ORIGINAL REPORT
The Potential of Instagram to Reduce Stigmatization of People with Psoriasis: A Randomized Controlled Pilot Study
Simona MASPERO1#, Christopher EBERT1#, Selina MOSER1#, Alexander ZINK2, Pablo SICHERT3, Maximilian SCHIELEIN2, Johanna WEIS2 and Stefanie ZIEHFREUND2,4
1Department of Sport and Health Sciences, 2Department of Dermatology and Allergy, School of Medicine, 3Department of Informatics and 4Institute of General Practice and Health Services Research, School of Medicine, Technical University of Munich, Munich, Germany
#Shared first authorship.
Psoriasis is a stigmatized skin disease. This randomized controlled trial aimed to evaluate an Instagram based stigma-reduction intervention targeting daily Instagram users aged 18 to 49 years without psoriasis. After stratification for baseline characteristics (t0), stigmatization of psoriasis was assessed using a questionnaire and a photo-rating task immediately before (t1) and after (t2) the intervention and two weeks post-intervention (t3). Data from 54 participants, recruited in a university setting and via Instagram, were analysed. For 10 min between t1 and t2, the intervention group (n = 26) and the control group (n = 28) scrolled through two different Instagram accounts. Psoriasis-sensitizing content was displayed to the intervention group while beauty-glorifying posts were shown to the control group. Results indicated significantly less Disease-related Misconceptions in the intervention group in comparison to the control group at t2 (U = 145.50, Z = –3.79, p < 0.001) and at t3 (U = 177.00, Z = –3.25, p = 0.003). Moreover, the intervention group showed a significant reduction over time in Stereotype Endorsement (F(2, 50) = 13.40, p < 0.001, partial η² = 0.35) and Disease-related Misconceptions (χ2(2) = 12.64, p = 0.002). These findings suggest that addressing psoriasis on Instagram has the potential to effectively reduce the related stigmatization. Further studies are necessary to assess the impact of social media on stigmatization concerning psoriasis in more depth.
Key words: psoriasis; social media; social stigma; skin disease; randomized controlled trial.
SIGNIFICANCE
Individuals affected by psoriasis experience external stigmatization. The aim of this study was to develop and evaluate an Instagram-based intervention to reduce such stigmatization among daily Instagram users (aged 18 to 49 years). A psoriasis-sensitizing Instagram account was created and displayed to individuals assigned to the intervention group. Data from 54 participants measured at three time-points (before, immediately after the intervention, and 2-weeks post-intervention) were used to assess the effectiveness of the intervention. A significant reduction in stigmatization was found for the intervention group regarding Stereotype Endorsement and Disease-related Misconceptions. These findings highlight the potential of Instagram in combating stigmatization.
Citation: Acta Derm Venereol 2023; 103: adv3513. DOI https://doi.org/10.2340/actadv.v103.3513.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Accepted: Dec 21, 2022; Published: Mar 23, 2023
Corr: Stefanie Ziehfreund, Public Health, Department of Dermatology and Allergy, Technical University of Munich, School of Medicine, Biedersteiner Str. 29, DE-80802 Munich, Germany. E-mail: stefanie.ziehfreund@tum.de
Competing interests and funding: SZ received travel fees from Novartis. MS has been an advisor and/or received speaker’s honoraria from the following companies: BeiersdorfDermo Medical, Janssen Cilag, Leo Pharma, Novartis. In addition, MS is currently employed by Novartis. AZ has been an advisor and/or received speaker’s honoraria and/or received grants and/or participated in clinical trials of the following companies: AbbVie, Almirall, Amgen, Beiersdorf Dermo Medical, Bencard Allergie, BMS, Celgene, Eli Lilly, GSK, Janssen Cilag, Leo Pharma, Miltenyi Biotec, Novartis, Pfizer, Sanofi-Aventis, Takeda Pharma, UCB Pharma. CE, SM, SM, JW, and PS have no conflict of interest to declare.
INTRODUCTION
In Western Europe, the prevalence for psoriasis was estimated to be 1.9% in 2017, with 2.2% of the German population affected (1). Due to the visual manifestations of the skin disease (e.g. itching areas of skin covered with scales), its concomitant physical diseases (e.g. psoriatic arthritis), and psychological comorbidities (e.g. depression and anxiety), the health-related quality of life (HRQoL) of those affected can be severely impaired (2, 3). The occurrence of mental health problems among people with psoriasis is closely related to ongoing external stigmatization of the skin disease by society (4–6).
In 2014, WHO declared reduction of stigmatization of psoriasis as a global goal (7). Following this, the national project against stigmatization in visible chronic skin diseases (Entstigmatisierung von chronischen sichtbaren Hautkrankheiten; ECHT) was implemented in Germany (8). This project promoted the development and evaluation of stigma-targeting interventions. One approach was to educate the general public in-person about psoriasis; for example, in the form of seminars or by establishing contact between unaffected and affected individuals. Studies demonstrate that these measures can successfully reduce the external stigmatization of psoriasis (9, 10).
Another educational approach encouraged by the WHO is social media (3). User engagement on social media, such as “liking” and/or commenting, is determined by the content format (e.g. emotional pictures, informative text) (11, 12). This can be explained by the binary processing of information by users (12), grounded in the dual processing theory (13). According to this theory, a person’s cognitive appraisal is connected to 2 competing systems in the brain. System 1 triggers reactions defined by subconscious emotions, beliefs, and influences of the context. System 2 drives responses that rely on the calculated evaluation of the indications in a situation (13). Although it is suggested not to assign specific terms to the two systems (14), for reasons of facilitated readability, system 1 reactions are referred to as “intuitive” and system 2 responses as “reflective” in the further course of this study. In line with the dual processing theory, in 2008, Reeder et al. showed that external stigmatization is dependent on situational cues and their intuitive and/or reflective processing (15). In order to induce change, intuitive stigmatization can be manipulated by shaping the autonomous processing of input (14, 15). Attitudes towards obesity, for example, become more favourable when participants face positive illustrations of obese individuals instead of negatively framed images (16, 17). Reflective stigmatization can be altered by prompting conscious engagement with facts (14, 15). This is supported by disease-specific education programmes (9, 10).
