about gender in the survey itself.
Variables of interest
All the variables were assessed through online questionnaires. Sociodemographic characteristics (age, civil status, education level), smoking, and drinking habits were collected. Disease severity was assessed using the Patient-Oriented SCORing Atopic Dermatitis (PO-SCORAD). The Dermatology Life Quality Index (DLQI), Patient Oriented Eczema Measure (POEM), and World Health Organization Quality of Life (WHOQOL) were used to assess QoL impairment. The presence of SD was evaluated with a numeric rating scale (NRS) for AD impact on sex life, in which participants were asked to measure from 0 to 10 how much the disease affects their sex life, and the Female Sexual Function Index-6 (FSFI-6). Patient were also asked about the impact of AD on their reproductive desires. Psychological impact was measured with the Hospital Anxiety and Depression Scale (HADD and HADA) questionnaires.
Statistical analysis
Descriptive statistics were used to present the sample characteristics. Continuous data were expressed as mean ± standard deviation and qualitative data as relative (absolute) frequency. The Shapiro–Wilk test was used to determine the normality of data distribution and Levene’s test to check the homogeneity of variance. Student’s t-test for independent samples was used to compare differences in continuous parameters between women who think that AD may impact their reproductive desires and those who did not. A χ2 test was used to compare categoric data between these two groups. Pearson’s correlation test was used to evaluate the correlation between continuous variables. Statistical significance was defined as a two-tailed p < 0.05. SPSS version 24.0 (IBM Corp, Armonk, NYc, USA) was used for statistical analyses.
Ethics
The study was approved by the Institutional Review Board of Hospital Universitario Virgen de las Nieves and is in accordance with the Declaration of Helsinki. Patients were aware of the anonymous treatment of their data and gave their informed consent to participate in the study.
RESULTS
Sociodemographic characteristics
A total of 102 women with AD were included (Table I). The mean age of the patients was 30.31 ± 7.75; 61% (61/102) of the participants were married and 65.7% (67/102) had a university education. Some 21.6% (22/102) and 33.3% (34/102) of the participants smoke and drink alcohol respectively. Current treatment of patients is provided in Fig. 1.
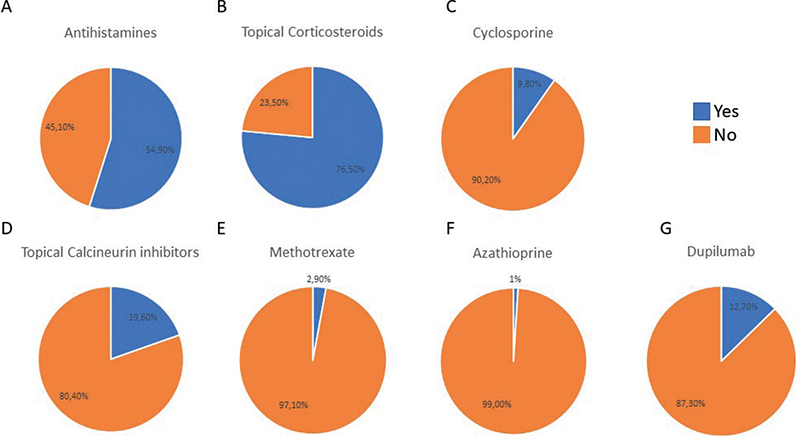
Fig. 1. Current treatment of patients included in the study. (A) antihistamines; (B) topical corticosteroids; (C) cyclosporine (D) topical calcineurin inhibitors; (E) methotrexate; (F) azathioprine; (G) dupilumab.
Disease severity and sexual dysfunction
The mean age of disease debut was 7.38 ± 10.24. The mean PO-SCORAD and POEM were 55.52 ± 19.69 and 15.96 ± 6.73 respectively, showing severe disease.
The mean DLQI score (18.47 ± 7.92) and the mean WHOQOL score (42.98 ± 20.29) indicated a very large impact of AD on patients’ QoL. HADD of 8.36 ± 4.56 and HADA of 9.49 ± 4.19 showed a borderline increase in anxiety and depression in patients with AD.
Regarding sexual function, 68.6% of the participants admitted that AD affected their sexual life. The mean NRS was 5.23 ± 2.16 and the mean FSFI was 16.44 ± 8.99, revealing an impairment of sexual life.
