ORIGINAL REPORT
A Comparative Analysis of the Predictors, Extent and Impacts of Self-stigma in Patients with Psoriasis and Atopic Dermatitis
Sophie SCHLACHTER1, Rachel SOMMER1, Matthias AUGUSTIN1, Athanasios TSIANAKAS2 and Lukas WESTPHAL1
1German Center for Health Services Research in Dermatology (CVderm), Institute for Health Services Research in Dermatology and Nursing (IVDP), University Medical Center Hamburg-Eppendorf (UKE), Hamburg and 2Fachklinik Bad Bentheim, Department of Dermatology, Bad Bentheim, Germany
The impact of dermatological diseases goes beyond symptoms and often includes psychosocial burden. Self-stigmatization plays a key role in this relationship and was compared in patients with psoriasis and atopic dermatitis to evaluate the validity of cross-disease stigmatization models. In total, 101 patients per indication were included in this cross-sectional study. Besides sociodemographic and clinical data, patient-reported outcome measures relating to self-stigmatization, depression, anxiety, and quality of life were compared across groups. Sociodemographic and clinical factors were tested for their moderating effects between self-stigmatization and quality of life. Group mean comparisons yielded no significant differences in self-stigmatization between patient groups. In both diseases, self-stigmatization significantly predicted depression and anxiety symptoms as well as quality of life. Current symptoms, not having close social relationships, and lower age predicted self-stigma in patients with psoriasis, whereas the involvement of sensitive body areas, the sum of previous treatments, and female sex were predictors in patients with atopic dermatitis. In both groups, symptoms had significantly moderating effects. The results underline the relevance of self-stigmatization in patients with chronic skin diseases. Awareness should be raised, screening implemented, and psychosocial support offered early on. Assessments, conceptual models of self-stigma, and interventions are probably applicable for both diseases.
Key words: atopic dermatitis; anxiety; depression; psoriasis; stereotyping; quality of life.
SIGNIFICANCE
Patients with chronic skin diseases often experience psychosocial impairment alongside somatic effects. This can have a considerable influence on their entire lives. Stigmatization, especially when generated by oneself, is a key element in the relationship between social, demographic, and clinical factors and quality of life, feelings of depression, and anxiety. Therefore, the mechanisms of self-stigmatization should be studied so that screenings can be developed, and appropriate interventions devised, thus reducing the psychological and social burdens on affected individuals and thereby empowering them throughout their lives.
Citation: Acta Derm Venereol 2023; 103: adv3962. DOI https://doi.org/10.2340/actadv.v103.3962.
Copyright: © Published by Medical Journals Sweden, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/)
Accepted: Mar 2, 2023; Published: Apr 4, 2023
Corr: Sophie Schlachter, German Center for Health Services Research in Dermatology (CVderm), Institute for Health Services Research in Dermatology and Nursing (IVDP), University Medical Center Hamburg-Eppendorf, Gebäude West 38 (W38), Martinistr. 52, DE-20246 Hamburg, Germany. E-mail: sophie.schlachter@stud.uke.uni-hamburg.de
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Psoriasis and atopic dermatitis (AD) are common chronic inflammatory skin diseases, with the former affecting approximately 2% of children (1) and 1–5% of adults (2), and the latter affecting approximately 20% of children and 1–9% of adults in Europe (3). Their visible and burdensome symptoms often give rise to negative emotions, exclusion, discrimination, social damage (including socioeconomic constrains), as well as negative self-perceptions, stigmatization, and exacerbation of existing conditions (4, 5). Consequently, patients experience sustained impacts on their somatic and psychological health as well as quality of life (QoL), and can face lifelong challenges as a result of the effects of these conditions on their careers and relationships (6, 7). Some researchers have characterized these challenges as “cumulative life course impairment” (8). Stigmatization plays a key role in this (4). WHO, in a 2014 resolution, called for a need to “raise awareness regarding the disease of psoriasis, including awareness of stigmatization” to foster acceptance and treatment solutions for people with psoriasis (9). This led to further research and the development of destigmatization programs. The authors of one German study (10) have suggested that self-stigmatization is a persistent thread running through all stages of an affected person’s life.
According to Link & Phelan (11), stigma can be viewed as manifested in a series of events whereby “elements of labeling, stereotyping, separation, status loss, and discrimination co-occur in a power situation that allows these processes to unfold”. Corrigan & Watson (12) expanded on this argument by distinguishing between external or public stigmatization and internal or self-stigmatization; in other words, when affected people are aware of, agree to, and apply the stereotypes that are conferred on them by external, predominantly social attitudes, this leads to them legitimating these preconceptions and therefore stigmatizing themselves (12). Some psychology researchers into stigma have suggested further refining the notion of self-stigma into internalized stigma, felt or perceived stigma, and enacted stigma (13) (middle part of Fig. 1). Felt stigma has been the most commonly studied phenomenon (14) in visible skin diseases (VSD). It is important to distinguish the types and subtypes of stigma and the correlations between them in order to devise tailored and effective approaches to combat stigma. Summarizing the inter-relationships between (self-)stigmatization and its underlying drivers, QoL, impacts, and coping strategies, Germain et al. (15) devised the first conceptual model of stigma in VSD. As well as taking into account sociodemographic variables, we can identify clinical characteristics, such as severity and localization/visibility, as key drivers. Lower age, a younger age of onset, as well as a lower age of (self-)diagnosis, all influence the manifestations and impacts of stigma. Psoriasis and AD have both been associated with depression and anxiety, which are themselves correlated with the age of (self-)-diagnosis or the time since diagnosis, and stigmatization of these conditions can, this contribution argues, lead to impairment of QoL (Fig. 1).

Fig. 1. Model of (self)-stigmatization (summarized from (11–13, 15)).