Due to the dual processing of content by social media users (12), such platforms may alter the stigmatization of psoriasis in either a negative or positive way. Considering intuitive and reflective stigmatization, a literature review advocated mass media interventions that follow an educational approach for changing external stigmatization (15). The platform Instagram fulfils these requirements as a social media application that is used by one-fifth of Germans on a daily basis (18) and that enables educational information to be shared via images, videos, and texts (19).
The aim of this randomized controlled trial (RCT) was to observe the effect of an Instagram-based intervention on daily Instagram users’ intuitive and reflective stigmatization of psoriasis. Included participants, aged 18–49 years, were exposed to either a psoriasis-sensitizing Instagram account or an Instagram account with beauty-glorifying content.
MATERIALS AND METHODS
Study design and participants
The study was designed as a double-blind, parallel group, 2-arm RCT and approved by the ethics committee of the Medical Faculty of the Technical University of Munich, Munich, Germany (reference 555/21 S).
The study was conducted between April 2021 and March 2022, with recruitment taking place in November and December 2021 and online data collection from November 2021 to January 2022. Assessments were performed at baseline (t0), immediately before (t1) and after the intervention (t2), and at a 2-week follow-up (= two weeks after the intervention took place; t3).
Study participants were recruited through an Instagram story and via flyers distributed online among members of the Faculty of Sport and Health Sciences of the Technical University of Munich. Both, the story, and the flyers comprised information regarding the studies procedures and a link to the baseline assessment. Before participation, all individuals gave electronic informed consent.
Study procedure
With the questionnaire at t0, eligibility criteria were checked and data on sex, highest educational degree, current employment/educational status, and skin heath status were collected. Individuals aged 18–49 years with an Instagram account and an understanding of the German language were deemed eligible. Participants were randomly assigned to either the intervention group (IG) or the control group (CG) as per a computer-generated sequence in a 1:1 ratio.
A permuted block stratification approach was chosen to ensure a balanced distribution of participants regarding selected key characteristics as well as to provide allocation concealment. Four strata based on age (18–25, 26–33, 34–41, 42–49 years), gender (female/male/non-binary), highest educational degree (secondary school, high school, university, other), and current employment/educational status (pupil, trainee, student, employee) were created, and each recruitment session was used as a block in the permuted block randomization procedure with varying block lengths.
Using the RAND function (Microsoft Excel; version: 16.7; Redmond, WA, USA: Microsoft Corp.), blockwise and in a continuous manner, 1 participant was assigned to the IG, the next one to the CG. Documentation of the randomization procedure was done via a list, encompassing all possible strata combinations and levels. Furthermore, the number of participants per group and stratum were included. Whenever differences in the number of participants per group and stratum occurred (difference >2 participants), an equal distribution was achieved by allocating the next participant with a suitable strata combination to the group with fewer participants.
Individuals were blinded to allocation, as were the staff members, except for a trustee responsible for administration of participants and not involved in the statistical analyses.
After randomization, participants in each study group received an e-mail containing a personalized, pseudonymized identifier and a questionnaire-link including a photo-rating task (t1). Upon completing both, individuals were instructed to scroll through the content of a group-specific Instagram account for 10 min that was either psoriasis-sensitizing (IG) or based on beauty-glorifying content (CG). German Instagram users spend a mean of 20–30 min per day on Instagram (20–22), generally distributed over multiple visits per day (23, 24). The duration of the intervention was therefore deemed suitable.
Subsequently, individuals were instructed to again complete the same questionnaire and photo-rating task as prior to the intervention (t2).
Two weeks after the intervention took place, participants were asked via e-mail to complete the questionnaire and photo-rating task again (t3) (Fig. 1). The follow-up period was considered appropriate since the study was designed as a pilot. Participants who completed all assessments were informed by e-mail about the study aims and the names of the Instagram accounts.
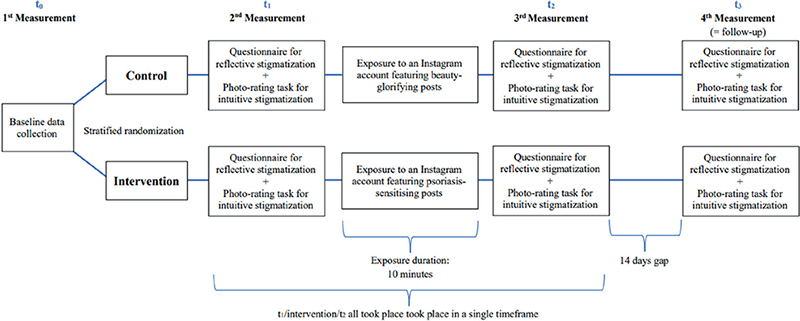
Fig. 1. Graphical representation of the study process. (t0) Baseline assessment, (t1) pre-intervention, (t2) post-intervention, and (t3) 2-weeks after the intervention took place.
Sample size calculation
An a priori power analysis with a t-test for 2 independent groups was performed using G*Power (25). Considering a significance level of α = 0.05, a minimum power of 0.80, an effect size of 0.65 (9), and a drop-out rate of 30%, a sample of 111 participants was required.