We found a positive association between higher scores in NRS for SD and PO-SCORAD (r = 0.269, p = 0.006), DLQI (r = 0.0518, p < 0.01), number of affected areas (r = 0.257, p = 0.009), and NRS for sleep (r = 0.242, p=0.014). Furthermore, NRS for SD was also associated with WHOQOL (r = – 0.344, p < 0.001) and HAD (r = 0.416, p < 0.001). FSFI was not associated with other severity parameters except with NRS for SD.
Women with gluteal (6.21 vs 4.63, p = 0.007) and genital (6.59 vs 4.74, p = 0.004) involvement showed greater values in NRS for SD.
Reproductive desire
In all, 51% (52/102) of the women thought their AD may influence their reproductive desire (Table II). In our sample, 32.4% (33/102) of women already have 1 child, whereas 42.2% (43/102) of them would like to have more children. In fact, 44.1% (45/102) used mean contraceptive method. Only 28.9% (11/38) of women talked about their gestational desires with their dermatologist.
| Do woman think AD may impact on their gestational desire? | No (n = 50), n (%) | Yes (n = 52), n (%) | p-value* |
| Age | 32.16 (9.17) | 28.54 (5.63) | 0.19 |
| Age of disease debut | 8.86 (11.94) | 5.98 (8.209) | 0.16 |
| Civil Status | |||
| Single | 12/50 (24%) | 25/52 (48.1%) | 0.032* |
| Married | 35/50 (70%) | 26/52 (50%) | |
| Separated | 3/50 (6%) | 1/52 (1.9%) | |
| Educational level | |||
| Primary | 3/50 (6%) | 0 (0%) | 0.355 |
| Secondary | 4/50 (8%) | 5/52 (9.6%) | |
| Professional | 11/50 (22%) | 12/52 (23.1%) | |
| University | 32/50 (64%) | 35/52 (67.3%) | |
| Smoking (yes) | 12/50 (24%) | 10/52 (19.2%) | 0.558 |
| Drinking (yes) | 19/50 (38%) | 15/52 (28.8%) | 0.327 |
| PO-SCORAD mild | 24/50 (48%) | 22/52 (42.3%) | 0.564 |
| PO-SCORAD severe | 26/50 (52%) | 30/52 (57.7%) | |
| Genital involvement (yes) | 11/50 (22%) | 16/52 (31.4%) | 0.287 |
| Gluteal involvement (yes) | 13/50 (26%) | 26/52 (51%) | 0.010* |
| PO-SCORAD | 53.19 (19.50) | 50.78 (19.80) | 0.241 |
| POEM | 15.5 (6.16) | 16.40 (7.27) | 0.499 |
| DLQI | 15.62 (7.35) | 21.21 (7.54) | < 0.001* |
| WHOQOL | 44.83 (22.78) | 41.25 (17.7) | 0.387 |
| HADA | 8.92 (4.17) | 10.04 (4.18) | 0.179 |
| HADD | 7.28 (4.48) | 9.40 (4.45) | 0.018* |
| FSFI-6 | 16.72 (8.70) | 16.18 (9.34) | 0.762 |
| NRS for sexual dysfunction | 3.58 (3.27) | 6.81 (2.22) | < 0.001* |
| Continuous variables are expressed as means (standard deviation) and qualitative variables as absolute (relative) frequencies. PO-SCORAD: Patient-Oriented SCORing Atopic Dermatitis. POEM: Patient Oriented Eczema Measure. DLQI: Dermatology Life Quality Index. WHOQOL: World Health Organization Quality of life. HADA/HADD: Hospital Anxiety and Depression Scale. FSFI-6: Female Sexual Function Index-6. NRS: numeric rating scale. | |||
| *p-value was obtained after using Student’s t-test for independent samples to compare continuous variables and χ2 test to compare categoric variables. | |||
Several differences were observed among women in terms of whether AD might influence their reproductive desire. Most of those who believe that AD had no influence on gestational desire were already married. Significant impairment in gestational desire was also observed in those women with gluteal disease. No other differences were found regarding age, education level, smoking, drinking, PO-SCORAD, or genital disease.
DISCUSSION
In this cross-sectional study, we have studied the impact of AD on sexual function and pregnancy. We have identified several factors associated with worse QoL. We have also determined the strong influence that AD may have on child desire. We have focused on female patients because women often bear the primary physical and emotional burdens associated with reproductive processes, including pregnancy, breastfeeding, childbirth, and postpartum care.
