SHORT COMMUNICATION
Eye Movement Desensitization Protocol for Urge to Reduce Scratching Behaviour in Patients with Prurigo Nodularis: A Pilot Study
Mathijs R. DE VEER1,2, Leonieke W. KRANENBURG1, Tamar E. C. NIJSTEN2, Jan J. BUSSCHBACH1 and Rick WAALBOER-SPUIJ2
1Department of Psychiatry, Section Medical Psychology, and 2Department of Dermatology, Erasmus MC, University Medical Center Rotterdam, P.O. Box 2040, NL-3000 CA, Rotterdam, Netherlands. E-mail: m.deveer@erasmusmc.nl
Citation: Acta Derm Venereol 2024; 104: adv39945. DOI https://doi.org/10.2340/actadv.v104.39945.
Copyright: © 2024 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Jan 23, 2024. Accepted after revision: Apr 3, 2024. Published: May 2, 2024
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Prurigo nodularis (PN) shows the highest scores for itch intensity and frequency in dermatologic conditions (1). Scratching of the skin, as a response to the itch, is rewarding in the short term but may perpetuate the skin condition in the long run (2).
A significant amount of research is currently focused on developing new pharmaceutical treatments. Although preliminary studies are showing promising results, there remains a group of patients with persistent symptoms and scratching behaviour despite adequate treatment. Therefore it is crucial not to overlook or underestimate the added value of psychological interventions targeting scratching behaviour, which have shown substantial alleviation in both itching intensity and scratching (3). These interventions encompass self-control techniques, habit reversal, and self-monitoring of habitual behaviour, common components of effective cognitive-behavioural treatments, resulting in reduced frequency of the behaviour (4).
Recently, a novel type of psychological intervention, the Eye Movement Desensitization Protocol for Urge (EMD-U) (5), has proved effective in reducing the scratching behaviour of patients with atopic dermatitis (6).
Parallel to the itch–scratch cycle in atopic dermatitis, the scratching behaviour in patients with PN also deteriorates the skin condition. The hypothesis is that the rewarding impact of scratching exerts even more influence in patients with PN. Therefore, we aimed to investigate the effect of EMD-U in reducing the daytime scratching behaviour of patients with PN, additional to the standard dermatological treatment.
MATERIALS AND METHODS
Participants
Included were adult patients with a clinical diagnosis of prurigo nodularis (PN) with stable disease activity, who exhibit significant and persistent scratching behaviour and are motivated to actively engage in treatment. Patients were not allowed to change medications during the study period. If this proved necessary, the patient would be considered a dropout. The study was approved by the medical scientific research Ethical Committee of the Erasmus University Medical Center (reference number MEC-2023-0009).
Study design and intervention
Similar to the study in atopic dermatitis (AD) patients, the current pilot study applies a multiple baseline across subjects design (6,7). The study duration for all patients was 8 weeks, and consisted of 2 phases: baseline (pre-treatment) and post-treatment (Fig. S1). All patients started and ended with the registration of the scratching behaviour on the exact same day. Patients were randomly assigned to 1 of 5 weekdays in 1 of the 4 possible starting weeks (weeks 3 to 6), to start the intervention (8). In this way, the moment at which a patient starts the intervention is controlled and within- and between-subject comparisons can be made. Within 3 days after each session, patients were called by the psychologist.
Baseline. At the start of the study, patients were instructed regarding the registration of scratching behaviour, the T0 questionnaires were administered, and the disease activity was evaluated by a dermatologist. Patients had the mobile phone application for the registration of scratching behaviouur installed on their devices.
During the baseline period, patients did not yet receive treatment, but only registered their scratching behaviour.
Intervention and post-treatment. The intervention consisted of 2 EMD-U sessions of maximum 90 min in 2 consecutive weeks. In EMD-U, only the desensitization part of the full EMDR (Eye Movement Desensitization and Reprocessing) procedure is applied. The goal of desensitization is to “fade out” or “lose appetite” for the desired behaviour, in this case scratching (9). Patients are allowed to scratch in their imagination. At the same time, a distracting stimulus is presented. In addition, homework assignments and self-registration of the scratching behaviour are essential components of the treatment. As a homework assignment straight after the first session, patients were instructed and encouraged to practise the same intervention at home whenever they felt the urge to scratch. A detailed description of the protocol can be found in the previous article involving AD patients (6).
Measures
During the full 8 weeks, patients registered the frequency of their actual scratching behaviour. The registration was recorded on a mobile phone application designed for this study. In addition, multiple standardized measures were applied at the start and end of the study. Disease activity was measured with the Investigator Global Assessment (IGA) for stage of chronic nodular prurigo (CNPG) and signs of activity in chronic prurigo (10). Moreover, 2 quality-of-life measures were used: the SKINDEX-17, a dermatology-specific health-related quality of life (HRQOL) instrument (11); and the EQ-5D-5L, a generic QoL outcome measure (12). Finally, self-control (the Self-Control Cognition Questionnaire (in Dutch: Zelfcontrole Cognitie Vragenlijst [ZCCL] (13)) and sleep quality (the Pittsburgh Sleep Quality Index (PSQI) (14)) were queried.