Based on the conceptual model in VSD and its implications, it is advisable first to study different VSD to complement the generic model. Secondly, identifying disease-specific drivers may help to specify interventions and hence reduce or prevent stigma (15). Several studies have found evidence that the type of VSD influences external and perceived stigmatization, such that the extent of stigma and its impacts may also vary with different manifestations of VSD (15). In this context, a cross-disease model is applied here for examining occurrences of stigma for compared diseases. It can be applied if predictors for stigma are similar, and in cases where its extent and impacts are identifiable with similar degrees of intensity. A cross-disease model enables common destigmatization programs to be more effectively devised for larger patient groups. So far, interventions have tended to focus only on specific VSD (16). Research into stigmatization (more than 60% of the studies) has mainly concentrated on patients with psoriasis (15). A knowledge gap could be identified for AD. It is well known that this erythematous scaly skin condition, presenting similar symptoms to psoriasis, is one of the most stigmatized conditions, although stigmatization and its correlations have rarely been studied, and usually with respect to incidence in children (5, 17). These studies found that severity (5, 18), involvement of sensitive body regions (19), and visibility (19) were associated with stigmatization. However, Halioua et al. (17) found no predictive evidence for sex, severity, and disease duration, only a younger age was predictive. Compared with the relative lack of studies relating to AD, we benefit from more widely studied factors in patients with psoriasis, such as lower age (20, 21), female sex (22), lower levels of educational attainment (21, 23), being unemployed (24), early age of onset (20, 24), longer disease duration (20, 21, 25), not having a partner (21), severity (21, 26), involvement of genital areas (27), visibility (21, 25, 27), itching/frequency of scratching (28, 29), living in the countryside (20), and type D personality (21). However, age, sex, education, employment status, relationship status, and involvement of genital areas have only been intermittently discussed regarding predictive effects and tendencies. Other characteristics have also been less studied, e.g. body mass index (BMI), subjective severity, having children, and the application of biological treatment (18, 22). Moreover, there have so far been few comparisons regarding feelings of stigmatization between patients with psoriasis and those with AD (18, 23) and the only common predictor examined to date has been the feeling of helplessness (23).
Therefore, the primary aim of this study was to compare the conceptual self-stigma models in patients with psoriasis and those with AD, in order to determine whether a cross-disease model is applicable and hence whether common screenings and anti-stigma interventions can be envisaged as effective treatment options.
Specifically, this study analysed self-stigmatization comparatively, with a focus on: the level of self-stigmatization; sociodemographic and clinical predictors; impacts on depression, anxiety, and QoL; and moderators in terms of the relationship between self-stigma and QoL.
MATERIALS AND METHODS
Recruitment
Data were collected in four German dermatology centers from January to July 2021. Patients were approached during their visits and included in the study if: they were at least 18 years old; they understood the project and the questions; had signed a document giving their informed consent; and had received a diagnosis either of plaque-type psoriasis or of AD.
Participants as well as medical staff completed a questionnaire. The study is based on a quantitative cross-sectional data collection. It was approved by the ethics commission for psychological studies at the University Medical Center Hamburg-Eppendorf (UKE) in Germany based on the Declaration of Helsinki.
Materials
The patient questionnaire consisted of three parts.
In the first part, sociodemographic data was gathered, regarding:
- age; sex; education (without, low, middle, and high education); relationship status (single [dichotomous]; in a partnership/married [dichotomous]; separated/divorced/widowed [dichotomous]), living alone (dichotomous); having children (dichotomous); having children in the household (dichotomous); currently having close social relationships (dichotomous); being employed (dichotomous);
as well as clinical data, relating to:
- time between first symptoms and diagnosis; disease duration; anogenital involvement, either currently or ever (both dichotomous).
Patients also completed a form detailing a list of treatments they had received, for each of their previous treatments. The sum of these was included as a variable. Afterwards, patients were asked to draw the extent of their skin lesions on a body grid map that featured a total of 1,424 squares (30). From this map the extent of affected visible body areas (hands, forearms, head, neck) and sensitive body areas (axillary, breast and nipples, submammary, genital, anal, inguinal, gluteal) was calculated with the aid of circled squares. Participants were also asked to estimate the severity of their skin lesions and the intensities of their symptoms, in terms of pain, itching, and burning on numerical rating scales. The second part of the patient questionnaire applied:
- the German version of the Feelings of Stigmatization Questionnaire (FSQ) (24) for psoriasis and an adapted version for AD: 33-item score, from “strongly disagree” (0 points) to “strongly agree” (5 points), range 0–165, with higher values specifying greater self-stigmatization, subscales/factors: I. Anticipation of rejection, II. Feelings of being flawed, III. Sensitivity to the opinions of others, IV. Guilt and shame, V. Positive attitudes, VI. Secretiveness. (see Appendix S1).
The third part of the patient questionnaire used:
- the Perceived Health Questionnaire (PHQ-2) and the Generalized Anxiety Disorder Scale (GAD-2) (31, 32): 2-item scores, range 0–6, cut-off scores ≥ 3 indicating severe symptoms of depression/anxiety;
- the Dermatology Life Quality Index (DLQI) (33): 10-item score, range 0–30, with higher values implying lower QoL; >10 was considered as very extensive impairment.
The physician questionnaire included information about height, weight, the current treatment based on whether this was: topical therapy (dichotomous); systemic (not biological) therapy (dichotomous); biological therapy (dichotomous); phototherapy (dichotomous); and information about comorbidities (for descriptive purposes).
The authors also deployed the following measures:
- Global Clinical Assessment (GCA) (34): 1-item score, range 0–4, 0 standing for “none”, 1 “mild”, 2 “moderate”, 3 “intense”, and 4 “very intense” severity;
- Body surface area (BSA) (35): range 0–100%, < 10 considered as mild, > 10 as moderate to severe skin disease;
- Psoriasis Area and Severity Index (PASI) (35): range 0–72, score ≥ 10 indicating moderate to severe psoriasis;
- Eczema Area and Severity Index (EASI) (36): range 0–72, > 1 “mild”, > 7 “moderate”, > 21 “severe”, > 50 very severe AD.