Intervention
The Instagram account for the IG was created in consultation with the “Psoriasis-Netz” (https://www.psoriasis-netz.de) and included 50 posts with pictures, texts, and videos that should sensitize participants to psoriasis by drawing attention to the skin disease, increasing knowledge, and ultimately targeting potential stigmatization, e.g. through information on the impaired HRQoL of affected individuals (Table SI). All information was based on scientific sources that were shared with participants in the captions of the respective posts. The Instagram account for the CG also contained 50 posts with pictures, texts, and videos, all of which contained beauty-glorifying content, e.g. representations of flawless skin (Table SII). The information provided was based on lifestyle magazines and internet blogs, and no sources were disclosed to participants. No instructions on how to engage with the account were given to the IG and CG, except those outlining an interaction time frame of 10 min. To check the participants’ account interaction, the 26th post prompted participants to give it a “like”. However, this served only as an indicator of the engagement with the provided Instagram content and not “liking” the post had no consequences. The comment function for both accounts was disabled, and the number of “likes” per picture was not displayed publicly.
Primary outcome measures
The primary outcome was reflective stigmatization towards people with psoriasis. According to the dual processing theory, system 2 is activated by loading the working memory, which simultaneously inhibits system 1 (14) and can be tested by self-report questionnaires (15). In accordance with this, participants were asked to actively reason on their attitudes towards people with psoriasis based on 4 categories extracted from a validated questionnaire (9).
Stereotype Endorsement. Stereotype awareness was assessed on a 5-point Likert Scale with 11 adjective pairs (e.g. “healthy” – “sick”). Participants needed to decide on a value in between both ends, representing their associations with a person affected by psoriasis. Inverted items were re-coded, and the mean of the sum of all scores was generated for each participant per group, with a lower number indicating less endorsement of negative stereotypes. Good internal consistency was observed in the present sample (Cronbach’s alpha = 0.83).
Social Distance. Social Distance was quantified with 14 items to test the attitude of participants towards people with psoriasis in different situations (e.g. shaking hands). A 5-point Likert scale was applied to measure their desire for Social Distance, ranging from “definitely not” to “definitely”. After re-coding inverted item scores, answer values were summed up for all participants of each group and the mean calculated, with smaller values suggesting a lower stigmatization. In the current sample, good internal consistency was observed (Cronbach’s alpha = 0.83).
Disease-related Misconceptions. Knowledge about 14 myths regarding psoriasis was queried. Participants were encouraged to give their assessment on a 5-point Likert scale, which evaluated their degree of agreement (“strongly agree” – “strongly disagree”) with certain statements (e.g. psoriasis is a serious disease). Inverted items were re-coded, scores were summed, and the mean was calculated for each participant per group. Smaller values indicated fewer misconceptions. Poor internal consistency was observed in the current sample (Cronbach’s alpha = 0.59).
Reported and Intended Behaviour Scale (RIBS). Evaluated with 4 items with each connected to a 5-point Likert Scale, RIBS queried the participants’ degree of agreement (“totally agree” – “totally disagree”) regarding potential future behaviours (e.g. living together with a person with a skin disease). Participants could also select the option “I do not know”. Except for those individuals who chose the answer “I do not know,” scores were summed for participants of each group and the mean calculated. Lower values indicated less stigmatizing behaviour. In the current sample, questionable internal consistency was observed (Cronbach’s alpha = 0.61).
Secondary outcome measures
The secondary outcome was defined as the intuitive stigmatization of people with psoriasis. The dual processing theory states that system 1 is triggered by decisions made under time pressure while simultaneously suppressing system 2 (14) and can be assessed by response time measures (15). Accordingly, an explorative photo-rating task was created. Ten computer-generated photographs of faces of non-existing persons were displayed to participants, generated by the website www.thispersondoesnotexist.com (26). Each person was featured both in their artificial-intelligence-generated psoriasis-free skin condition and with psoriasis added to the facial area by image processing (Fig. 2). All pictures were shown for only 10 s with the possibility to review them once again. This approach was chosen based on a study that similarly observed participants’ intuitive and reflective stigmatization when shown pictures of people with different stigmatized conditions (e.g. paralysis). Results did not yield a clear cut-off concerning how long a reaction remains intuitive and when reflective processing starts. The authors argued that, at all times, both types of processing are present to varying extents, with intuitive processing becoming less prominent and reflective processing becoming more prominent over time (27). In contrast to that research, participants in the current study were not specifically informed of what condition the individuals being rated had, and were not directed to reflect on their rating towards the end of the 10-s period. Both aspects can be assumed to trigger a premature onset of reflective stigmatization. Since the dual processing of stigmatization towards skin diseases has never been examined, the full 10 s were employed. This length of time should further address potential complications related to the photo-rating task not being carried out under a controlled laboratory setting, which was also the reason for giving the opportunity to review each photograph once.

Fig. 2. Example of a displayed non-existent face without (left) and with (right) added psoriasis lesion.
During the photo-rating task, individuals were instructed to note whether they would trust the shown person (yes/no) and how trustworthy they perceived them to be, measured on a visual analogue scale (VAS) that ranged from 0 (not trustworthy) to 100 (very trustworthy). Trust was chosen as stigmatization indicator, since the absence of skin smoothness was associated with reduced trustworthiness in previous studies (28, 29).
In the subsequent statistical analysis, only VAS values were considered, due to the more accurate information regarding trust that they provided. An individual’s score was examined with 3 steps: by calculating the difference between the images of the same person displayed with and without psoriasis, summing these differences, and then calculating the overall mean. Smaller scores indicated a lower difference between an image pair, and therefore less stigmatization.