Statistical analysis
Registration data of scratching behaviour was analysed using the web application Shiny SCDA (Single-Case Data Analysis; https://ppw.kuleuven.be/mesrg/software-and-apps/shiny-scda) (8,15). The nonoverlap of all pairs (NAP) effect size, an index of overlap of data between 2 phases in single-case research, is calculated using an expected decrease in scratching behaviour (16).
Standardized measures were presented as descriptives, given the small sample size in this multiple baseline study.
RESULTS
Five patients with prurigo nodularis completed the 8-week study period (mean age 61.8 years [SD 15.2]), 4 female). Patients 1, 2, and 6 used class 3 or 4 topical steroids with emollients. Patient 4 used narrowband UVB and patient 5 methotrexate 15 mg/week. There was no change in treatment during the study and patients showed insufficient improvement on standard dermatological treatment. One patient dropped out during the baseline phase as they experienced a sudden decrease in skin complaints and no longer considered the intervention necessary.
The course of the scratching behaviour of individual patients is shown in Fig. 1. The end of the baseline (A) and therefore the start of treatment (B) is indicated by the vertical dotted line. Except for patient 1, all other plots show a decrease in scratching behaviour over time. The horizontal dotted lines in Fig. 1 represent the average scratching frequency pre- and post-intervention.
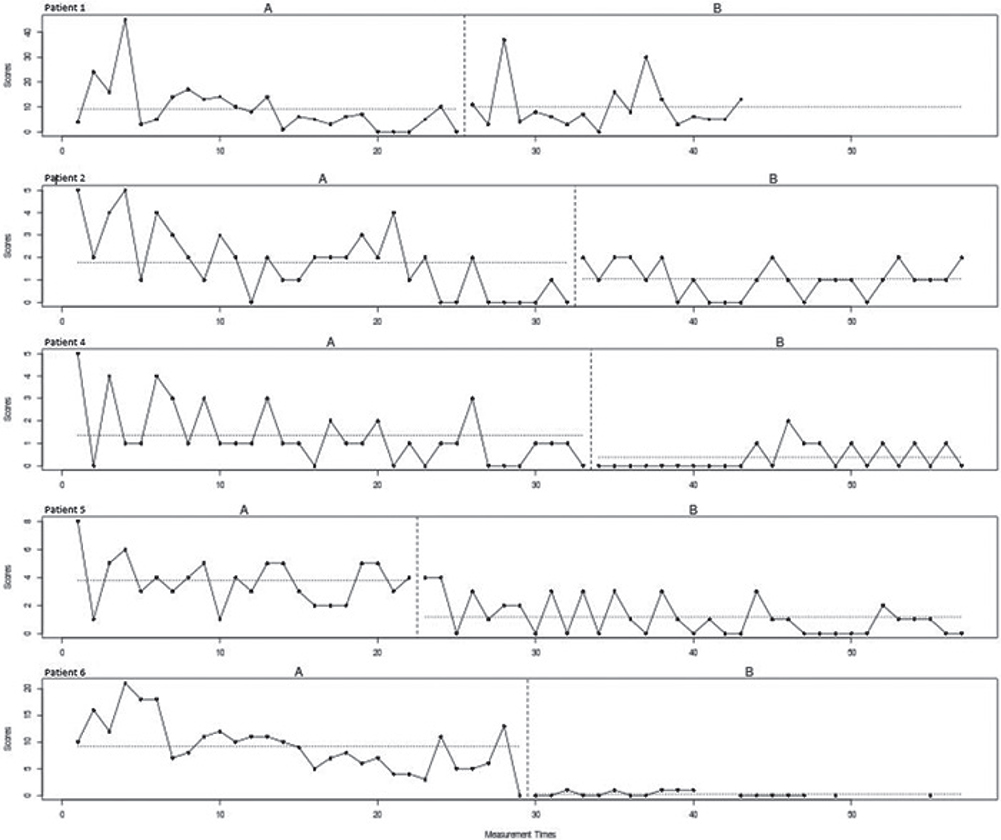
Fig. 1. Scratching behavior of individual patients over time for the baseline (A) and intervention (B) phase.
A NAP (non-overlap of all pairs) effect size of 0.75 was found, indicating a moderate treatment effect.
The exploratory analysis of disease activity, self-control, quality of life, and sleep quality are indicated in Table SI.
DISCUSSION
This multiple baseline study is the first to investigate the effect of the EMD-U in PN patients. The results show a moderate effect of the treatment on reducing scratching behaviour in addition to standard dermatological treatment. This effect is almost identical to the effect found in patients with AD (6). Again, an important observation is the improvement in scratching behaviour prior to the intervention. This occurrence has been documented in numerous pharmacological and behavioural studies before, yet its implications and even more intriguingly, how we can leverage it to our benefit in daily practice, must be the subject of further research (17). Improvement in health prior to the intervention could be attributed to factors such as self-monitoring and anticipatory effects (e.g. the optimistic expectations patients hold regarding the therapy).