Statistical analyses
All analyses are based on a group comparison between patients with psoriasis and AD. Descriptive analyses were performed using standard parameters (absolute/relative frequencies, means, standard deviation). For comparisons, either a Mann-Whitney U test, a χ2 test, or t-tests were calculated. The subscales of the FSQ were compared based on their mean values (range 0–5) since the subscales consisted of varying numbers of items. An analysis of variance (ANOVA) was used to identify significant differences between subscales and diagnoses. To identify predictors for self-stigmatization, linear regression analyses were undertaken, taking into account sociodemographic parameters (e.g., age) and clinical variables (e.g., GCA) after a common variable selection, including calculations of correlations and t-tests as well as variable exclusion for reasons of multicollinearity. Afterwards, three linear regressions were computed to gauge the impact of the FSQ on PHQ-2, GAD-2, and DLQI. Finally, selected variables associated with the FSQ were tested to explore their possible moderating effects on the relationship between FSQ and DLQI. QoL was chosen among the impacts as this can be affected by stigma (15) and is assumed to reflect the occurrence of everyday impairments in all patients. All statistical analyses were performed by the program Statistical Package for the Social Sciences version 26.0 (SPSS by IBM, Armonk, NY) and the add-on PROCESS version 4.0 (written by Andrew F. Hayes, Calgary, Alberta, Canada). Statistical significance was determined at the p < 0.05 level.
RESULTS
In total, 101 patients with plaque-type psoriasis and 101 patients with AD were included. A total of 32 patients refused to participate or had to be excluded due to lack of time (68.75%) or interest (31.25%). Patients with psoriasis were mainly inpatients at a specialist clinic in Bad Bentheim (71.3%), whereas the most of the participants with AD were outpatients recruited at the Institute for Health Services Research in Dermatology and Nursing (IVDP), at the University Medical Center Hamburg-Eppendorf (UKE) (73.3%). Sociodemographic and clinical data are shown in Table I and Table SI.
| Psoriasis | AD | Comparison between groups | ||
| t/Z/χ2 | p-value | |||
| Age, years, mean ± SD | 53.05 ± 11.43a | 40.41 ± 16.43 | t = 6.339 | < 0.001*** |
| Sex, n (%) | χ2 = 1.996 | 0.158 | ||
| Male | 60 (59.4) | 50 (49.5) | ||
| Female | 41 (40.6) | 51 (50.5) | ||
| High school graduation, n (%) | Z = –6.343 | < 0.001*** | ||
| Without | 3 (3)b | 1 (1)a | ||
| Low graduation | 34 (33.7)b | 8 (7.9)a | ||
| Middle graduation | 39 (38.6)b | 23 (22.8)a | ||
| High graduation | 25 (24.8)b | 68 (67.3)a | ||
| Close social relationships, n (%) | χ2 = 8.659 | 0.003** | ||
| No | 33 (32.7)a | 15 (14.9)b | ||
| Yes | 67 (66.3)a | 84 (83.2)b | ||
| Duration of disease, years, mean ± SD | 19.44 ± 15.65b | 29.3 ±16.01c | t = –4.440 | < 0.001*** |
| Past or current anogenital involvement, n (%) | χ2 = 3.164 | |||
| No | 36 (35.6) | 58 (57.4) | ||
| Yes | 65 (64.4) | 43 (42.6) | ||
| Sensitive body areas, mean ± SDd | 20.18 ± 26.32a | 12.62 ± 22.45 | t = 2.191 | 0.030* |
| Visible body areas, mean ± SDe | 34.39 ± 40.91a | 53.20 ± 53.83 | t = –2.790 | 0.006** |
| Intensity of symptoms, mean ± SD | ||||
| Pain | 3.21 ± 2.91 | 2.84 ± 3.00 | t = 0.881 | 0.380 |
| Pruritus | 4.42 ± 3.30 | 4.01 ± 2.85 | t = 0.937 | 0.350 |
| Burning | 3.45 ± 3.13 | 3.25 ± 3.16 | t = 0.447 | 0.655 |
| Body mass index, kg/m2, mean ± SD | 30.11 ± 6.03a | 25.72 ± 5.25 | t = 5.505 | < 0.001*** |
| GCA, mean ± SD | 2.03 ± 1.100 | 1.43 ± 0.931 | t = 4.213 | < 0.001*** |
| PASI, mean ± SD | 10.13 ± 11.17 | N/A | – | – |
| Min–Max | 0–59.40 | N/A | – | – |
| EASI, mean ± SD | N/A | 5.79 ± 7.74 | – | – |
| Min–Max | N/A | 0–35.30 | – | – |
| aMissing values: 1, bmissing values: 2, and cmissing values: 7 (of 101 in total). dMax. 141 squares of the body grid map. eMax. 264 squares of the body grid map. | ||||
| AD: atopic dermatitis; SD: standard deviation; t: t-test; Z: Mann-Whitney U test; N/A: not applicable; GCA: Global Clinical Assessment (range 0–4); PASI: Psoriasis Area and Severity Index (range 0–72); EASI: Eczema Area and Severity Index (range 0–72; *p < 0.05, **p < 0.01, ***p < 0.001.). | ||||
Despite these differences, neither the total score of the FSQ nor any of its subscales revealed significant differences between patients with psoriasis and those with AD. In both groups, the total scores made up approximately 44–45% of the maximum possible FSQ score of 165 points. Moreover, the means of subscales were ranked in the same way, on the basis of: 1. Anticipation of rejection, 2. Guilt and shame, 3. Positive attitudes, 4. Sensitivity to the opinions of others, 5. Feelings of being flawed, and 6. Secretiveness (Fig. 2, Table II and Table SII). The subscales “Anticipation of rejection”, “Guilt and shame”, and “Secretiveness” differed highly significantly from each other and from all the other subscales (Table SIII).