Statistical analysis
To ensure plausibility, participants were checked for unlikely combinations of personal characteristics at t0. Furthermore, extreme outliers, more than 3 interquartile ranges below the 1st quartile or above the 3rd quartile, at t1, t2, and t3 of the questionnaire subcategories and of the ratings in the photo-rating task were not considered for separate analyses of the related components. This led to variations in the number of participants analysed per questionnaire subcategory and for the photo-rating task. Missing data were not processed, since both the questionnaire and the photograph-rating task were constructed to not allow for missing values. Descriptive statistics were provided for age, sex, highest educational level, current employment/educational status, and skin disease affectedness. The group means and standard deviations (SDs) at t1, t2, and t3 for each questionnaire subcategory and for the photo-rating task were reported.
Due to violations of normal distribution in Social Distance, Disease-related Misconceptions, Reported and Intended Behaviour, and for the photo-rating task, inter-group differences in stigmatization at the 3 measured time-points were analysed with Mann–Whitney U tests. For Stereotype Endorsement, homogeneity of covariance matrices was not met. Thus, unpaired t-tests were used. To account for multiple testing, Bonferroni correction was applied by multiplying a test specific significance value with the number of related tests performed. Intra-group changes over time were assessed using Friedmann tests and an analysis of variance (ANOVA), supplemented respectively by Bonferroni corrected Wilcoxon signed-rank tests and t-tests for post hoc analysis.
Furthermore, it was investigated via binary logistic regressions whether the potential covariables age, sex, highest educational level, current employment/educational status, and skin disease affectedness had an influence, in case of significant intra-group changes in stigmatization over time (yes/no).
A significance level of α = 0.05 was applied. Statistical analysis was performed using IBM SPSS Statistics 27.0 (version 1.0.0.1461) (Armonk, NY, USA: IBM Corp.).
RESULTS
Sample characteristics
A total of 123 individuals responded to the baseline questionnaire at t0, of whom 105 met the inclusion criteria and were enrolled in the study. Of these, 54 participants adhered fully to the study procedure at t1, t2, and t3 and were included in the statistical analysis, with 26 individuals assigned to the IG and 28 to the CG (Fig. 3).
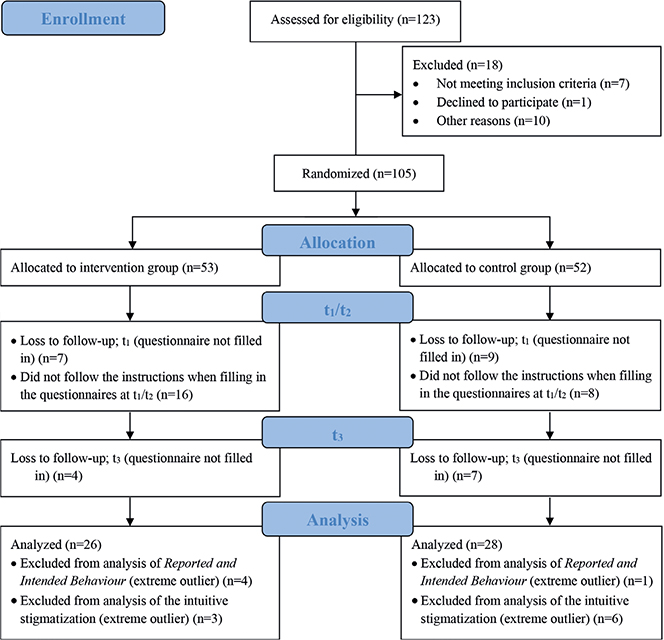
Fig. 3. Participants’ flow chart. (t1) Pre-intervention, (t2) post-intervention, and (t3) 2-weeks after the intervention took place.
The mean age of individuals included in the statistical analyses was 24.78 (SD 4.95) years and more than 70% were women (n = 38). Almost all participants reported either having a high school degree (n = 23) or a university degree (n = 26). A total of 29 participants were students, while 21 individuals were employees. Four people reported being affected by a skin disease, with 2 reporting having acne and another 2 atopic dermatitis (Table I).
| Total (n = 54) | Intervention group (n = 26) | Control group (n = 28) | |
| Age, mean (SD) | 24.78 (4.95) | 25.12 (6.49) | 24.46 (2.98) |
| Gender, n | |||
| Female | 38 | 18 | 20 |
| Male | 16 | 8 | 8 |
| Highest educational degree, n | |||
| Secondary school | 4 | 1 | 3 |
| High school degree | 23 | 12 | 11 |
| University degree | 26 | 13 | 13 |
| Other educational degree | 1 | − | 1 |
| Current employment/educational status, n | |||
| Pupil | 1 | 1 | − |
| Trainee | 3 | 3 | − |
| Student | 29 | 15 | 14 |
| Employee | 21 | 7 | 14 |
| Affected by skin diseasea, n | |||
| Yes | 4 | 1 | 3 |
| No | 50 | 25 | 25 |
| Type of skin diseaseb, n | |||
| Acne | 2 | _ | 2 |
| Atopic dermatitis | 2 | 1 | 1 |
| aSubjects reported if they were personally affected by a skin disease. bFour subjects reported their type of skin disease. | |||
| SD: standard deviation. | |||
A total of 17 participants in the IG and 14 in the CG “liked” the Instagram post as instructed.
