ORIGINAL REPORT
Tolerability of Narrow-band Ultraviolet-B Phototherapy for Different Dermatological Diseases in Relation to Co-medications
Anna M. HALUPCZOK, Ann-Sophie BOHNE, Sascha GERDES, Stephan WEIDINGER and Michael WEICHENTHAL
Department of Dermatology, University Hospital of Schleswig-Holstein, Kiel, Germany
Phototherapy is an efficient therapy for a variety of skin diseases. Various drugs can cause photosensitivity and impact tolerability of phototherapy. The tolerability was investigated of narrowband ultraviolet-B 311 nm therapy in dependence on the underlying disease and long-term co-medication. A total of 534 narrowband ultraviolet-B therapy courses were examined. Compared with psoriasis, adverse events were observed more frequently in eczematous diseases and, in some cases, other indications. About two-thirds of all courses were carried out in patients taking at least one photosensitising drug, according to the summaries of product characteristics. Phototherapy was more frequently associated with adverse events when medication was taken concomitantly. When considering the tolerability of phototherapy in dependence on individual substances or drug classes, no statistically significant result was shown after adjustment.
Key words: medication; photosensitivity; phototherapy; UV therapy.
SIGNIFICANCE
Phototherapy is an efficient therapy for a variety of skin diseases. In addition to the therapeutic benefit of sunlight, the light-sensitising effect of many active substances is also known. The tolerability of NB-UVB therapy was investigated in dependence on underlying dermatological disease and existing long-term medication. Overall, phototherapy is considered a safe, well-tolerated therapy option with few side effects. When taking potentially light-sensitising drugs, the practitioner should still aim for careful dose finding to be able to guarantee safe therapy even in the presence of light-sensitising medication.
Citation: Acta Derm Venereol 2024; 104: adv35215. DOI https://doi.org/10.2340/actadv.v104.35215.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Submitted: Dec 19, 2023; Accepted: Feb 27, 2024; Published: Apr 3, 2024
Corr: Anna M. Halupczok, Department of Dermatology, University Hospital of Schleswig-Holstein, Kiel, Germany. E-mail: anna.halupczok@web.de
Competing interests and funding: The authors have no conflicts of interest to declare
INTRODUCTION
Phototherapy has been used for more than 125 years to treat a variety of skin diseases (1, 2). Already in ancient times sunlight was applied for the treatment of skin diseases such as vitiligo (3). In modern phototherapy, non-ionizing radiation from the UV spectrum is used (4). The most widely used types of phototherapy are broad spectrum UVB, narrow-band UVB therapy, in which UV-B radiation of wavelength 311 nm is used (NB-UVB), and PUVA therapy, which combines the use of psoralens as photo sensitisers and UV-A radiation. NB-UVB is effective and safe with few side effects and is used for a large number of indications (5–9). The simultaneous intake of medication can potentially lead to a drug-induced increase in photosensitivity. A large number of medications are reported to have photosensitising potential (10–12). The aim of this study was to investigate the tolerability of NB-UVB phototherapy in relation to the underlying dermatological disease and concomitant medications.
MATERIALS AND METHODS
Study design, patient population, and data collection
Archived NB-UVB phototherapy plans as well as the corresponding patient files and discharge letters of outpatients and patients of the day care unit as well as inpatients of the Department of Dermatology at Kiel University were reviewed retrospectively. Demographic characteristics and the indication for UV therapy were documented for each patient. The latter was classified as psoriasis, atopic dermatitis, other types of eczema, mycosis fungoides, parapsoriasis, lichen planus, vitiligo, and “other”. Number of phototherapy sessions, start and end of phototherapy, start and end dose, cumulative radiation dose, and the reason for discontinuation of therapy were recorded. Only patients who carried out at least 6 sessions of NB-UVB and achieved a maintenance dose or those who developed treatment intolerance at any time point qualified for the evaluation. Achievement of maintenance dose was defined as a minimum of 6 sessions, of which at least the last 3 consecutive sessions were performed without dose increase or having achieved a dose of at least 1.0 J/cm2. The medications taken were classified and grouped by ATC code. The following 15 categories are distinguished: cardiovascular drugs, anticoagulants, lipid-lowering drugs, antidiabetics, diuretics, antibiotics, antiepileptic drugs, analgesics, psychopharmaceuticals, hormone preparations, supplementaria, antacids, uric acid reducers, antianaemics, and antihistamines. The summaries of product characteristics (SMPC) were used to classify the photosensitising potential of drugs as “not known”, “very rarely”, “rarely”, “occasionally”, “frequently”, and “very frequently”.
