ORIGINAL REPORT
Notalgia Paresthetica Dermatologist Report of Symptom Burden and Treatment: Results from a Physician Survey
Brian S. KIM1, Sonja STÄNDER2, Kenji KABASHIMA3, Jennifer A. MOHAWK4*, Sherri SO4*, Joana GONCALVES4*, Nilam SHAH4, Catherine MUNERA4, Joseph C. PUNZALAN5*, Romelia ARGUDO5 and MARK LEBWOHL1
1Icahn School of Medicine at Mount Sinai, New York, NY, USA, 2University Hospital Münster, Münster, Germany, 3Kyoto University Graduate School of Medicine, Kyoto, Japan, 4Cara Therapeutics, Stamford, CT, USA, 5AplusA Bell Falla, Newark, NJ, USA. *At the time of study conduct
Notalgia paresthetica (NP) is a sensory neuropathy characterized by chronic pruritus, skin pain, and other pathologic sensations affecting the mid-to-upper back. NP may be under-recognized and under-diagnosed, with limited data available on its symptom presentation and treatment patterns. NP-DERM was an internet-based survey of dermatologists (n = 650) from 8 different countries on their perspectives on NP symptoms and current treatment practices. Dermatologists typically treated a median of 12 patients with NP per month. Dermatologists reported that itch (pruritus) was the most common symptom for their patients with NP, followed by hyperpigmentation and sensitive skin. The most burdensome NP symptom was pruritus, followed by burning or hot sensation, and painful or raw skin. The most prescribed treatments included non-medicated skin care, topical corticosteroids, oral antihistamines, medicated topicals, and gabapentin or pregabalin. Physicians reported low satisfaction with available treatments. The most common reason for physicians to discontinue patients’ therapy was lack of response.
SIGNIFICANCE
Notalgia paresthetica (NP) is a sensory neuropathy characterized by chronic pruritus, which can lead to intense physical discomfort, decreased quality of life, and negative psychosocial impact. Limited information is available regarding its symptom presentation and treatment patterns. This online survey of dermatologists was conducted to better understand symptom burden and treatment journey for patients with NP. Dermatologists reported that pruritus was the most common and burdensome symptom. They primarily utilized topical therapies with low satisfaction. Additional research is needed to ensure early and accurate diagnosis for patients with NP and to identify safe and effective therapies.
Key words: notalgia paresthetica; pruritus; neuropathic itch; sensory neuropathy; dermatologist; physician survey.
Citation: Acta Derm Venereol 2024; 104: adv39941. DOI https://doi.org/10.2340/actadv.v104.39941.
Copyright: 2024 © The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Jan 22, 2024; Accepted after revision: May 30, 2024; Published: Sep 11, 2024
Corr: Joana Goncalves, MD, Cara Therapeutics, Stamford, CT, USA. E-mail: jgoncalves73@gmail.com
Competing interests and funding: BSK: Founder – Klirna Biotech; consultant – 23andMe, ABRAX Japan, AbbVie, Almirall, Amagma Therapeutics, Amgen, Arcutis Biotherapeutics, Arena Pharmaceuticals, argenx, AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Cara Therapeutics, Clexio Biosciences, Eli Lilly and Company, Escient Pharmaceuticals, Evommune, Galderma, Genentech, GlaxoSmith-Kline, Granular Therapeutics, Incyte Corporation, Innovaderm Research, Janssen, Kiniksa, LEO Pharma, Maruho, Novartis, Pfizer, Recens Medical, Regeneron Pharmaceuticals, Sanofi, Septerna, Vial, WebMD; stock in – ABRAX Japan, KliRNA Biotech, Locus Biosciences, and Recens Medical; patent for the use of JAK1 inhibitors for chronic pruritus; patent pending for the use of JAK inhibitors for interstitial cystitis; research grants – AbbVie, Cara Therapeutics, LEO Pharma, and Veradermics. SS: Speaker and/or consultant and/or investigator and/or has received research funding – AbbVie, Almirall, Beiersdorf, BMS, Clexio, Eli Lilly, FomF, Galderma, German Research Foundation (DFG), Integrity CE, Kiniksa, Leo Pharma, L’Oréal, MEDahead, Moroscience, NACCME, Novartis, Omnicuris, P.G. Unna Academy, Pfizer, Sanofi, TouchIME, UCB, Vifor, and WebMD. KK: Consulting fees and/or advisory board honoraria – Japan Tobacco Inc., Kao, LEO Pharma, Torii, Chugai