Primary outcome: reflective stigmatization towards individuals with psoriasis
Stereotype Endorsement. No significant inter-group stereotyping differences at the 3 measured time-points were identified (t1: t(52) = 1.32, p = 0.582, 95% CI [–0.11, 0.53]; t2:t(52) = –0.27, p = 1.00, 95% CI [–0.42, 0.32]; t3: t(52) = –1.05, p = 0.898, 95% CI [–0.48, 0.15]). How-ever, significant changes were found for the IG with a strong effect size (F(2, 50) = 13.40, p < 0.001, partial η² = 0.35, f = 0.73, n = 26). Post-hoc analysis presented a significant decrease in Stereotype Endorsement, t1–t2 (MDiff = 0.44, p = 0.002, 95% (CI) [0.16; 0.72]) and t1–t3 (MDiff = 0.55, p < 0.001, 95% CI [0.25, 0.84]) but not for t2–t3 (MDiff = 0.11, p = 1.00, 95% CI [–0.18, 0.39]). Binary regression denoted no significant influence of covariables on stereotyping reduction for either t1–t2 (χ2(5) = 4.54, p = 0.474) or t1–t3 (χ2(5) = 4.16, p = 0.527). Regarding the CG, no significant change was achieved over the study period (F(2, 54) = 2.82, p = 0.068, partial η² = 0.10, n = 28).
Social Distance. No inter-group differences were significant (t1: U = 354.00, Z = –0.17, p = 1.00; t2:U = 238.00, Z = –2.20, p = 0.084; t3: U = 317.00, Z = –0.82, p = 1.00). Furthermore, participants of both groups, IG and CG, did not significantly lower their desire for Social Distance over time (χ2(2) = 5.48, p = 0.065, n = 26; χ2(2) = 5.59, p = 0.061, n = 28, respectively).
Disease-related Misconceptions. A significantly lower agreement with misconceptions for the IG in comparison with the CG occurred with a strong effect size at t2 (U = 145.50, Z = –3.79, p < 0.001, d = 0.52) and a medium effect size at t3 (U = 177.00, Z = –3.25, p = 0.003, d = 0.44). At t1, no significant inter-group difference was detected(U = 344.00, Z = –0.35, p = 1.00). In addition, significant changes throughout the study period were observed for the IG (χ2(2) = 12.64, p = 0.002, n = 26). Post-hoc analysis revealed significantly lower values of misconceptions with a small effect size for t1–t2 (Z = 0.71, p = 0.031; d = 0.14) and for t1–t3 (Z = 0.90, p = 0.003; d = 0.18), while t2–t3 was not significant (Z = 0.19, p = 1.00). Binary regression models did not imply a significant influence of any covariable on t1–t2 (χ2(5) = 4.27, p = 0.511) nor on t1–t3 (χ2(5) = 2.70, p = 0.746). For the CG, results indicat-ed no significant change between the study time-points (χ2(2) = 4.83, p = 0.089, n = 28).
Reported and Intended Behaviour. At no study time-point was a significant difference between IG and CG in stigmatizing behaviour demonstrated (t1: U = 237.50, Z = –1.44, p = 0.452; t2:U = 221.50, Z = –1.86, p = 0.187; t3: U = 281.00, Z = –0.41, p = 1.00). Moreover, there was no significant change over time for the IG (χ2(2) = 1.00, p = 0.607, n = 22) or for the CG (χ2(2) = 3.23, p = 0.198, n = 27).
Secondary outcome: intuitive stigmatization towards individuals with psoriasis
For the 3 study time-points, no significant differences were observed between the 2 study groups (t1: U = 252.00, Z = –0.02, p = 1.00; t2:U = 189.00, Z = –1.45, p = 0.438; t3: U = 177.50, Z = –1.72, p = 0.259). Furthermore, the intuitive stigmatization of participants in the IG and CG did not reveal a significant change across the study period (χ2(2) = 2.54, p = 0.282, n = 23; χ2(2) = 5.37, p = 0.068, n = 22, respectively).
All presented intra-group changes, measured time-points, and underlying mean and SD values are shown in Table II.
| Intervention Mean (SD) | Time range | Statistical difference | Control Mean (SD) | Time range | Statistical difference | |
| Stereotype endorsement IG: n = 26 | CG: n = 28 |
||||||
| t1 | 2.20 (0.65) | t2–t1 | t(25) = 3.99; p = 0.002a | 1.99 (0.52) | t2–t1 | t(27) = 2.24; p = 1.00a |
| t2 | 1.77 (0.57) | t3–t1 | t(25) = 4.77; p < 0.001a | 1.81 (0.75) | t3–t1 | t(27) = 2.06; p = 1.00a |
| t3 | 1.66 (0.52) | t3–t2 | t(25) = 0.98; p = 1.00a | 1.82 (0.62) | t3–t2 | t(27) = –0.07, p = 1.00a |
| Social distance IG: n = 26 | CG: n = 28 |
||||||
| t1 | 0.54 (0.51) | t2–t1 | z = –2.62; p = 0.027b | 0.50 (0.39) | t2–t1 | z = –0.05; p = 1.00b |
| t2 | 0.34 (0.40) | t3–t1 | z = –1.81; p = 0.210b | 0.54 (0.41) | t3–t1 | z = –2.26; p = 0.072b |
| t3 | 0.40 (0.49) | t3–t2 | z = –0.62; p = 1.00b | 0.39 (0.38) | t3–t2 | z = –2.48; p = 0.040b |
| Disease-related misconceptions IG: n = 26 | CG: n = 28 |
||||||
| t1 | 1.01 (0.39) | t2–t1 | z = 0.71; p = 0.031b | 1.06 (0.44) | t2–t1 | z = –2.09; p = 0.110b |
| t2 | 0.79 (0.30) | t3–t1 | z = 0.90; p = 0.003b | 1.22 (0.43) | t3–t1 | z = –0.05; p = 1.00b |
| t3 | 0.71 (0.24) | t3–t2 | z = 0.19; p = 1.00b | 1.04 (0.42) | t3–t2 | z = –2.10; p = 0.106b |
| Stigmatizing behaviour IG: n = 22 | CG: n = 27 |
||||||
| t1 | 0.11 (0.24) | t2–t1 | z = –1.30; p = 0.581b | 0.27 (0.40) | t2–t1 | z = –0.63; p = 1.00b |
| t2 | 0.07 (0.18) | t3–t1 | z = –0.82; p = 1.00b | 0.23 (0.35) | t3–t1 | z = –2.04; p = 0.124b |
| t3 | 0.09 (0.16) | t3–t2 | z = –0.71; p = 1.00b | 0.15 (0.27) | t3–t2 | z = –1.81; p = 0.210b |
| Photo-rating task IG: n = 26 | CG: n = 28 |
||||||
| t1 | 7.01 (43.62) | t2–t1 | z = –0.89; p = 1.00b | –0.86 (79.71) | t2–t1 | z = –1.34; p = 0.543b |
| t2 | –0.10 (32.44) | t3–t1 | z = –0.29; p = 1.00b | 24.37 (56.02) | t3–t1 | z = –0.75; p = 1.00b |
| t3 | 11.16 (25.76) | t3–t2 | z = –1.62; p = 0.318b | –8.35 (48.55) | t3–t2 | z = –2.26; p = 0.072b |
| at-test corrected for multiple testing (n = 3) according to Bonferroni. bWilcoxon test corrected for multiple testing (n = 3) according to Bonferroni. | ||||||
| t0:baseline assessment; t1: pre-intervention; t2: post-intervention; t3: 2-weeks after the intervention took place ; IG: intervention group; CG: control group; SD: standard deviation; in bold: p - value <0.05. | ||||||