| Psoriasis | AD | Comparison between groups | ||
| t | p-value | |||
| FSQ total, mean ± SD | 75.06 ± 25.11a | 72.92 ± 24.34a | t = 0.590 | 0.556 |
| Min–Max | 18.00–123.00a | 17.00–127.00a | ||
| Factor I: Anticipation of rejection, mean ± SD | 3.22 ± 0.93b | 3.03 ± 0.90 | t = 1.525 | 0.129 |
| Min–Max | 0.5–5.00b | 0.38–4.88 | ||
| Factor II: Feelings of being flawed, mean ± SD | 1.99 ± 1.08 | 1.78 ± 1.21 | t = 1.285 | 0.200 |
| Min–Max | 0–4.83 | 0–4.83 | ||
| Factor III: Sensitivity to the opinions of others, mean ± SD | 2.07 ± 1.06c | 2.07 ± 1.14d | t = 0.310 | 0.976 |
| Min–Max | 0–4.80c | 0–4.40d | ||
| Factor IV: Guilt and shame, mean ± SD | 2.52 ± 1.11c | 2.76 ± 0.97d | t = –1.565 | 0.119 |
| Min–Max | 0–4.80c | 0.60–4.60d | ||
| Factor V: Positive attitudes, mean ± SD | 2.10 ± 1.01 | 2.10 ± 1.07b | t = 0.037 | 0.970 |
| Min–Max | 0–4.25 | 0–4.75b | ||
| Factor VI: Secretiveness, mean ± SD | 1.11 ± 0.84 | 0.99 ± 0.78 | t = 1.111 | 0.268 |
| Min–Max | 0–4.00 | 0–3.60 | ||
| PHQ-2, mean ± SD | 2.10 ± 1.73 | 1.58 ± 1.35 | t = 2.310 | 0.022* |
| GAD-2, mean ± SD | 2.02 ± 1.86 | 1.52 ± 1.47e | t = 2.110 | 0.036* |
| DLQI, mean ± SD | 9.29 ± 7.26 | 7.68 ± 6.75 | t = 1.626 | 0.105 |
| aMissing values: 8, bmissing values: 2, cmissing values: 4, dmissing values: 3, emissing values: 1 (of 101 in total). | ||||
| AD: atopic dermatitis; SD: standard deviation; t: t-test; FSQ: Feelings of Stigmatization Questionnaire (range 0–165); factors I–VI (range 0–5); PHQ: Patient Health Questionnaire (range 0–6); GAD: Generalized Anxiety Disorder (range 0–6); DLQI: Dermatology Life Quality Index (range 0–0); * p < 0.05, ** p < 0.01, *** p < 0.001. | ||||
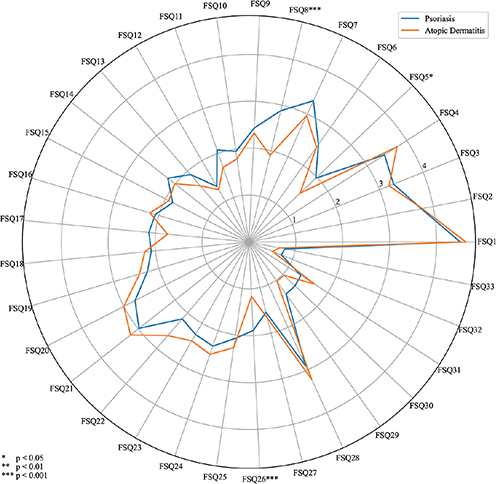
Fig. 2. Distributions of the Feelings of Stigmatization Questionnaire (FSQ).
Regarding further patient-reported outcomes, patients with psoriasis reported significantly more feelings of depression and anxiety than patients with AD, though both groups recorded mean scores below the cut-off points (≤ 3), such as not having severe symptoms of depression or anxiety. The mean scores of QoL were moderately lower in both groups, with no significant distinction (Table II).
Assessing sociodemographic and clinical characteristics for their associations with the FSQ in both diseases, this study could identify significant correlations with: female sex, lower education, not having currently close social relationships, having been affected at some point (“ever”) in anogenital areas, a higher sum of previous treatments, sensitive body areas, and reported symptoms of pain, itching, and burning. Age was significant only in patients with psoriasis, while patients with AD showed significant correlations with objective severity scores (GCA and EASI). These significant variables were included in the regression model. For reasons of multicollinearity, the variable “burning” was chosen, having the greatest degree of correlation among highly correlating symptoms. The GCA was prioritized as a generic severity score. In both diseases, significant differences in the extent of the FSQ could not be identified when it came to the variables relationship status, living alone, having children, having children in the household, employment status, time between first symptoms and diagnosis, disease duration, BMI, BSA, and type of treatment. However, the following variables were associated with higher stigma scores in patients with psoriasis: having children (p = 0.207), having children in the household (p = 0.058), and being employed (p = 0.070). In both groups links to more stigmatization were: subjective severity (p = 0.075), current anogenital involvement (p = 0.195), being treated with topical therapy (p = 0.122) and with non-biological systemic therapy (p = 0.162), although receiving biological (p = 0.157) or phototherapeutic interventions (p = 0.181) were both connected with less stigmatization. Prevalence in visible body areas showed no link to the FSQ (p = 0.512), but was included in the regression model because of evidence of this variable in the literature.