Pharmaceutical, Maruho, Pola Pharma, AbbVie, Eli Lilly, Sanofi, and Pfizer; research grants – LEO Pharma, Japan Tobacco Inc., P&G Japan, Eli Lilly Japan, Tanabe Mitsubishi, Ono Pharmaceutical, Kyowa Kirin, Pola Pharma, AbbVie, Sanofi, Kose, Maruho, and Kyorin Pharmaceutical. NS, CM: Employment – Cara Therapeutics. JAM, SS, JG: Former employment – Cara Therapeutics. JCP: Former employment – AplusA Bell Falla, LLC. RA: Employment – AplusA Bell Falla, LLC. ML: Employment – Mount Sinai; research funding – AbbVie, Amgen, Arcutis, Avotres, Boehringer Ingelheim, Cara Therapeutics, Dermavant Sciences, Eli Lilly, Incyte, Inozyme, Janssen Research & Development, LLC, Novartis, Ortho Dermatologics, Regeneron, and UCB, Inc.; consultant - AnaptysBio, Arcutis, Inc., Arena Pharmaceuticals, Aristea Therapeutics, Avotres Therapeutics, BiomX, Boehringer Ingelheim, Brickell Biotech, Castle Biosciences, CorEvitas, Dermavant Sciences, Evommune, Inc., Facilitation of International Dermatology Education, Forte Biosciences, Foundation for Research and Education in Dermatology, Hexima Ltd., Meiji Seika Pharma, Mindera, Pfizer, Seanergy, and Verrica.
This study was sponsored by Cara Therapeutics, Inc.
INTRODUCTION
Notalgia paresthetica (NP) is a sensory neuropathy with chronic pruritus, skin pain, and dysesthesia, which can lead to intense physical discomfort, decreased quality of life, and negative psychosocial impact (1). NP is classified as a form of neuropathic itch and characterized by recurrent pruritus in the mid-to-upper back, typically unilaterally localized to the interscapular and paravertebral regions (2–4). The pathophysiology of NP remains unclear, though it is thought to be caused by intervertebral disk disease or vertebral degenerative changes, specifically affecting the thoracic nerves (3–5). In addition to pruritus, patients may experience other localized symptoms including burning, numbness, or tingling (1, 6). Skin discoloration, often presenting as hyperpigmentation of the affected region, and bleeding or scabbing may also occur secondary to scratching (1, 7). Recent case series and qualitative studies have enhanced our understanding of the condition (1, 6), yet much regarding the patient experience of NP remains poorly understood. The aim of the NP-DERM survey was to identify and describe physician perspectives on NP symptoms and patient burden as well as current practices in treating NP.
METHODS
The Notalgia Paresthetica Dermatologist Report of symptom burden and treatment (NP-DERM) study was an internet-based survey conducted by AplusA (Newark, NJ, USA) between 8 June and 28 July 2023. Institutional review board approval for data collection in the United States was received before the survey commenced; applicable regulations of other countries participating in the study were followed as well. All participants provided informed consent prior to participating in the survey.
Respondents were screened from an existing research panel of physicians in Canada, France, Germany, Italy, Japan, Spain, the United Kingdom, and the United States. For eligibility, respondents had to affirm they were board-certified dermatologists in practice for at least 2 years post-residency/training completion. Dermatologists were required to report spending at least 10% of their professional time dedicated to direct patient care with at least 40% of visits in medical dermatology (as opposed to cosmetic). As the focus of the survey was the diagnosis, characterization, and treatment of NP, respondents were required to report treating at least 1 NP patient per month. Respondents were excluded if a member of their household or immediate family worked in market research, advertising, or public relations.
Screening continued until the prespecified quotas were obtained (n = 650 respondents; n = 300 for the United States and n = 50 for each of the other countries). Survey topics included questions concerning respondent credentials, respondent medical practice characteristics, number of NP patients treated in a typical month, NP diagnoses and referrals, NP disease and symptom burden, and treatment patterns. Data are presented in the form of descriptive statistics.