For patients who had an intolerance reaction during phototherapy, further criteria were recorded, e.g. the severity of the erythema was graded in the 3 categories mild, moderate, and severe. As part of the documentation of the radiation data, every erythema or adverse reaction that occurred was initially recorded, and not only those that resulted in relevant adverse events or could be directly assessed as such.
For the classification of adverse events, the following criteria were applied independently of each other: a documented early discontinuation of phototherapy due to increased photosensitivity; a documented severe erythema reaction or more than 2 intolerance reactions during the incremental or maintenance phase, respectively; the non-achievement of an expected therapeutic target dose, whereby the following target doses were defined for the patient collective: if the maximum tolerated dose at an initial dose of 0.1 J/cm2, which is selected for skin type I, as well as at an initial dose of 0.2 J/cm2, which is selected for skin type II, was less than 0.4 J/cm2, and if there was also an intolerance reaction, these therapies were classified as adverse events. In this case, no separate determination of the expected therapeutic target dose was made due to insufficient discriminatory power of the two skin type groups in clinical practice. If the maximum tolerated dose at an initial dose of 0.3 J/cm2, which was selected for skin type III, was below 0.7 J/cm2, this was also rated as an adverse event if an intolerance reaction also occurs.
Statistical analysis
The statistical calculations were carried out with the software package R (v 4.0.3; R Foundation for Statistical Computing, Vienna, Austria). Categorised characteristics were presented in descriptive statistics using absolute numbers, percentages, and 95% confidence intervals (95% CI), if appropriate. For continuous variables, arithmetic mean with standard deviations or median values together with 95% CI were used, depending on their distribution. Comparison tests were carried out using χ2 or Fisher’s exact tests, as appropriate. For the exploratory part of this study, no adjustments were made for multiple testing, for individual drugs with significant associations additional Bonferroni–Holmes adjusted p-values were calculated. For all tests the level of significance was set at p ≤ 0.05.
RESULTS
Data on a total of 534 NB-UVB phototherapies, including 303 male and 231 female patients, were analysed. In 89 of these, adverse events ascribed to the UVB exposure were reported, mostly erythematous reactions. Females were slightly more often affected by adverse events than males (20.3% vs 13.9%; p = 0.05) (Table I). Most indications were associated with a higher rate of AEs as compared with psoriasis (Table II); in particular, AEs were more frequent in eczema (22.6%) and atopic dermatitis (21.7%) compared with psoriasis (11.8%, p = 0.01 and p < 0.1, respectively). For eczema, the target dose was not reached in 17.5% of therapies. A particularly high treatment discontinuation rate of 18.2% was found in patients with lichen planus. Severe erythema was reported significantly more often in atopic dermatitis than in psoriasis (8.7% vs 1.2%, p < 0.01).
| Factor | Psoriasis n (%) | Atopic dermatitis n (%) | Eczema n (%) | Lichen planus n (%) | Mycosis fungoides n (%) | Para-psoriasis n (%) | Prurigo n (%) | Vitiligo n (%) | Other n (%) | Total n (%) |
| 245 (45.9) | 46 (8.6) | 137 (25.7) | 11 (2.1) | 17 (3.2) | 13 (2.4) | 37 (6.9) | 3 (0.6) | 25 (4.7) | 534 (100) | |
| Adverse events | 29 (11.8) | 10 (21.7)* | 31 (22.6)*** | 2 (18.2) | 4 (23.5) | 1 (7.7) | 6 (16.2) | 1 (33.3) | 5 (20.0) | 89 (16.7) |
| Low target dose | 15 (6.1) | 1 (2.2) | 24 (17.5)*** | 1 (9.1) | 2 (11.8) | 0 (0) | 3 (8.1) | 0 (0) | 2 (8.0) | 48 (9.0) |
| Discontinuation | 4 (1.6) | 1 (2.2) | 8 (5.8)** | 2 (18.2)** | 0 (0) | 0 (0) | 2 (5.4) | 0 (0) | 0 (0) | 17 (3.2) |
| > 2 AE in incremental phase | 10 (4.1) | 5 (10.9)* | 3 (2.2) | 0 (0) | 1 (5.9) | 0 (0) | 0 (0) | 1 (33.3) | 3 (12.0) | 23 (4.3) |
| Severe reaction | 3 (1.2) | 4 (8.7)** | 5 (3.7) | 0 (0) | 1 (5.9) | 1 (7.7) | 2 (5.4) | 0 (0) | 1 (4.0) | 17 (3.2) |
| *p < 0.1; **p < 0.05; ***p < 0.01 (Fisher’s exact test). | ||||||||||
Only 59 of the patients did not use any co-medication during phototherapy, whereas 475 therapies were accompanied by at least one drug. Adverse events were reported in 17.3% of therapies using co-medication and in 11.9% of therapies without co-medication (difference not significant). The number of co-medications was not associated with a higher frequency of adverse events (Fig. 1).