Looking at predictors from the FSQ among selected sociodemographic and clinical variables, the results from the linear regression analyses revealed the symptom skin burning, not having close social relationships and a lower age with decreasing effect size as significant predictors for patients with psoriasis, accounting for 20.9% of the variance. On the other hand, for patients with AD, the predictors higher sum of previous treatments, greater involvement of sensitive body areas, and female sex significantly influenced (in descending order) the extent of the FSQ, accounting for 34.8% of the variance. There was not a single significant predictor in common (Table III).
| Predictor variables | Model coefficients | Cohen’s f² | p-value | Model summary | |
| Unstandardized B [95% CI] | Standardized beta | Adjusted R² | |||
| Psoriasis | |||||
| Age | –0.534 [–0.966; –0.102] | –0.238 | 0.08 | 0.016* | 0.209 |
| Sex | 8.391 [–1.561; 18.343] | 0.164 | 0.04 | 0.097 | |
| Graduation | –3.085 [–9.038; 2.868] | –0.101 | 0.01 | 0.305 | |
| Close social relationships | –15.046 [–25.564; –4.527] | –0.284 | 0.10 | 0.006** | |
| Visible body regions | –0.570 [–0.198; –0.084] | –0.096 | 0.01 | 0.424 | |
| Sensitive body regions | 0.009 [–0.221; 0.238] | 0.009 | 0.00 | 0.941 | |
| Sum of previous treatments | 0.637 [–0.564; 1.838] | 0.109 | 0.01 | 0.295 | |
| Anogenital involvement ever | 6.779 [–3.590; 17.147] | 0.129 | 0.02 | 0.197 | |
| Burning of skin | 2.709 [0.914; 4.505] | 0.330 | 0.12 | 0.004** | |
| GCA | –3.760 [–9.213; 1.693] | –0.167 | 0.02 | 0.174 | |
| Atopic dermatitis | |||||
| Age | –0.019 [–0.332; 0.294] | –0.012 | 0.00 | 0.903 | 0.348 |
| Sex | 10.459 [1.455; 19.464] | 0.215 | 0.07 | 0.023* | |
| Graduation | –6.434 [–13.001; 0.133] | –0.180 | 0.05 | 0.055 | |
| Close social relationships | –1.259 [–14.095; 11.576] | –0.019 | 0.02 | 0.846 | |
| Visible body regions | 0.002 [–0.091; 0.095] | 0.004 | 0.00 | 0.968 | |
| Sensitive body regions | 0.337 [0.092; 0.582] | 0.311 | 0.10 | 0.008** | |
| Sum of previous treatments | 1.493 [0.527; 2.459] | 0.289 | 0.17 | 0.003** | |
| Anogenital involvement ever | 9.078 [–0.400; 18.557] | 0.185 | 0.05 | 0.060 | |
| Burning of skin | –0.198 [–1.767; 1.371] | –0.025 | 0.00 | 0.802 | |
| GCA | 4.047 [–1.254; 9.348] | 0.158 | 0.03 | 0.133 | |
| B: regression coefficient; 95% CI: 95% confidence interval; Beta: standardized regression coefficient; Cohen’s f²: effect size; R²: coefficient of determination; GCA: Global Clinical Assessment (range 0–4); *p < 0.05, **p < 0.01, ***p < 0.001. | |||||
In turn, the FSQ predicted with high significance the PHQ-2, GAD-2, and the DLQI scores in both groups. However, the effect sizes were high in patients with psoriasis and only medium in patients with AD with the strongest impact on QoL. In these models, more variance could be explained for patients with psoriasis (27.6–28.6%) than for patients with AD (10.1–14.1%). Thus, the model for the effects of self-stigmatization applied more closely to patients with psoriasis. Nevertheless, feelings of depression, anxiety and a lessening of QoL can be considered as impacts of self-stigmatization in both diseases (Table IV).
| Predicted variable | Predictor variables | Model coefficients | Cohen’s f² | p-value | Model summary | |
| Unstandardized B [95% CI] | Standardized beta | Adjusted R² | ||||
| Psoriasis | ||||||
| PHQ-2 | FSQ – Total | 0.038 [0.028; 0.050] | 0.532 | 0.39 | 0.001*** | 0.276 |
| GAD-2 | 0.040 [0.030; 0.051] | 0.542 | 0.42 | 0.001*** | 0.286 | |
| DLQI | 0.158 [0.106; 0.210] | 0.535 | 0.40 | < 0.001*** | 0.278 | |
| AD | ||||||
| PHQ-2 | FSQ – Total | 0.018 [0.004; 0.033] | 0.332 | 0.12 | 0.021* | 0.101 |
| GAD-2 | 0.021 [0.010; 0.034] | 0.363 | 0.15 | 0.001*** | 0.122 | |
| DLQI | 0.108 [0.055; 0.161] | 0.388 | 0.18 | < 0.001*** | 0.141 | |
| B: regression coefficient; CI: confidence interval; Beta: standardized regression coefficient; Cohen’s f²: effect size; R²: coefficient of determination; PHQ: Patient Health Questionnaire (range 0–6); GAD: Generalized Anxiety Disorder (range 0–6); DLQI: Dermatology Life Quality Index (range 0–30); AD: atopic dermatitis; FSQ: Feelings of Stigmatization Questionnaire (range 0–165); *p < 0.05, **p < 0.01, ***p < 0.001. | ||||||
The moderation analysis in the psoriasis group showed an interaction of the symptoms burning, itching and pain as well as of the GCA on the relationship between the FSQ and the DLQI, with a stronger effect, indicated by higher point values. For patients with AD the moderating effect of the GCA was not significant, although in this group all three symptoms also indicated stronger moderating effects with related higher point values. All moderating inter-actions were significant, with medium and strong effects (Tables SIV and SV).
To sum up, in spite of the heterogeneous samples, the extent, impacts and moderators of self-stigmatization are comparable in patients with psoriasis and AD, albeit its predictors differed.
DISCUSSION
This study assessed the extent, sociodemographic factors, clinical aspects, and psychosocial impacts of self-stigmatization in patients with psoriasis and AD, with the aim of determining whether a cross-disease stigma model is applicable, and with a view to the feasibility in applying previously unproven common anti-stigma interventions.
