QUIZ SECTION
Coexistence of Vitiligo and Hyperpigmentation: A Quiz
Laure LEMARCQ1,2, Maarten DE VIS3, Sophie DEWEER4, Jan GUTERMUTH1,2 and Brigitte VELKENIERS5
1SKIN Research Group, Vrije Universiteit Brussel (VUB), 2Department of Dermatology, Vrije Universiteit Brussel (VUB), Universitair Ziekenhuis Brussel (UZ Brussel), 3Department of Endocrinology, Vrije Universiteit Brussel (VUB), Universitair Ziekenhuis Brussel (UZ Brussel), 4Department of Endocrinology and Diabetology, Algemeen Ziekenhuis Sint-Elisabeth Zottegem, and 5Department of Internal Medicine, Vrije Universiteit Brussel (VUB), Universitair Ziekenhuis Brussel (UZ Brussel), Laarbeeklaan 101, BE-1090 Brussels, Belgium. E-mail: laure.lemarcq@uzbrussel.be
Citation: Acta Derm Venereol 2024; 104: adv35429. DOI: https://doi.org/10.2340/actadv.v104.35429.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-Non-Commercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Published: Feb 21, 2024
We report here a 62-year-old man with long-standing Cushing’s disease. The patient had persistent hypercortisolaemia despite repeated resection of the pituitary adenoma. Pharmacological therapy was unsuccessful. Ultimately, he underwent bilateral adrenalectomy after which biochemical remission was achieved and symptoms resolved. Further follow-up was unremarkable, except that vitiligo appeared.
Two years postoperatively, he presented with severe headache, vision loss and hyperpigmentation of the skin areas not affected by vitiligo (Fig. 1). Laboratory testing showed a steep rise in adrenocorticotrophic hormone (ACTH) and magnetic resonance imaging (MRI) revealed a large sellar tumour. Debulking surgery was performed and tissue pathology was compatible with an aggressive ACTH-secreting pituitary tumour (Ki-67 > 50%, P53 > 50%).

Fig. 1. Clinical presentation. Photograph of the patient’s head and neck showing a sharp demarcation between skin areas with depigmentation due to vitiligo, and skin areas not affected by vitiligo with profound hyperpigmentation. The patient is deceased. His son has given written informed consent to publication of his father’s case details.
What is your diagnosis?
Differential diagnosis 1: Nelson’s syndrome
Differential diagnosis 2: Chronic Addison’s disease
Differential diagnosis 3: Ectopic ACTH syndrome
Differential diagnosis 4: Acquired hemochromatosis
See next page for answer.
ANSWERS TO QUIZ
The Coexistence of Vitiligo and Hyperpigmentation: A Commentary
Diagnosis: Nelson’s syndrome
Because the triad hyperpigmentation, excessive ACTH secretion, and an ACTH-secreting pituitary tumour was present, the diagnosis of Nelson’s syndrome was made (1). Nelson’s syndrome is a rare complication of bilateral adrenalectomy (1). Despite adjuvant radio-chemotherapy, the patient developed bone and liver metastases (Fig. 2). He opted for palliative care and died 1 month later.
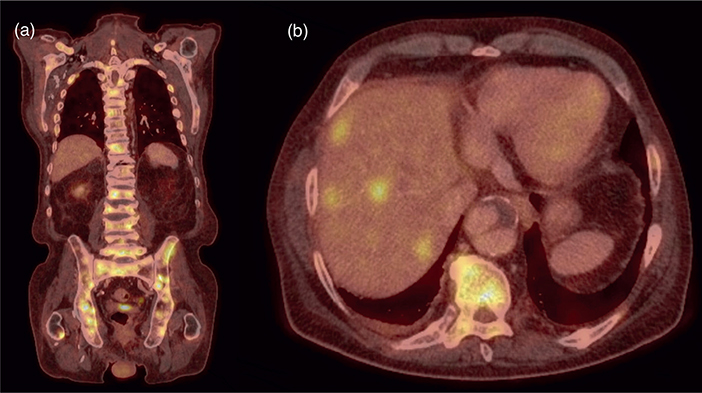
Fig. 2. Whole-body fluorine-18 (F-18) fluoro-2-deoxyglucose (FDG) positron emission (PET)/computed tomography (CT). (a) Coronal F-18 FDG PET/CT image showing numerous hypermetabolic bone lesions (yellow) indicative of bone metastases. (b) Axial F-18 FDG PET/CT image showing multiple hypermetabolic liver lesions (yellow) indicative of liver metastases.