RESULTS
Respondent population
Of 1,110 physicians screened, 650 met eligibility criteria and completed the survey. A total of 88 otherwise eligible screened respondents (representing 12% of the eligible respondents) reported treating no NP patients in a typical month and were not included in the survey. Survey respondents were board-certified dermatologists and had been practicing for a mean of 14.3 years since completion of residency/training (Table I). Participants spent the majority of their time dedicated to direct patient care, primarily in medical dermatology (Table I). Respondents were asked to estimate the average number of unique patients with NP they treat in a month, and 5 other dermatological conditions of varying prevalence (Table I; outliers ≥ 2 standard deviations above the mean were removed from reported patient-count summary statistics). The median number of patients with NP dermatologists reported treating in a typical month was 12 (Table I); the most common responses were 10 patients with NP (n = 97 responding dermatologists) followed by 5 patients with NP (n = 75 responding dermatologists) per month.
| Responses | n = 650 |
| Years practicing (since completion of residency/training), mean (SD) | 14.3 (9.24) |
| Percentage of professional time spent directly treating patients, mean (SD) | 92.2 (8.85) |
| Percentage of total patient visits for medical dermatology (vs cosmetic), mean (SD) | 88.5 (10.52) |
| No. of unique patients seen in a typical month (all conditions), mediana | 400 |
| Dermatologic conditions: no. of patients treated per month, mediana | |
| Atopic dermatitis | 60 |
| Brachioradial pruritus | 5 |
| Prurigo nodularis | 15 |
| Notalgia paresthetica | 12 |
| Psoriasis | 50 |
| Vitiligo | 10 |
| an = 643. | |
Patients referred to dermatologists for notalgia paresthetica symptoms often come in without an accurate diagnosis
To better understand the patient diagnostic journey, respondents were asked what percentage of their patients with NP are referred to them by another healthcare provider. Dermatologists reported that 44.5% of their patients with NP are referrals from other healthcare providers, with 83.1% of patients without an accurate diagnosis (Table II). Primary care providers were the most common referring physicians, followed by allergists. The complete list of referring specialties is reported in Table II.
| Survey question | Result |
| Percentage of NP patients referred by another HCP, mean (SD) | 44.5 (34.69) |
| Percentage of NP patients referred coming in WITHOUT a correct diagnosis (referring physician unable to diagnose the condition) | |
| n | 571 |
| Mean (SD) | 83.1 (21.98) |
| What specialties did the NP patients referred to you consult?a | |
| Primary care | 81.4% |
| Allergy | 22.1% |
| Dermatology | 21.4% |
| Neurology | 19.6% |
| Rheumatology | 15.6% |
| Pain management | 12.1% |
| Acupuncture | 7.9% |
| Orthopedics | 6.5% |
| aPercentage of respondents reporting they had patients who had seen each specialty/provider type. | |
| HCP: healthcare provider; NP: notalgia paresthetica. | |
Dermatologists consider pruritus to be the most frequent and bothersome symptom of notalgia paresthetica
Respondents were asked how frequently their patients experience various localized symptoms of NP using a 5-point Likert-type scale from “Never” to “Always.” The list of symptoms (itch or pruritus, bleeding or scabbing, hyperpigmentation, painful or raw skin, burning or hot sensation, sensitive skin, tenderness, numbness, and tingling) was derived from previous reports of NP symptoms (1, 6), and respondents had the opportunity to include additional symptoms in their responses. A total of 94.2% of dermatologists reported that their patients “Almost Always” or “Always” experienced itch or pruritus. The second most frequently reported symptoms were hyperpigmentation, with 56.6% of dermatologists reporting that patients “Almost Always” or “Always” experience this symptom, and sensitive skin, reported by 38.9% as occurring “Almost Always” or “Always.” Frequency histograms of the responses are shown in Fig. 1.

Fig. 1. Dermatologist-reported most frequent symptom of notalgia paresthetica (NP). Survey question: How frequently are NP patients experiencing the following localized symptoms?
In addition to frequency of symptoms, respondents were surveyed regarding the perceived burden of symptoms (list as above) on their patients with NP. This was assessed using a 5-point Likert-type scale from “Not at all Burdensome” to “Extremely Burdensome.” A total of 82.0% of dermatologists reported that their patients considered itch or pruritus to be “Very” or “Extremely Burdensome.” The second most burdensome symptoms were burning or hot sensation, as reported by 44.9% of respondents to be “Very” or “Extremely Burdensome” for their patients, and painful or raw skin, with 41.2% reporting it to be “Very” or “Extremely Burdensome.” Responses for all symptoms are shown in Fig. 2.