Both patient groups showed moderate levels of feelings of stigmatization without any significant differences and with the same ranking of the subscales. For patients with psoriasis, the total FSQ score is in accordance with some earlier studies, e.g. (37), and slightly lower compared with more recent studies (22, 25). This discrepancy could be explained by various environmental, cultural, socio-economic and clinical factors (16). Caution is needed when comparing FSQ scores, because studies carried out in different countries have rated response possibilities in different ways (20, 28). One of the few comparisons of feelings of stigmatization in patients with psoriasis and AD also did not reveal distinct differences (18). The most apparent feelings of stigmatization were reported in the subscales “Anticipation of rejection” and “Guilt and shame”. An explanation could be that educational work and public campaigns might address risks involved in keeping the conditions secret or may recommend patients not to associate their disease with some perceived personal “weakness”. Nevertheless, patients may experience deeply internalized and persistent feelings, sometimes built up over a period of years. This underlines the need for specific self-stigma interventions that target patients. With regard to particular types of self-stigma, one treatment approach could be to address the ways in which people feel stigmatized, in order to explore more tailored approaches. It might be worthwhile enhancing self-esteem and self-efficacy if internalized stigma prevails (12) and introducing coping strategies for enacted stigma (13). To sum up, the results relating to felt stigma confirm the relevant levels and similarities of perceived stigmatization in both diseases, and this is a strong case for adopting cross-disease models. The FSQ seems appropriate as a measuring instrument, not just for patients with psoriasis, but also for patients with AD.
The similar extent of self-stigma in patient groups is unexpected, considering that patients with AD were mainly outpatients having biological treatments and presenting lower severity. Interestingly, neither subjective severity, objective severity, or visibility could be identified as predictors for feelings of stigmatization in both diseases, although they have been described as key drivers for stigma in VSD (15). Nonetheless, there was a small, yet significant, correlation of objective severity to patients with AD, being in line with earlier studies (5, 18), and a moderating effect of objective severity on the relationship between self-stigma and QoL in patients with psoriasis. These findings emphasize that the development of self-stigma tends to be determined by personal evaluation of present lesions and the individual perception of self-efficacy (23) rather than by objective severity and visibility (7, 21, 25). The current study found sensation of burning, currently close social relationships, and younger age to be predictors in patients with psoriasis. In contrast, in patients with AD, the sum of previous treatments, the involvement of sensitive body areas, and female sex were identified as factors underlying the propensity to self-stigmatize. Symptoms moderated the relationship between felt stigma and QoL in both diseases. Confirming earlier studies, e.g. in (21), younger patients with psoriasis might care more about social integration (29), beauty stereotypes, and supposed ideals of perfection (38), leading to higher FSQ scores. It is important to note that all symptoms would probably have had a predictive effect in patients with psoriasis as they exhibited high multicollinearity, although the variable “burning” had the highest correlation in both diseases. A relatively minor skin lesion might soon be forgotten or its impact in everyday life minimized, but perceiving this as evidence of a skin disease might lead someone to constantly feel different, thereby reinforcing a propensity to identify with stigmatized groups. A recent study found evidence that patients with moderate/severe itching yearned for a decrease in sensation of burning (29). By scratching, patients can relieve for a short while the sensation of itching, but, as a consequence, the skin barrier is destroyed, and patients may feel powerless in the face of an increased sensation of burning. A feeling of being helpless has been identified by some researchers as a strong predictor in psoriasis and AD (23). Having currently close social relationships significantly lowered the incidence of self-stigmatizing for patients in both diseases and can be viewed as a form of psychological protection, as a previous study had also suggested (23). However, it seems that social factors influence the development of self-stigma in patients with psoriasis more than in those with AD. As such, close social contacts predicted the occurrence of felt stigma in patients with psoriasis, while the variables related to having children (especially those still living in the household) and being employed also tend to increase feelings of stigmatization. In contrast to a recent study (17), this study could identify sex differences in felt stigma in patients with AD. Reflecting gender stereotypes, women face greater social pressure to fulfill stereotypes of appearance, as women’s accomplishments tend to be assessed by their appearance (38). Thus, having a VSD creates double distress for women with AD because they might be stigmatized both for their VSD and because they are female. The sum of previous treatments reflects how many different therapies someone has tried and the switch to other medical approaches because of unsuccessful results. As a consequence, patients might feel, similar to patients with psoriasis and their symptoms, hopeless and powerless, thus supporting the presence of the predictor “helplessness” (23). An earlier study has suggested that sensitive body areas were more important than visible body areas (19), and this is in line with the current study, which provides evidence that sensitive body areas are a predictor for self-stigma in patients with AD. One explanation could be that these areas are particularly relevant for intimate relationships and the perception of oneself in terms, e.g. self-disgust and self-acceptance (39). The results of the current study further indicate that, in both diseases, it is not the effect of any particular episode of anogenital involvement that is important for participants, rather, their experience of having been affected at any point (“ever”) in their lives is associated with feelings of stigmatization. This suggests that, that even if an episode occurred in the past, negative emotions associated with this experience can nevertheless accumulate and reinforce self-stigmatization. Regarding drivers for self-stigma, psoriasis and AD differed in all their predictors. This suggests that different conditions shape self-stigma in these VSD. Notwithstanding, a feeling of helplessness could probably be a common predictor. The regression model also fitted more closely for patients with AD, accounting for 14% more of the variance. This argues against a cross-disease model for drivers of stigma and for disease-specific approaches when tackling and treating the origins of self-stigma.
The results of the current study imply, for both patient groups, that self-stigma leads, with high significance, to feelings of depression, anxiety and QoL impairment. Levels of impacts can be seen in the data, especially impairment of QoL, which accords with other findings (6, 7, 15). However, the levels of depression and anxiety were slightly (but still significantly) lower in patients with AD than in patients with psoriasis. Lower severity and the existence of current social contacts as a protective factor (23) could be responsible for these differences. Furthermore, self-stigmatization accounted for 39–40% of the variance in the regression models in psoriasis, which is more than double that of patients with AD. Thus, for patients with AD, other factors might play a role in the development of the impacts mentioned and would repay further study. In the context of social neuroscience, it might be taken into account that psoriasis and AD differ in pathomechanisms and in various activities of body mediators. This might lead to different biological impacts on the development of psychological comorbidities. Again, further research is needed in this field (40). Considering impacts as a component of any effective stigma model, the same impacts on and connections with self-stigma were found, although few differences in their extent could be identified.