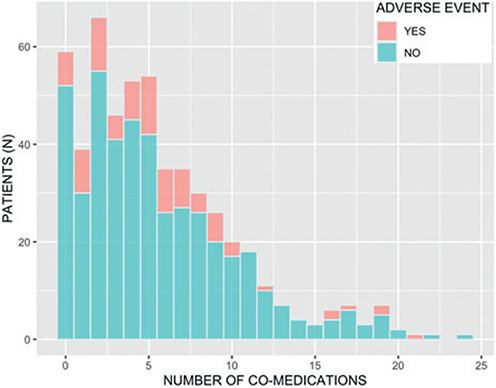
Fig. 1. Number of medications and associated adverse events.
Across all treatments, 349 therapies (65.4%) were carried out under a potentially light-sensitising medication according to SMPC. Adverse events occurred in 17.8% of therapies with a potentially photosensitising co-medication, and in 15.9% of the treatments without co-medication classified as potentially photosensitising. If drugs were taken that were “frequently” (1 x acyclovir, 1x benazepril, 1x clomipramine, 1 x valaciclovir) or “very frequently” (3 x doxycycline, 1 x amiodarone) associated with increased photosensitivity, the rate of adverse events in each of the groups was 25% (not statistically significant). Treatment with doxycycline was discontinued in one patient due to intolerance, and a low target dose was achieved with clomipramine.
Analysis of drug classes that were reported to be used during phototherapy by at least 20 patients showed no statistically significant association with the frequency of adverse events. Analysis of individual drugs that were reported to be used during phototherapy by at least 20 patients showed a nominally significant association only for L-thyroxine (Fig. 2).
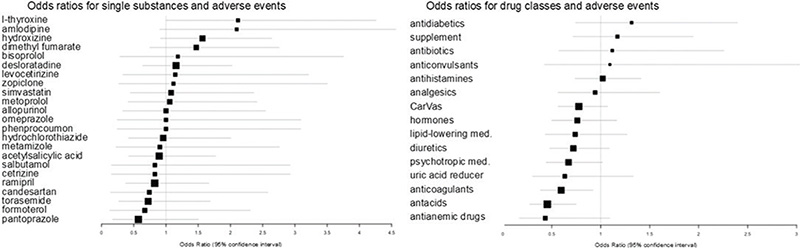
Fig. 2. Odds ratios for single substances or drug classes and adverse events. CarVas: cardiovascular medication; med.: medication.
Several substances and drug classes were significantly associated with particular types of adverse events in the unadjusted analysis, e.g. including antihistamines such as hydroxyzine with an odds ratio of 3.0 (95% CI 1.6–5.8), as well as cardiovascular drugs such as amlodipine with an odds ratio of 2.9 (95% CI 1.1–7.1) (Fig. S1). After adjustment for multiple testing these associations were no longer significant.
DISCUSSION
In the current study, no significant correlation was found between the tolerability of NB-UVB therapy and concomitant medication. This is of relevance because a large majority of patients in our analysis used at least one medication, including medications classified as potentially photosensitising. Thus, the available information from SMPC on the light-sensitising potential of drugs appears to be of limited value to the clinical practice of NB-UVB therapy.
The largest group investigated in this study was patients with psoriasis. In general, patients with psoriasis are a population for which phototherapy is well described (13, 14). In our study, 11.8% of the patients with psoriasis experienced adverse events with NB-UVB therapy. The most frequent type of reported AE was a low target dose in 6.1% of cases. Compared with the literature, adverse events with NB-UVB therapy occur in 3.9–28.6% of psoriasis cases (15–18), depending on the study design and definition of adverse events. The occurrence of severe erythema was found in 3.9% of patients with psoriasis in one study (18). In our study, severe erythema was reported in 1.2%. For atopic dermatitis and other types of eczema, the rate of adverse events was significantly higher than for psoriasis. Atopic dermatitis has a particularly high prevalence in the young population (19), while other forms of eczema often occur at an older age (20). Bulur et al. were able to demonstrate the occurrence of erythema in 35% of elderly patients when photosensitising drugs were taken concomitantly under NB-UVB therapy (21), which is much more frequent than in our study. However, phototherapy is still considered to be a safe form of therapy, even in older patients (22, 23). Even in diseases described as photosensitive, such as mycosis fungoides, the rate of adverse events was no higher than in eczema. In our study, adverse events occurred in 23.5%, which is in line with the literature, where adverse events are described in 21.4% (21).