DISCUSSION
The aim of this study was to investigate the effect of an Instagram-based intervention on users stigmatization of people with psoriasis, depending on the social media content to which they were exposed. Regarding reflective stigmatization between IG and CG, there were significant inter-group differences only in Disease-related Misconceptions post-intervention and at follow-up. When comparing the different time-points in the IG, a significant decrease in Stereotype Endorsement could be observed between pre- and post-intervention as well as between pre-intervention and follow-up. The agreement with Disease-related Misconceptions decreased significantly between the study time points. No significant changes were shown in other subcategories of the IG or at any time in the CG. Concerning intuitive stigmatization, no significant changes between or within IG and CG were identified over the course of the study.
Referring to the dual processing theory, system 2 can be addressed through conscious engagement with information (14), and connected stigmatizing thought processes can be altered via educational strategies (15). Since the IG Instagram account presented informative, evidence-based content about psoriasis, a reduction in Stereotype Endorsement and Disease-related Misconceptions over time was to be expected, as both subcategories reflect knowledge of the disease. This, together with the CG not having received any psoriasis-specific facts, also serves as a rationale for the lower values in Disease-related Misconceptions of the IG compared with the CG found at post-intervention and follow-up.
The findings of the current study are mostly in line with 2 studies that aimed to reduce external stigmatization of visible chronic skin diseases, but through in-person approaches (9, 10). Furthermore, at least 1 of the 2 studies reported an inter-group difference for each subcategory for a certain study time-point. An agreement was given regarding less Stereotype Endorsement in the IG post-intervention and at the follow-up compared with the CG (9, 10). Furthermore, both studies found evidence for a reduction in the desire for Social Distance and less stigmatized Reported and Intended Behaviour between the measurement time-points in the IG.
The greater impact of both studies may be due to the longer duration of their interventions (1.5–3 h). Another reason may be the more extensive design of their interventions, e.g. by initiating direct contact between participants and persons affected by psoriasis (9, 10). Interpersonal contact is considered effective in targeting stigma-related system 2 (15) and shown to be even more successful in reducing negative attitudes and stigmatization than focusing exclusively on knowledge and the sole application of an educational approach (30).
Since Instagram is a mass media platform and both the IG and CG accounts presented emotional and entertaining content in the form of images, a change in intuitive stigmatization would have been anticipated through the activation and modification of system 1 (12, 15). However, no changes in intuitive stigmatization were observed. This could be due to the missing validation of the photo-rating task or the fact that intuition changes only slowly (31); thus, the 10-min intervention in the current study might have been too short. Except for 1 study that collected data after, but not before, displaying images of persons affected by psoriasis to study participants (32), a lack of studies on intuitive stigmatization of psoriasis inhibits comparison of the study results with previous research. A possible argument for the absence of a negative influence of the CG Instagram account on both types of stigmatization is that the Instagram account focused on people fitting modern beauty standards. The findings of 2 studies on obesity indicated higher stigmatization of obesity in participants when shown pictures illustrating obese people in unflattering scenarios compared with in favourable scenarios (16, 17). Therefore, had the CG account depicted people with psoriasis in a negative light, a different outcome on stigmatization may have been observed.
The lack of effect of the photo-rating task could also be due to the fact that the 10-s period and the additional single repetition were too long to trigger solely intuitive stigmatization. The participants might have already been primed by the previous questionnaire, assuming that the task must somehow be about psoriasis, and consequently answered more reflectively. With respect to the dual processing theory, the wordings “intuitive” and “reflective” to represent system 1 and system 2 processing can be questioned. Indeed, a major criticism of the theory is its lack of unified labelling of the 2 systems (14). In another study on dual psychological processes underlying stigmatization, the authors referred to system 1 as “associative” and system 2 as “rule-based processing” (15). Such ambiguities lead to confusion and limit the modes of action of the 2 systems. At the same time, a clear and evidence-based theoretical foundation is evolving for the differentiation between systems 1 and 2 to explain processes of judgement, decision-making, and stigmatization (14, 15), which makes it desirable to prefer the general designation of these processes as system 1 and system 2. Furthermore, the 2 systems should not be considered as working completely independently of each other (14), underlining the necessity of both systems for successful stigma reduction strategies (15).