Study limitations
Firstly, patient groups differed in sociodemographic and clinical variables, which complicates comparisons. Secondly, patients were recruited at special care units after passing through other healthcare services, often for years and without treatments that were satisfactory over the long term. Thirdly, participants were selected based on the recruiting day rather conducting a fully representative preselection. Finally, a cross-section study is only a snapshot of a sometimes long-lasting impairment and cannot be expected to demonstrate unambiguous causality.
Conclusion
In summary, a cross-disease model is not fully applicable. However, all the overlaps in extent, impacts, moderators, and their interconnections can be used for introducing common screening instruments and anti-stigma interventions with a focus on “Anticipation of rejection” and “Guilt and shame”. Apart from the importance of dermatological treatment for alleviating symptoms in patients with psoriasis and the involvement of sensitive body areas in patients with AD, interventions in both groups should be introduced on an intrapersonal basis. Counselling, skills building, coping strategies (problem or emotion-based), reinforcement of self-esteem and self-efficacy, and psychological education to change attitudes, implicit beliefs, behavior responses, and self-concepts seem promising when it comes to both diseases (12, 13, 16) and could be accomplished in both groups together, in particular for younger patients with psoriasis and women with AD. Cognitive behavior therapy should be offered early on if depression and anxiety occur (7) and social support encouraged in both groups. In future research, predictors for AD should be better explored and reviewed for psoriasis.
Concluding from this study, the following practical implications should be taken into consideration:
- Screenings for self-stigma, depression, anxiety, and QoL should be implemented in all dermatological visits in order to raise awareness and reinforce psychosocial care.
- Dermatological treatment should focus particularly on reducing symptoms in patients with psoriasis and limiting changes in treatments and the involvement of sensitive body areas in patients with AD in order to mitigate the development of self-stigmatization.
- If self-stigmatization occurs, its impact on feelings of depression, anxiety, and QoL can be diminished by reducing symptoms in both diseases.
- Common anti-stigma interventions on an intrapersonal level should be introduced and offered, especially to young patients with psoriasis and women with AD.
- Psychological and social support should be offered and given to both patient groups.
ACKNOWLEDGEMENTS
The study was approved by the ethics commission for psychological studies at the University Medical Center Hamburg-Eppendorf in Germany based on the Declaration of Helsinki.
Statements: The abstract of this paper has been accepted for publication at the 21st German Congress for Health Services Research (21. Deutscher Kongress für Versorgungsforschung) and at the 31st Congress of the European Academy of Dermatology and Venereology. The statistical analyses were conducted in collaboration with the Institute for Health Services Research in Dermatology and Nursing (IVDP) research group and the Institute for Biometric and Epidemiology was also consulted.
REFERENCES
- Mahé E. Childhood psoriasis. Eur J Dermatol 2016; 26: 537–548.
- Parisi R, Iskandar IYK, Kontopantelis E, Augustin M, Griffiths CEM, Ashcroft DM. National, regional, and worldwide epidemiology of psoriasis: systematic analysis and modelling study. Bmj 2020; 369: m1590.
- Bylund S, Kobyletzki LB, Svalstedt M, Svensson Å. Prevalence and Incidence of Atopic Dermatitis: A Systematic Review. Acta Derm Venereol 2020; 100: adv00160.
- Sommer R, Topp J, Mrowietz U, Zander N, Augustin M. Perception and determinants of stigmatization of people with psoriasis in the German population. J Eur Acad Dermatol Venereol 2020; 34: 2846–2855.
- Chernyshov PV. Stigmatization and self-perception in children with atopic dermatitis. Clin Cosmet Investig Dermatol 2016; 9: 159–166.
- Sahi FM, Masood A, Danawar NA, Mekaiel A, Malik BH. Association Between Psoriasis and Depression: A Traditional Review. Cureus 2020; 12: e9708.
- Wittkowski A, Richards HL. How beneficial is cognitive behaviour therapy in the treatment of atopic dermatitis? A single-case study. Psychol Health Med 2007; 12: 445–449.
- Augustin M. Cumulative life course impairment: identifying patients at risk. Curr Probl Dermatol 2013; 44: 74–81.
- World Health Organization (WHO). Resolutions and Decisions. Sixty-Seventh World Health Assembly. Geneva, 2014.
- Sommer R, Augustin M, Mrowietz U, Topp J, Schäfer I, von Spreckelsen R. Stigmatisierungserleben bei Psoriasis – qualitative Analyse aus Sicht von Betroffenen, Angehörigen und Versorgern. Hautarzt 2019; 70: 520–526.
- Link BG, Phelan JC. Conceptualizing stigma. Annual Review of Sociology 2001; 27: 363–385.
- Corrigan PW, Watson AC. The paradox of self-stigma and mental illness. Clinical Psychology: Science and Practice 2002; 9: 35–53.
- Bos AER, Pryor JB, Reeder GD, Stutterheim SE. Stigma: advances in theory and research. Basic and Applied Social Psychology 2013; 35: 1–9.
- Luck-Sikorski C, Roßmann P, Topp J, Augustin M, Sommer R, Weinberger NA. Assessment of stigma related to visible skin diseases: a systematic review and evaluation of patient-reported outcome measures. J Eur Acad Dermatol Venereol 2022; 36: 499–525.
- Germain N, Augustin M, François C, Legau K, Bogoeva N, Desroches M, et al. Stigma in visible skin diseases – a literature review and development of a conceptual model. J Eur Acad Dermatol Venereol 2021; 35: 1493–1504.