AD is a limiting disease due to its erratic course and the severity of its symptoms (13) and, like other dermatological diseases including psoriasis, hidradenitis suppurative, urticaria, and alopecia areata, it has been associated with severe impairment in quality of life (14–17). In our report, it was observed that the mean DLQI score in patients with AD was high, reflecting a great impact on patients’ QoL as previously reported (18). Also, it has been reported that AD patients often develop sleep disorders, anxiety, depression, low self-esteem, and even suicidal thoughts (19,20). In our study, scales such as HAAD and HADA confirmed a borderline increasement of anxiety and depression in patients with AD.
Concerning the impact of AD on SD, a report evaluating SD in patients with many inflammatory skin diseases, including eczema, observed no difference in SD between the sexes and reported that SD was related to younger age, originating in Southern countries, greater disease severity, having flares on the scalp and on the hands, and the presence of itch (21). Studies conducted in men showed that the prevalence of SD ranged from 6.7% to 57.9% and that patients with genital involvement reported greater disease burden and lower QoL (22, 23). However, there are some limitations in these studies as the presence of SD was only evaluated using the score of question 9 in DLQI or based on treatment prescription. Other studies focusing on women with AD have shown that those with both HE and depression have significantly decreased FSFI scores (24). Our study evaluated the prevalence of SD using FSFI, NRS for SD, and item 9 of the DLQI and observed that more than 2/3 of women suffering from AD had SD and that SD was directly associated with PO-SCORAD, number of affected areas, sleep, and gluteal and genital disease.
Furthermore, in this study we aimed to assess whether AD might have an influence on gestational desire as little has been published on this. We observed that those women with gluteal disease were less willing to get pregnant. No other factors in terms of age, education level, smoking, drinking, PO-SCORAD, or genital disease were observed to have an impact. More studies are needed to confirm these results and to explore the concerns of AD patients regarding pregnancy. In fact, it was especially striking how little women talked about this topic with their dermatologist. Without a doubt, more needs to be done to fully understand this topic and progress towards personalized dermatological attention.
The main limitation of our research is the relatively small sample size. Also, a potential selection bias may exist, as it solely represents individuals engaged with support groups and Internet resources, potentially excluding the elderly, who might have limited Internet usage, or those with lower sociocultural status or apprehension towards new technologies, resulting in potential underrepresentation. In addition, as only women belonging to an association were asked, selection bias related to severity of disease may be present, as those with milder symptoms are not usually affiliated with these groups. Also, patient-reported outcome is commonly higher than that of a doctor. Furthermore, individuals already preoccupied with issues related to AD may have been more inclined to participate in the survey. Nevertheless, the fundamental characteristics of our sample align with those previously documented in the literature, whether derived from hospital-based studies or broader population surveys. Given the limited available information on AD and its impact on sexuality, we posit that this study serves as a meaningful introduction to the issue, laying the groundwork for subsequent investigations.
In conclusion, AD affects QoL, sexuality, and gestational desire. Controllable factors such as the severity and extension of the symptoms enhance this impact. Despite all of this, patients scarcely consult on the issue with a dermatologist. Given this situation, an effort needs to be made by dermatologists to be concerned and to approach patients with AD in a more holistic way, emphasizing psychological and social aspects such as sexuality and reproductive desires.
ACKNOWLEDGEMENTS
This study was approved by the ethics committee of Hospital Universitario Virgen de las Nieves (HC01/0442-N-20). The nature of the study was explained to all participants, who agreed to participate by giving their verbal and written consent. All measurements were non-invasive, and the confidentiality of participants’ data was strictly preserved. This research is part of PhD work of Juan Angel Rodriguez Pozo
REFERENCES
- Nutten S. Atopic dermatitis: global epidemiology and risk factors. Ann Nutr Metab 2015; 66: 8–16.
- Bylund S, Von Kobyletzki LB, Svalstedt M, Svensson Å. Prevalence and incidence of atopic dermatitis: a systematic review. Acta Derm Venereol 2020; 100: 320–329.
- Yu SH, Silverberg JI. Association between atopic dermatitis and depression in US adults. J Invest Dermatol 2015; 135: 3183–3186.
- Eckert L, Gupta S, Amand C, Gadkari A, Mahajan P, Gelfand JM. The burden of atopic dermatitis in US adults: health care resource utilization data from the 2013 National Health and Wellness Survey. J Am Acad Dermatol 2018; 78: 54–61.