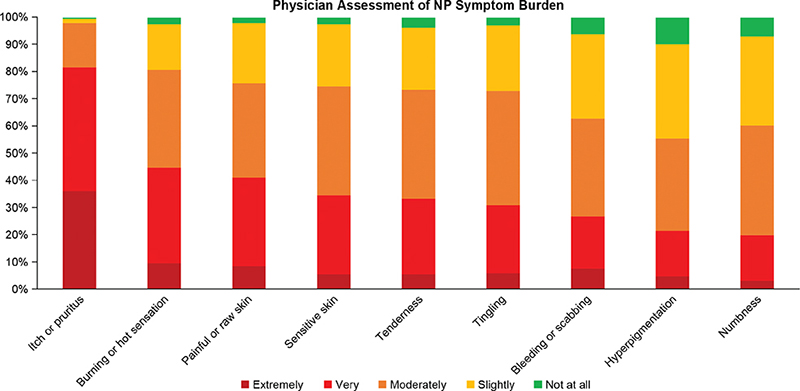
Fig. 2. Dermatologist-reported most burdensome symptom of notalgia paresthetica (NP). Survey question: How burdensome are these symptoms for your patients with NP?
Dermatologists use mainly topical therapies, with low treatment satisfaction
Survey participants were asked which therapies they recommend or prescribe for the signs and symptoms of NP, including both itch and non-itch symptoms (Table III). A list of therapies for NP was provided based on the published literature and survey respondents had the option to add additional therapies. Topical treatments were utilized by the majority of respondents to treat both itch and non-itch symptoms of NP. Systemic treatments were commonly recommended or prescribed with 80.7% of respondents utilizing gabapentin or pregabalin, and 71.3% utilizing oral antihistamines for managing itch due to NP. Respondents were less inclined to recommend or prescribe physical therapies and procedures, although over half reported that they recommend cold packs or physiotherapy for itch and/or non-itch symptoms of NP.
| Recommend/prescribe for ITCH due to NP | Recommend/prescribe for NON-ITCH signs/symptoms of NP | |||
| Use first, second, or third line (n = 649) | Estimated % of patients who received first line | Use first, second, or third line (n = 646) | Estimated % of patients who received first line | |
| Any topical treatment | 99.70% | 99.4% | ||
| Topical corticosteroids | 90.8% | 43.9% | 80.0% | 30.3% |
| Medicated topicalsa | 84.3% | 25.5% | 81.9% | 27.7% |
| Non-medicated skin care | 84.0% | 53.7% | 81.7% | 50.9% |
| Topical non-steroidal anti-inflammatory agents | 70.0% | 7.9% | 63.9% | 8.6% |
| Any systemic treatment | 95.4% | 91.2% | ||
| Gabapentin or pregabalin (Lyrica) | 80.7% | 9.1% | 77.2% | 14.6% |
| Oral antihistamines | 71.3% | 27.5% | 55.6% | 16.2% |
| Antidepressants to treat skin symptoms | 51.9% | 3.0% | 47.5% | 3.1% |
| OTC pain medications (e.g., acetaminophen) | 42.4% | 7.7% | 50.5% | 10.1% |
| Opioid-targeting agents | 28.2% | 0.6% | 26.8% | 0.5% |
| Botulinum toxin injections | 23.7% | 0.8% | 24.1% | 0.6% |
| Sodium channel blockers | 20.2% | 0.9% | 21.4% | 1.0% |
| Any physical therapies/procedures | 87.8% | 81.7% | ||
| Cold packs | 60.7% | 22.6% | 59.1% | 22.3% |
| Physiotherapy exercises | 51.9% | 16.1% | 50.6% | 15.5% |
| Phototherapy/narrowband UVB | 46.8% | 3.4% | 39.0% | 3.0% |
| EMS/TENS | 32.2% | 2.4% | 33.9% | 2.7% |
| Chiropractic care | 29.3% | 5.9% | 32.0% | 7.2% |
| aExamples of medicated topicals included topical non-steroidal anti-inflammatory agents (e.g., tacrolimus, crisaborole, ruxolitinib) and medicated topical neuromodulatory/analgesic agents (e.g., lidocaine, capsaicin). | ||||
| EMS: electronic muscle stimulation; NP: notalgia paresthetica; OTC: over-the-counter; TENS: transcutaneous electrical nerve stimulation; UVB: ultraviolet B. | ||||
For every therapy included in their treatment armamentarium, respondents were asked to estimate the percentage of their patients with NP for whom they recommend the therapy as first line. Despite the broad range of potential therapies being utilized by responding dermatologists, most of these options were recommended for a relatively small proportion of patients. The only therapies recommended as first-line for over 25.0% of patients, whether for itch or non-itch symptoms, included oral antihistamines, medicated topical treatments, topical corticosteroids, and non-medicated skin care (Table III).