The coexistence of 2 contrasting dermatological conditions, vitiligo and hyperpigmentation, forms a remarkable clinical image in which the patient’s normal skin colour is no longer visible.
As a reminder, Cushing’s disease occurs when the pituitary gland produces excessive levels of ACTH due to a benign pituitary tumour. In response, the adrenal glands produce too much cortisol, resulting in hypercortisolaemia.
We hypothesize that the appearance of vitiligo after treating Cushing’s disease is not an incidental finding. Due to hypercortisolaemia, the active phase of Cushing’s disease is associated with a state of immunosuppression (2, 3). After disease remission, and thereby normalization of hypercortisolaemia, rebound autoimmunity may occur (2, 3). A wide range of new-onset and exacerbations of autoimmune diseases during the remission phase of Cushing’s disease was reported, including autoimmune thyroiditis, Graves’ disease, coeliac disease, rheumatoid arthritis, sarcoidosis, and vitiligo, as illustrated by this case (2, 3). However, the exact mechanism leading to autoimmunity after remission of Cushing’s disease is not yet fully understood (2).
Bilateral adrenalectomy is an effective and definitive treatment for patients with Cushing’s disease refractory to pituitary surgery, radiotherapy, or pharmacological treatment (4). Although, it exposes patients to the risk of developing Nelson’s syndrome (4). In patients with Cushing’s disease, bilateral adrenalectomy resolves hypercortisolaemia, but also releases the hypothalamic–pituitary–adrenal axis from the negative feedback control of cortisol (5, 6). Without negative feedback, corticotrophin-releasing hormone levels rise, resulting in increased production of proopiomelanocortin and its subsequent products ACTH and alpha-melanocyte stimulating hormone (4–6). Both ACTH and alpha-melanocyte-stimulating hormone stimulate melanogenesis by binding melanocortin-1 receptors on melanocytes and keratinocytes (7, 8). Furthermore, it is hypothesized that excessive corticotrophin-releasing hormone levels after bilateral adrenalectomy can lead to the progression of a residual corticotroph tumour, contributing to the abundance of circulating ACTH (4, 6). Consequently, the profound hyperpigmentation characteristic of Nelson’s syndrome results from excessive ACTH secretion (8). In the current case, the hyperpigmentation is particularly visible in contrast to the skin areas affected by vitiligo.
To our knowledge this is the first published case of a patient with coexistence of vitiligo and hyperpigmentation due to underlying endocrine disorders. The development of vitiligo is an example of rebound autoimmunity after remission of Cushing’s disease, which underlines the necessity of close follow-up after treating Cushing’s disease to early detect autoimmune diseases. Moreover, this case demonstrates that hyperpigmentation after bilateral adrenalectomy may be an indication of Nelson’s syndrome as a rare, but potentially life-threatening, postoperative complication. In conclusion, it is vital to identify skin abnormalities as potential manifestations of endocrine diseases.
REFERENCES
- Nelson DH, Meakin JW, Dealy JB Jr, Matson DD, Emerson K Jr, Thorn GW. ACTH-producing tumor of the pituitary gland. N Engl J Med 1958; 259: 161–164.
- Pivonello R, Isidori AM, De Martino MC, Newell-Price J, Biller BM, Colao A. Complications of Cushing’s syndrome: state of the art. Lancet Diabetes Endocrinol 2016; 4: 611–629.
- da Mota F, Murray C, Ezzat S. Overt immune dysfunction after Cushing’s syndrome remission: a consecutive case series and review of the literature. J Clin Endocrinol Metab 2011; 96: E1670–1674.
- Fountas A, Karavitaki N. Nelson’s syndrome: an update. Endocrinol Metab Clin North Am 2020; 49: 413–432.
- Patel J, Eloy JA, Liu JK. Nelson’s syndrome: a review of the clinical manifestations, pathophysiology, and treatment strategies. Neurosurg Focus 2015; 38: E14.
- Barber TM, Adams E, Ansorge O, Byrne JV, Karavitaki N, Wass JA. Nelson’s syndrome. Eur J Endocrinol 2010; 163: 495–507.
- Herraiz C, Martínez-Vicente I, Maresca V. The α-melanocyte-stimulating hormone/melanocortin-1 receptor interaction: a driver of pleiotropic effects beyond pigmentation. Pigment Cell Melanoma Res 2021; 34: 748–761.
- Slominski A, Tobin DJ, Shibahara S, Wortsman J. Melanin pigmentation in mammalian skin and its hormonal regulation. Physiol Rev 2004; 84: 1155–1228.