- Silverberg JI, Gelfand JM, Margolis DJ, Boguniewicz M, Fonacier L, Grayson MH, et al. Patient burden and quality of life in atopic dermatitis in US adults: a population-based cross-sectional study. Ann Allergy Asthma Immunol 2018; 121: 340–347.
- Hsieh BJ, Shen D, Hsu CJ, Chan TC, Cho YT, Tang CH, et al. The impact of atopic dermatitis on health-related quality of life in Taiwan. J Formos Med Assoc 2022; 121: 269–277.
- Eckert L, Gupta S, Amand C, Gadkari A, Mahajan P, Gelfand JM. Impact of atopic dermatitis on health-related quality of life and productivity in adults in the United States: an analysis using the National Health and Wellness Survey. J Am Acad Dermatol 2017; 77: 274–279.
- Kaundinya T, Rakita U, Silverberg JI. Prevalence, predictors, and longitudinal course of sexual dysfunction in adults with atopic dermatitis. Dermatitis 2023; 34: 233–240.
- Mitchell KR, Jones KG, Wellings K, Johnson AM, Graham CA, Datta J, et al. Estimating the prevalence of sexual function problems: the impact of morbidity criteria. J Sex Res 2016; 53: 955–967.
- Russell L, Ugalde A, Milne D, Krishnasamy M, O Seung Chul E, Austin DW, et al. Feasibility of an online mindfulness-based program for patients with melanoma: study protocol for a randomised controlled trial. Trials 2018; 19: 223.
- Lehrhoff S, Keltz M, The P, Perelman RO. Specific dermatoses of pregnancy and their treatment. Dermatol Ther 2013; 26: 274–284.
- Babalola O, Strober BE. Treatment of atopic dermatitis in pregnancy. Dermatol Ther 2013; 26: 293–301.
- Eichenfield LF, Tom WL, Chamlin SL, Feldman SR, Hanifin JM, Simpson EL, et al. Guidelines of care for the management of atopic dermatitis: section 1. Diagnosis and assessment of atopic dermatitis. J Am Acad Dermatol 2014; 70: 338–351.
- Goldburg SR, Strober BE, Payette MJ. Hidradenitis suppurativa: epidemiology, clinical presentation, and pathogenesis. J Am Acad Dermatol 2020; 182: 1045–1058.
- Nabieva K, Vender R. Quality of life and body region affected by psoriasis: a systematic review. Actas Dermosifiliogr 2023; 114: T33–T38.
- Gonçalo M, Gimenéz-Arnau A, Al-Ahmad M, Ben-Shoshan M, Bernstein JA, Ensina LF, et al. The global burden of chronic urticaria for the patient and society. Br J Dermatol 2021; 184: 226–236.
- Villasante Fricke AC, Miteva M. Epidemiology and burden of alopecia areata: a systematic review. Clin Cosmet Investig Dermatol 2015; 8: 397–403.
- Ali F, Vyas J, Finlay AY. Counting the burden: atopic dermatitis and health-related quality of life. Acta Derm Venereol 2020; 100: 330–340.
- Baurecht H, Welker C, Baumeister SE, Weidnger S, Meisinger C, Leitzmann MF, et al. Relationship between atopic dermatitis, depression and anxiety: a two-sample Mendelian randomization study. Br J Dermatol 2021; 185: 781–786.
- Talamonti M, Galluzzo M, Silvaggio D, Lombardo P, Tartaglia C, Bianchi L. Quality of life and psychological impact in patients with atopic dermatitis. J Clin Med 2021; 10: 1–9.
- Misery L, Seneschal J, Reguiai Z, Merhand S, Héas S, Huet F, et al. The impact of atopic dermatitis on sexual health. J Eur Acad Dermatol Venereol 2019; 33: 428–432.
- Ludwig CM, Fernandez JM, Hsiao JL, Shi VY. The interplay of atopic dermatitis and sexual health. Dermatitis 2020; 3: 303–308.
- Linares-Gonzalez L, Lozano-Lozano I, Gutierrez-Rojas L, Lozano-Lozano M, Rodenas-Herranz T, Ruiz-Villaverde R. Sexual dysfunction and atopic dermatitis: a systematic review. Life (Basel) 2021; 11:1314.
- Ergün M, Türel Ermertcan A, Oztürkcan S, Temeltaş G, Deveci A, Dinç G. Sexual dysfunction in patients with chronic hand eczema in the Turkish population. J Sex Med 2007; 4: 1684–1690.