Respondents were asked the common reasons for not initiating specific treatment types for their patients with NP. Regarding topical treatments, the most frequently cited reasons for non-initiation included lack of response (57% of respondents), poor patient compliance (44% of respondents), and the perceived burdensomeness of the method (41% of respondents). For systemic treatments, prevalent reasons for not initiating therapy included safety concerns, with 59% reporting patients’ concerns around safety and 50% expressing their own safety as treating physicians. Additional reasons included patient refusal (42% of respondents), and contraindications (41% of respondents). For physical modalities, the most common reasons reported for not initiating therapy were patient-access related, with 41% noting high cost for patients and 40% highlighting a lack of insurance coverage.
Dermatologists were asked about their satisfaction with each of the therapies they included in their treatment armamentarium for itch related to NP. Overall, satisfaction with itch treatment was low for all available therapies (Fig. 3). When asked why they may discontinue a treatment for a given patient with NP, the most reported reason for all classes of therapy was lack of response. Specifically, 73% of respondents cited lack of response as a reason for discontinuing topical treatments, 58% for systemic treatments, and 50% for physical modalities.
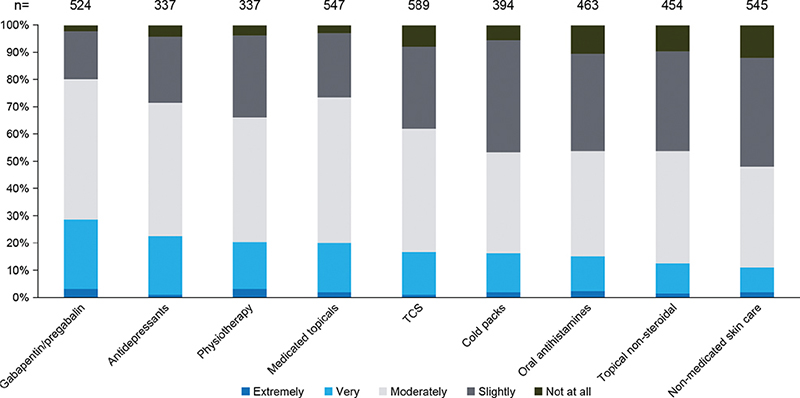
Fig. 3. Treatment satisfaction of available therapies. Therapies used first, second, or third line by at least half of the respondents. TCS: topical corticosteroid.
DISCUSSION
NP is thought to be an underrecognized, underdiagnosed condition. Perhaps because of this lack of recognition, there are limited data in the literature reporting patient and physician views on the symptoms and treatment of this condition.
Respondents were clinical dermatologists, spending over 90% of their time on direct patient care. They reported seeing an average of 400 patients per month, 12 of whom they were treating for NP. The median number of patients with NP in this study may appear higher than the typical dermatology practice, as the survey included dermatologists who encounter at least 1 NP patient per month. Some dermatologists infrequently treat NP patients, and most cases observed are a result of secondary skin changes induced by NP or visits for other dermatological concerns. Additionally, 88 dermatologists were excluded due to reporting 0 NP patients treated per month. There is also a possibility of recall bias amongst the respondents.
These dermatologists treating patients with NP consider pruritus to be the most frequently occurring and bothersome symptom of the condition and revealed a lack of consensus around best practices for treatment.
There are very few data available regarding the NP patient journey. In the current survey, dermatologists reported that 44.5% of their patients with NP were referrals from other healthcare providers, often without an accurate diagnosis. Not surprisingly, most of the referred patients come from primary care. However, the next most common referral source was allergists, followed by other dermatologists and then neurologists. It may be that patients are consulting allergists believing their symptoms to result from an allergic reaction or contact dermatitis. Additional research and engaging in patient interviews may provide greater clarity, facilitating improved education for both patients and non-dermatologist physicians. This, in turn, may contribute to earlier diagnosis for these patients.
Itch or pruritus was reported by dermatologists to be the most frequently occurring and most burdensome symptom of NP for their patients. This is in line with previous data in which all, or nearly all, patients with NP report experiencing itch (1, 6). In the current survey, dermatologists reported hyperpigmentation and sensitive skin to be the next most frequently occurring symptoms in their patients with NP, while they reported burning or hot sensation and painful or raw skin to be the second and third most burdensome symptoms (following pruritus). Dermatologists’ perceptions of the most common and bothersome symptoms of NP are likely influenced by what patients are expressing during the office visit or, in the case of hyperpigmentation, what the dermatologist observes during a physical examination. It is important to note that these perceptions may not necessarily cover all aspects of the condition. Nonetheless, dermatologists’ reports on symptom frequency and burden are likely indicative of the symptoms for which patients with NP actively seek treatment. Broader studies of NP patient-reported symptoms, treatment-seeking behavior, and quality-of-life impact are needed.