Strengths and limitations
The theoretical foundation of stigmatization on the dual processing theory and the standardized and validated questionnaire used to assess reflective stigmatization (9) can be seen as strengths of this study. The double-blinded, stratified randomized controlled design accounted for confounding, selection bias, and researcher influence. Compared with other studies (9, 10), which included specific target groups (e.g. medical students), this study addressed a more heterogeneous study sample by focusing on daily Instagram users, aged 18 to 49 years, at large. Nevertheless, as study participation was voluntary and participants were recruited through online flyers and stories on Instagram, selection bias should be considered, which may have resulted in a misleading estimation of the effect. In addition, the sample consisted of individuals with an overall higher educational level than the average Instagram user (33). Participants were relatively young, and the male:female ratio was approximately 1:2. External validity is therefore minimized. Moreover, participant responses may have been adapted to socially desirable norms and values (34). With a duration of 10 min and a non-restricted setting, the application and accessibility of the intervention were favourable compared with those of another study that reported difficulties with the implementation of a 3-h in-person intervention (9).
The uncontrolled setting in which the intervention took place can be considered a limitation. The only given indicator concerning engagement with the provided Instagram content (to “like” the 26th post) suggests a low interaction in both IG and CG. suggested, engagement behaviour in a study is perceived as a too complex a construct to evaluate with only 1 marker (35).
As values for Cronbach’s alpha were shown to be poor to questionable in 2 subcategories, internal consistency is minimized. It should be noted that 1 item was missing in the questionnaire component Disease-related Misconceptions with 14 items, which could have led to a tampered estimation of the effect on the related subcategory. Lastly, the explorative photo-rating task used in this pilot study is a newly developed, and not yet validated, tool, making it unclear whether intuitive stigmatization is actually being addressed regarding the 10-s duration and additional single repetition per photograph.
This pilot study supports further, more in-depth, study of the effectiveness of social media on the stigmatization of psoriasis and the usage of image-based technologies for dermatological purposes. Future research should focus on an appropriate sample size with balanced participant characteristics. In addition, an extension of the follow-up period would be useful to investigate longer-lasting effects of such an intervention. As the current study showed low engagement with the Instagram accounts, a study in a controlled setting should be conducted. Furthermore, validation and standardization of the photo-rating task should be performed. Attention should be given to additional research on the dual processing theory, with special focus on system 1- and system 2-related stigmatization.
Conclusion
An Instagram account with psoriasis-sensitizing content can be effective in reducing daily Instagram users’ stigmatization of people with psoriasis. The promising results of the current study support future research into the use of Instagram and other social media platforms as an intervention tool to reduce stigmatization of people affected by psoriasis or other visible skin diseases. This intervention could contribute towards the WHO global goal of decreasing stigmatization of psoriasis while simultaneously increasing support for the HRQoL of people with psoriasis.
ACKNOWLEDGEMENTS
The authors would like to thank Claudia Liebram, representing the “Psoriasis-Netz” (https://www.psoriasis-netz.de), for her support with and the provision of materials for the Instagram account. We would also like to thank the ECHT study project team, and, in particular, Dr Rachel Sommer, for their valuable contributions to designing this intervention and for supplying essential research resources.
REFERENCES
- Parisi R, Iskandar IYK, Kontopantelis E, Augustin M, Griffiths CEM, Ashcroft DM. National, regional, and worldwide epidemiology of psoriasis: systematic analysis and modelling study. BMJ 2020; 369: m1590.
- Dalgard FJ, Gieler U, Tomas-Aragones L, Lien L, Poot F, Jemec GBE, et al. The psychological burden of skin diseases: a cross-sectional multicenter study among dermatological out-patients in 13 European countries. J Invest Dermatol 2015; 135: 984–991.
- World Health Organization (WHO). Global report on psoriasis. [accessed 2021 Apr 05]. Available from: https://apps.who.int/iris/bitstream/handle/10665/204417/9789241565189_eng.pdf.psoriasis?sequence=1.
- Jankowiak B, Kowalewska B, Krajewska-Kułak E, Khvorik DF. Stigmatization and quality of life in patients with psoriasis. Dermatol Ther (Heidelb) 2020; 10: 285–296.
- Sommer R, Augustin M, Mrowietz U, Topp J, Schäfer I, von Spreckelsen R. Stigmatisierungserleben bei Psoriasis – qualitative Analyse aus Sicht von Betroffenen, Angehörigen und Versorgern. Hautarzt 2019; 70: 520–526.
- Sommer R, Topp J, Mrowietz U, Zander N, Augustin M. Perception and determinants of stigmatization of people with psoriasis in the German population. J Eur Acad Dermatol Venereol 2020; 34: 2846–2855.
- World Health Assembly. Sixty-Seventh World Health Assembly: Psoriasis. 2014. [accessed 2021 Jan 21]. Available from: https://apps.who.int/gb/ebwha/pdf_files/WHA67/A67_R9-en.pdf.
- Augustin M, Mrowietz U, Luck-Sikorski C, von Kiedrowski R, Schlette S, Radtke MA, et al. Translating the WHA resolution in a member state: towards a German programme on ‘Destigmatization’ for individuals with visible chronic skin diseases. J Eur Acad Dermatol Venereol 2019; 33: 2202–2208.
- Sommer R, Weinberger NA, Von Spreckelsen R, Mrowietz U, Schielein MC, Luck-Sikorski C, et al. A structured intervention for medical students significantly improves awareness for stigmatisation in visible chronic skin diseases: a randomised controlled trial. Acta Derm Venereol 2021; 102: adv00641.