Results of the EMD-U procedure both for PN and AD patients show promising evidence supporting the efficacy of this new method. In addition to a reduction in scratching frequency, improvements are observed in disease activity and self-control. Notably, there appears to be a positive impact on dermatology-specific quality of life as well. Nevertheless, further extensive research with a larger sample size is necessary to determine whether this intervention is a suitable method of enhancing the (dermatology-specific) quality of life for individuals experiencing frequent scratching behaviour. Moreover, in the current study we one used self-report data of scratching behaviour. Integrating actigraphs or similar tools could address this limitation, yet accurately capturing daytime scratching remains challenging due to difficulties in distinguishing it from other movements like playing the piano (18). Therefore, while alternative measurement methods offer potential solutions, they also pose their own challenges.
In conclusion, while considerable efforts and resources are mostly directed toward the development of pharmaceutical treatments for this impactful disease, it is imperative not to underestimate the contribution of additional psychological interventions addressing scratching behaviour. Although many patients benefit from pharmacological therapy, this unfortunately is not true for all. For these individuals, additional psychological interventions like EMD-U may play an important role in enhancing treatment effects. As we navigate the path to more effective solutions, a holistic approach that incorporates both pharmacological and psychological perspectives holds the key to cost-effective and enduring relief for those affected.
REFERENCES
- Steinke S, Zeidler C, Riepe C, Bruland P, Soto-Rey I, Storck M, et al. Humanistic burden of chronic pruritus in patients with inflammatory dermatoses: Results of the European Academy of Dermatology and Venereology Network on Assessment of Severity and Burden of Pruritus (PruNet) cross-sectional trial. J Am Acad Dermatol 2018; 79: 457–463.e5.
- Kwatra SG. Breaking the itch–scratch cycle in prurigo nodularis. Mass Medical Soc 2020; 3382: 757–758.
- Chida Y, Steptoe A, Hirakawa N, Sudo N, Kubo C. The effects of psychological intervention on atopic dermatitis. Int Arch Allergy Immunol 2007; 144: 1–9.
- Maas J, Hietbrink L, Rinck M, Keijsers GPJ. Changing automatic behavior through self-monitoring: does overt change also imply implicit change? J Behav Ther Exp Psychiatry 2013; 44: 279–284.
- Doeksen D, ten Broeke E. Too good to be true? Treatment of three patients with excessive scratching and tricotrillomania. EMDR Magazine 2009: p. 5–9.
- de Veer MR, Waalboer-Spuij R, Hijnen DJ, Doeksen D, Busschbach JJ, Kranenburg LW. Reducing scratching behavior in atopic dermatitis patients using the EMDR treatment protocol for urge: a pilot study. Front Med 2023; 10: 660.
- Morley S. Single case methods in clinical psychology: a practical guide: Routledge; 2017.
- De T, Michiels B, Vlaeyen J, Onghena P. Shiny SCDA. 2017.
- Markus W, Hornsveld HK, Burk WJ, de Weert-van Oene GH, Becker ES, DeJong CAJ. Addiction-focused eye movement desensitization and reprocessing therapy as an adjunct to regular outpatient treatment for alcohol use disorder: results from a randomized clinical trial. Alcohol Clin Exp Res 2020; 44: 272–283.
- Zeidler C, Pereira MP, Augustin M, Spellman M, Ständer S. Investigator’s global assessment of chronic prurigo: a new instrument for use in clinical trials. Acta Derm Venereol 2021; 101: adv00401.
- Nijsten TEC, Sampogna F, Chren M-M, Abeni DD. Testing and reducing skindex-29 using Rasch analysis: Skindex-17. J Invest Dermatol 2006; 126: 1244–1250.
- Janssen MF, Pickard AS, Golicki D, Gudex C, Niewada M, Scalone L, et al. Measurement properties of the EQ-5D-5L compared to the EQ-5D-3L across eight patient groups: a multi-country study. Qual Life Res 2013; 22: 1717–1727.
- Maas J, Keijsers GPJ, Cangliosi CM, van der Veld W, Tanis-Jacobs J, & Van Minnen A (2017). The Self-control Cognition Questionnaire: Cognitions in the maintenance of unwanted habits. Eur J Psychol Assess 2015; 33: 328–335.
- Buysse DJ, Reynolds Iii CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res 1989; 28: 193–213.
- Bulté I, Onghena P. The single-case data analysis package: analysing single-case experiments with R software. J Mod Appl Stat Methods 2013; 12: 28.
- Parker RI, Vannest K. An improved effect size for single-case research: nonoverlap of all pairs. Behav Ther 2009; 40: 357–367.
- Engelke M, Simões J, Vogel C, Schoisswohl S, Schecklmann M, Wölflick S, et al. Pilot study of a smartphone-based tinnitus therapy using structured counseling and sound therapy: a multiple-baseline design with ecological momentary assessment. PLOS Digit Health 2023; 2: e0000183.
- Yang AF, Nguyen M, Li AW, Lee B, San Chun K, Wu E, et al. Use of technology for the objective evaluation of scratching behavior: a systematic review. JAAD Int 2021; 5: 19–32.