There are currently no approved therapies to treat NP, though a variety of topical, systemic, and physical therapies have been employed in clinical practice and reported in the literature. The surveyed dermatologists reported utilizing a broad range of therapies in their armamentarium, though only topical therapies and, in the case of treatments specific for itch, oral antihistamines were commonly reported as being used first-line. The latter is particularly interesting as chronic itch in NP is not thought to be histamine-mediated and it is likely that any efficacy derived from antihistamines for itch is due only to sedation (2, 8). The reluctant use of other therapeutic options may be due to the presumed safety of systemic therapies or in response to the intensity or bother of the symptoms reported by the patients. Conversely, it may reflect the lack of approved, efficacious, and accessible therapies for patients with NP. The broad range of therapies being utilized by the dermatologists in this survey, however, probably indicates the lack of consensus and evidenced-based treatment algorithms for managing NP. Indeed, overall treatment satisfaction was low and the primary reason dermatologists reported discontinuing any class of therapy was lack of response. This underscores the need for proven and effective therapies for NP.
This broad, international survey of dermatologists confirmed that pruritus is the hallmark feature of NP. The dermatologists surveyed noted that they are seeing several NP patients per month, many of whom are referrals lacking an accurate diagnosis. Dermatologists are primarily utilizing non-medicated topicals and topical corticosteroids to treat the skin lesions associated with NP but are unsatisfied with available therapies as they have little influence on the itch intensity. Additional research and consensus are needed to ensure early and accurate diagnosis for patients with NP and to identify safe and effective therapies for pruritus and other symptoms of NP.
ACKNOWLEDGMENTS
The authors thank the survey participants. They also gratefully acknowledge Peloton Advantage, LLC, an OPEN Health company, for medical writing and editorial support, which was funded by Cara Therapeutics, under the direction of the authors.
Data sharing: Please contact Cara Therapeutics for data inquiries.
REFERENCES
- Bacci ED, Currie BM, Wilson R, Qian J, Munera C, Nograles K. Understanding the patient experience of living with notalgia paresthetica: a qualitative interview study. JAAD Int 2022; 8: 94–101. https://doi.org/10.1016/j.jdin.2022.04.003
- Auyeung KL, Kim BS. Emerging concepts in neuropathic and neurogenic itch. Ann Allergy Asthma Immunol 2023; 131: 561–566. https://doi.org/10.1016/j.anai.2023.08.008
- Robinson C, Downs E, De la Caridad Gomez Y, Nduaguba C, Woolley P, Varrassi G, et al. Notalgia paresthetica review: update on presentation, pathophysiology, and treatment. Clin Pract 2023; 13: 315–325. https://doi.org/10.3390/clinpract13010029
- Šitum M, Kolić M, Franceschi N, Pećina M. Notalgia paresthetica. Acta Clin Croat 2018; 57: 721–725. https://doi.org/10.20471/acc.2018.57.04.14
- Howard M, Sahhar L, Andrews F, Bergman R, Gin D. Notalgia paresthetica: a review for dermatologists. Int J Dermatol 2018; 57: 388–392. https://doi.org/10.1111/ijd.13853
- Pereira MP, Lüling H, Dieckhöfer A, Steinke S, Zeidler C, Ständer S. Brachioradial pruritus and notalgia paraesthetica: a comparative observational study of clinical presentation and morphological pathologies. Acta Derm Venereol 2018; 98: 82–88. https://doi.org/10.2340/00015555-2789
- Huesmann T, Cunha PR, Osada N, Huesmann M, Zanelato TP, Phan NQ, et al. Notalgia paraesthetica: a descriptive two-cohort study of 65 patients from Brazil and Germany. Acta Derm Venereol 2012; 92: 535–540. https://doi.org/10.2340/00015555-1344
- Klein PA, Clark RA. An evidence-based review of the efficacy of antihistamines in relieving pruritus in atopic dermatitis. Arch Dermatol 1999; 135: 1522–1525. https://doi.org/10.1001/archderm.135.12.1522