In our study, severe erythema reactions were most common among patients with atopic dermatitis, which is in line with the literature, where erythema reactions during NB-UVB therapy are also frequently described in patients with atopic dermatitis (24). In the literature, a discontinuation of phototherapy due to AE was described in up to 6.7% of patients with atopic dermatitis (25), which is higher than in our study (2.2%).
For a variety of drugs, a photosensitising potential has been described and the simultaneous intake of such medication during phototherapy can potentially lead to drug-induced photosensitivity reactions. Guidelines propose individual MED testing if potentially photosensitising medication is taken concomitantly (26). However, it remains quite undefined as to which medications are photosensitising. Various sources suggested different medications to be considered photosensitising, often without robust evidence (10–12, 27, 28). In SMPCs we found a large number of medications that are reported to be associated with photosensitivity. In patients who used groups of co-medication classified as photosensitising according to the SMPC there was a slightly increased, but not statistically significant, rate of adverse events with 17.8% compared with treatments without such co-medication (11.9%) or co-medication not classified as potentially photosensitising (15.9%). These groups did not clearly differ with regard to AE. Likewise, the tolerability of phototherapy did not differ significantly when considering individual substances according to their photosensitising potential. Our study demonstrates that in routine practice the concomitant intake of drugs with and without suggested photosensitising potential is very common and that the incidence of adverse reactions seems to be weakly associated at best with the intake of such drugs. The type of skin disease treated appears to be more strongly associated with adverse events than the co-medication, although overall differences were small.
A few therapies were carried out even under concomitant use of medication with a suggested strong light-sensitising potential, without, however, an excessive increase in adverse events. Nevertheless, a medication history should always be taken before and during the implementation of UV phototherapy (29). Our data suggest that MED testing can be postponed in favour of careful dose finding, as no serious side effects were observed in our study design.
Strengths and limitation
The data were obtained retrospectively from archived phototherapy plans prepared by different investigators in daily routine. No uniform criteria for documentation were established in advance, which resulted in non-uniform documentation. Despite a reasonably high overall number of treatments evaluated, the number of cases with individual medication was low in many instances. Based on the large amount of data, it was possible to analyse the adverse events in detail and a review of the therapy safety of NB-UVB therapy in everyday clinical practice could be prepared.
Conclusion
This work shows that NB-UVB therapy is a safe form of therapy overall that can also be carried out with concomitant medication. Before starting the therapy, a medication history should be taken. We did not observe a robust association of AE with the use of potentially photosensitising drugs. It appears that the photosensitising potential of many drugs is partly overestimated in light of the frequency of their use. However, if potentially photosensitising drugs are taken, clinicians should still aim for careful dose finding to be able to guarantee safe therapy even in the presence of light-sensitising medication.
REFERENCES
- Moller KI, Kongshoj B, Philipsen PA, Thomsen VO, Wulf HC. How Finsen’s light cured lupus vulgaris. Photodermatol Photoimmunol Photomed 2005; 21: 118–124.
- Roelandts R. Photodermatology over the past 125 years. Br J Dermatol 2014; 171: 926–928.
- Brodsky M, Abrouk M, Lee P, Kelly KM. Revisiting the history and importance of phototherapy in dermatology. JAMA Dermatol 2017; 153: 435.
- Vangipuram R, Feldman SR. Ultraviolet phototherapy for cutaneous diseases: a concise review. Oral Dis 2016; 22: 253–259.
- Hannuksela-Svahn A, Sigurgeirsson B, Pukkala E, Lindelof B, Berne B, Hannuksela M, et al. Trioxsalen bath PUVA did not increase the risk of squamous cell skin carcinoma and cutaneous malignant melanoma in a joint analysis of 944 Swedish and Finnish patients with psoriasis. Br J Dermatol 1999; 141: 497–501.
- Hearn RM, Kerr AC, Rahim KF, Ferguson J, Dawe RS. Incidence of skin cancers in 3867 patients treated with narrow-band ultraviolet B phototherapy. Br J Dermatol 2008; 159: 931–935.
- Lee E, Koo J, Berger T. UVB phototherapy and skin cancer risk: a review of the literature. Int J Dermatol 2005; 44: 355–360.
- Shephard SE, Panizzon RG. Carcinogenic risk of bath PUVA in comparison to oral PUVA therapy. Dermatology 1999; 199: 106–112.