- Weinberger NA, Mrowietz S, Luck-Sikorski C, von Spreckelsen R, John SM, Sommer R, et al. Effectiveness of a structured short intervention against stigmatisation in chronic visible skin diseases: results of a controlled trial in future educators. Health Expect 2021; 24: 1790–1800.
- Shahbaznezhad H, Dolan R, Rashidirad M. The role of social media content format and platform in users’ engagement behavior. J Interact Market 2021; 53: 47–65.
- Dolan R, Conduit J, Bentham C, Fahy J, Goodman S. Social media engagement behavior: a framework for engaging customers through social media content. Eur J Market 2019; 53: 2213–2243.
- Evans JS. In two minds: dual-process accounts of reasoning. Trends Cogn Sci 2003; 7: 454–459.
- Evans JS, Stanovich KE. Dual-process theories of higher cognition: advancing the debate. Perspect Psychol Sci 2013; 8: 223–241.
- Reeder GD, Pryor JB. Dual psychological processes underlying public stigma and the implications for reducing stigma. Mens Sana Monogr 2008; 6: 175–186.
- McClure KJ, Puhl RM, Heuer CA. Obesity in the news: do photographic images of obese persons influence antifat attitudes? J Health Commun 2011; 16: 359–371.
- Puhl RM, Luedicke J, Heuer CA. The stigmatizing effect of visual media portrayals of obese persons on public attitudes: does race or gender matter? J Health Commun 2013; 18: 805–826.
- Beisch N, Koch W. 25 Jahre ARD/ZDF-Onlinestudie: Unterwegsnutzung steigt wieder und Streaming/Mediatheken sind weiterhin Treiber des medialen Internets. [accessed 2022 Mar 06]. Available from: https://www.ard-media.de/fileadmin/user_upload/media-perspektiven/ARD-ZDF-Onlinestudie/25_Jahre_ARD-ZDF-Onlinestudie.pdf.
- Fung IC, Blankenship EB, Ahweyevu JO, Cooper LK, Duke CH, Carswell SL, et al. Public health implications of image-based social media: a systematic review of Instagram, Pinterest, Tumblr, and Flickr. Perm J 2020; 24: 18.307.
- Die Medienanstalten. Average time spent using social networks per person in Germany in December 2017, by platform. [accessed 2022 Mar 06]. Available from: https://www.die-medienanstalten.de/fileadmin/user_upload/die_medienanstalten/Themen/Forschung/Internetnutzung/Nielsen_Jahresbericht_2017.pdf.
- Instagram. Celebrating one year of Instagram stories. [accessed 2022 Mar 06]. Available from: https://about.instagram.com/blog/announcements/celebrating-one-year-of-instagram-stories.
- Murmuras. Tägliche Nutzungsdauer der WhatsApp-, Instagram-, und YouTube-App durch Nutzer in Deutschland von Januar bis Juli 2020. [accessed 2022 Mar 06]. Available from: https://de.statista.com/statistik/daten/studie/1175958/umfrage/taegliche-nutzungsdauer-von-apps/#professional.
- Yellow. Umfrage zur Nutzungsdauer pro Besuch von sozialen Netzwerken in Australien 2016. [accessed 2022 Mar 06]. Available from: https://irp-cdn.multiscreensite.com/535ef142/files/uploaded/Sensis_Social_Media_Report_2016.pdf.
- Facebook IQ. How to connect with new audiences on Instagram. [accessed 2022 Mar 06]. Available from: https://en-gb.facebook.com/business/news/insights/how-to-connect-with-new-audiences-on-instagram.
- Faul F, Erdfelder E, Lang A-G, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods 2007; 39: 175–191.
- Karras T, Laine S, Aila T. A style-based generator architecture for generative adversarial networks. IEEE Trans Pattern Anal Mach Intell 2021; 43: 4217–4228.
- Pryor JB, Reeder GD, Yeadon C, Hesson-McLnnis M. A dual-process model of reactions to perceived stigma. J Pers Soc Psychol 2004; 87: 436–452.
- Jaeger B, Wagemans FMA, Evans AM, van Beest I. Effects of facial skin smoothness and blemishes on trait impressions. Perception 2018; 47: 608–625.
- Tsankova E, Kappas A. Facial skin smoothness as an indicator of perceived trustworthiness and related traits. Perception 2016; 45: 400–408.
- Corrigan PW, Morris SB, Michaels PJ, Rafacz JD, Rüsch N. Challenging the public stigma of mental illness: a meta-analysis of outcome studies. Psychiatr Serv 2012; 63: 963–973.
- Lieberman MD, Jarcho JM, Satpute AB. Evidence-based and intuition-based self-knowledge: an FMRI study. J Pers Soc Psychol 2004; 87: 421–435.
- Pearl RL, Wan MT, Takeshita J, Gelfand JM. Stigmatizing attitudes toward persons with psoriasis among laypersons and medical students. J Am Acad Dermatol 2019; 80: 1556–1563.
- Faktenkontor. Anteil der befragten Internetnutzer, die Instagram nutzen, nach Bildungsgrad in Deutschland im Jahr 2017. [accessed 2022 Jan 02]. Available from: https://www.faktenkontor.de/studien/social-media-atlas-2017-2018/
- Jonkisz E, Moosbrugger H, Brandt H. Planung und Entwicklung von Tests und Fragebogen. In: Moosbrugger H, Kelava A, editors. Testtheorie und Fragebogenkonstruktion. Berlin, Heidelberg: Springer Berlin Heidelberg; 2012. p. 27–74.
- Short C-E, DeSmet A, Woods C, Williams S-L, Maher C, Middelweerd A, et al. Measuring engagement in ehealth and mhealth behavior change interventions: viewpoint of methodologies. J Med Internet Res 2018; 20: e292.