- Topp J, Andrees V, Weinberger NA, Schäfer I, Sommer R, Mrowietz U, et al. Strategies to reduce stigma related to visible chronic skin diseases: a systematic review. J Eur Acad Dermatol Venereol 2019; 33: 2029–2038.
- Halioua B, Bastien M, Taieb C, Thenie C, Veniard C, Noel M, et al. Prevalence and predictors of perceived stigmatization in adult patients with moderate-to-severe atopic dermatitis in France. J Eur Acad Dermatol Venereol 2023; 37: e80-e81.
- Schmid-Ott G, Burchard R, Niederauer HH, Lamprecht F, Künsebeck HW. Stigmatisierungsgefühl und Lebensqualität bei Patienten mit Psoriasis und Neurodermitis. Hautarzt 2003; 54: 852–857.
- Schmid-Ott G, Kuensebeck HW, Jaeger B, Werfel T, Frahm K, Ruitman J, et al. Validity study for the stigmatization experience in atopic dermatitis and psoriatic patients. Acta Derm Venereol 1999; 79: 443–447.
- Kowalewska B, Cybulski M, Jankowiak B, Krajewska-Kułak E. Acceptance of illness, satisfaction with life, sense of stigmatization, and quality of life among people with psoriasis: a cross-sectional study. Dermatol Ther (Heidelb) 2020; 10: 413–430.
- van Beugen S, van Middendorp H, Ferwerda M, Smit JV, Zeeuwen-Franssen ME, Kroft EB, et al. Predictors of perceived stigmatization in patients with psoriasis. Br J Dermatol 2017; 176: 687–694.
- Hawro M, Maurer M, Weller K, Maleszka R, Zalewska-Janowska A, Kaszuba A, et al. Lesions on the back of hands and female gender predispose to stigmatization in patients with psoriasis. J Am Acad Dermatol 2017; 76: 648–654.e2.
- Lu Y, Duller P, van der Valk PGM, Evers AWM. Helplessness as Predictor of Perceived Stigmatization in Patients with Psoriasis and Atopic Dermatitis. Dermatology and Psychosomatics / Dermatologie und Psychosomatik 2003; 4: 146–150.
- Ginsburg IH, Link BG. Feelings of stigmatization in patients with psoriasis. J Am Acad Dermatol 1989; 20: 53–63.
- Jankowiak B, Kowalewska B, Krajewska-Kułak E, Kowalczuk K, Khvorik DF. The sense of stigmatization in patients with plaque psoriasis. Dermatology 2021; 237: 611–617.
- Kowalewska B, Jankowiak B, Cybulski M, Krajewska-Kułak E, Khvorik DF. Effect of disease severity on the quality of life and sense of stigmatization in psoriatics. Clin Cosmet Investig Dermatol 2021; 14: 107–121.
- Łakuta P, Marcinkiewicz K, Bergler-Czop B, Brzezińska-Wcisło L, Słomian A. Associations between site of skin lesions and depression, social anxiety, body-related emotions and feelings of stigmatization in psoriasis patients. Postepy Dermatol Alergol 2018; 35: 60–66.
- Dimitrov D, Matusiak Ł, Szepietowski JC. Stigmatization in Arabic psoriatic patients in the United Arab Emirates – a cross sectional study. Postepy Dermatol Alergol 2019; 36: 425–430.
- Sommer R, Augustin M, Hilbring C, Ständer S, Hubo M, Hutt HJ, et al. Significance of chronic pruritus for intrapersonal burden and interpersonal experiences of stigmatization and sexuality in patients with psoriasis. J Eur Acad Dermatol Venereol 2021; 35: 1553–1561.
- Augustin M, Sommer R, Kirsten N, Danckworth A, Radtke MA, Reich K, et al. Topology of psoriasis in routine care: results from high-resolution analysis of 2009 patients. Br J Dermatol 2019; 181: 358–365.
- Löwe B, Wahl I, Rose M, Spitzer C, Glaesmer H, Wingenfeld K, et al. A 4-item measure of depression and anxiety: validation and standardization of the Patient Health Questionnaire-4 (PHQ-4) in the general population. J Affect Disord 2010; 122: 86–95.
- Kroenke K, Spitzer RL, Williams JB, Monahan PO, Löwe B. Anxiety disorders in primary care: prevalence, impairment, comorbidity, and detection. Ann Intern Med 2007; 146: 317–325.
- Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI) – a simple practical measure for routine clinical use. Clin Exp Dermatol 1994; 19: 210–216.
- Cappelleri JC, Bushmakin AG, Harness J, Mamolo C. Psychometric validation of the physician global assessment scale for assessing severity of psoriasis disease activity. Qual Life Res 2013; 22: 2489–2499.
- Mrowietz U, Kragballe K, Reich K, Spuls P, Griffiths CE, Nast A, et al. Definition of treatment goals for moderate to severe psoriasis: a European consensus. Arch Dermatol Res 2011; 303: 1–10.
- Leshem YA, Hajar T, Hanifin JM, Simpson EL. What the Eczema Area and Severity Index score tells us about the severity of atopic dermatitis: an interpretability study. Br J Dermatol 2015; 172: 1353–1357.
- Zięciak T, Rzepa T, Król J, Żaba R. Stigmatization feelings and depression symptoms in psoriasis patients. Psychiatr Pol 2017; 51: 1153–1163.
- Ellemers N. Gender Stereotypes. Annu Rev Psychol 2018; 69: 275–298.
- Schienle A, Wabnegger A. Self-disgust in patients with dermatological diseases. Int J Behav Med 2022; 29: 827–832.
- Fabrazzo M, Cipolla S, Signoriello S, Camerlengo A, Calabrese G, Giordano GM, et al. A systematic review on shared biological mechanisms of depression and anxiety in comorbidity with psoriasis, atopic dermatitis, and hidradenitis suppurativa. Eur Psychiatry 2021; 64: e71.