- Kurz B, Berneburg M, Bäumler W, Karrer S. Phototherapy: theory and practice. J Dtsch Dermatol Ges 2023; 21: 882–897.
- Hofmann GA, Weber B. Medikamenten-induzierte Photosensibilität: auslösende Medikamente, mögliche Mechanismen und klinische Folgen. J Dtsch Dermatol Ges 2021; 19: 19–30.
- Selvaag E. Clinical drug photosensitivity: a retrospective analysis of reports to the Norwegian Adverse Drug Reactions Committee from the years 1970–1994. Photodermatol Photoimmunol Photomed 1997; 13: 21–23.
- Stein KR, Scheinfeld NS. Drug-induced photoallergic and phototoxic reactions. Expert Opin Drug Saf 2007; 6: 431–443.
- Beani JC, Jeanmougin M. Narrow-band UVB therapy in psoriasis vulgaris: good practice guideline and recommendations of the French Society of Photodermatology. Ann Dermatol Venereol 2010; 137: 21–31.
- Barros NM, Sbroglio LL, Buffara MO, Baka J, Pessoa AS, Azulay-Abulafia L. Phototherapy. An Bras Dermatol 2021; 96: 397–407.
- Klein A, Schiffner R, Schiffner-Rohe J, Einsele-Krämer B, Heinlin J, Stolz W, et al. A randomized clinical trial in psoriasis: synchronous balneophototherapy with bathing in Dead Sea salt solution plus narrowband UVB vs. narrowband UVB alone (TOMESA-study group). J Eur Acad Dermatol Venereol 2011; 25: 570–578.
- Eysteinsdóttir JH, Ólafsson JH, Agnarsson BA, Lúðvíksson BR, Sigurgeirsson B. Psoriasis treatment: faster and long-standing results after bathing in geothermal seawater. A randomized trial of three UVB phototherapy regimens. Photodermatol Photoimmunol Photomed 2014; 30: 25–34.
- Iversen L, Conrad C, Eidsmo L, Costanzo A, Narbutt J, Pinter A, et al. Secukinumab demonstrates superiority over narrow-band ultraviolet B phototherapy in new-onset moderate to severe plaque psoriasis patients: week 52 results from the STEPIn study. J Eur Acad Dermatol Venereol 2023; 37: 1004–1016.
- Koek MB, Buskens E, van Weelden H, Steegmans PH, Bruijnzeel-Koomen CA, Sigurdsson V. Home versus outpatient ultraviolet B phototherapy for mild to severe psoriasis: pragmatic multicentre randomised controlled non-inferiority trial (PLUTO study). BMJ 2009; 338: b1542.
- Chen WY, Chen SC, Hsu SY, Lin YA, Shih CM, Huang CY, et al. Annoying psoriasis and atopic dermatitis: a narrative review. Int J Mol Sci 2022; 23: 4898.
- Tétart F, Joly P. Eczema in elderly people. Eur J Dermatol 2020; 30: 663–667.
- Bulur I, Erdogan HK, Aksu AE, Karapınar T, Saracoglu ZN. The efficacy and safety of phototherapy in geriatric patients: a retrospective study. An Bras Dermatol 2018; 93: 33–38.
- Matthews SW, Pike K, Chien AJ. Phototherapy: safe and effective for challenging skin conditions in older adults. Cutis 2021; 108: E15–E21.
- Torres AE, Lyons AB, Hamzavi IH, Lim HW. Role of phototherapy in the era of biologics. J Am Acad Dermatol 2021; 84: 479–485.
- Patrizi A, Raone B, Ravaioli GM. Safety and efficacy of phototherapy in the management of eczema. Adv Exp Med Biol 2017; 996: 319–331.
- Musters AH, Mashayekhi S, Harvey J, Axon E, Lax SJ, Flohr C, et al. Phototherapy for atopic eczema. Cochrane Database Syst Rev 2021; 10: Cd013870.
- Wolf P. The 2022 British guidelines for narrowband ultraviolet B phototherapy: an absolute necessity for anyone administering or prescribing phototherapy. Br J Dermatol 2022; 187: 285–286.
- Moore DE. Drug-induced cutaneous photosensitivity: incidence, mechanism, prevention and management. Drug Saf 2002; 25: 345–372.
- Schauder S. Phototoxische Reaktionen der Haut durch Medikamente. Deutsches Ärzteblatt 2005; 102: A 2314–2319.
- Patrizi A, Raone B, Ravaioli GM. Management of atopic dermatitis: safety and efficacy of phototherapy. Clin Cosmet Investig Dermatol 2015; 8: 511–520.