REVIEW ARTICLE
Sex-related Variations in Comorbidities in Lichen Sclerosus: A Systematic Review and Meta-Analysis
Špela Šuler BAGLAMA1, Gregor B. E. JEMEC2,3, Jan ZMAZEK4 and Katarina TRČKO5
1Clinic of Dermatovenereology, University Medical Centre Ljubljana, Ljubljana, Slovenia, 2Department of Dermatology, Zealand University Hospital, Roskilde, Denmark, 3Department of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark, 4Department of Physics, Faculty of Natural Sciences and Mathematics, University of Maribor, Maribor, Slovenia, and 5Department of Dermatology and Venereal Diseases, University Medical Centre Maribor, Maribor, Slovenia
The comorbidities of lichen sclerosus (LS) are presumed but have not been analysed in detail. The purpose of this review was to identify evidence-based associated diseases in patients with LS and explore the potential need for sex-dependent screening protocols. A comprehensive search of the MEDLINE, Embase, and PsycINFO databases from inception to 29 February 2024 was conducted using the key search terms LS and all its synonyms. Pooled odds ratios and 95% confidence intervals of comorbidities were generated using the DerSimonian and Laird random-effects model. A total of 21 case-control studies met the inclusion criteria. Of the 75 comorbidities analysed, only 16 (21.3%) were studied in both sexes, revealing no contrasting associations based on sex. Both female and male LS patients showed significantly increased odds of common dermatological conditions (i.e., lichen planus, vitiligo, alopecia areata, atopic dermatitis, and psoriasis), various cardiovascular risk factors (i.e., essential hypertension, obesity, dyslipidaemia, diabetes mellitus, and diabetes mellitus type 2), genital warts, and hypothyroidism compared with controls. Overall, the scarcity of data currently does not support the implementation of sex-dependent screening strategies. The findings do, however, present significant associations with a range of potentially serious comorbidities, which warrants further elucidation and clinical vigilance.
Key words: comorbidities; lichen; sclerosus; sex; systematic review; meta-analysis.
SIGNIFICANCE
This study examines comorbidities and potential sex-based differences in lichen sclerosus (LS) across 21 case-control studies. Due to limited research, only a few comorbidities were common to both female and male LS patients, suggesting no distinct sex-based associations. This limited exploration discourages implementing sex-dependent screening strategies and underscores the importance of thorough skin examinations and regular screenings for cardiovascular risk factors and thyroid diseases in all LS patients to detect common comorbidities.
Citation: Acta Derm Venereol 2024; 104: adv39982. DOI https://doi.org/10.2340/actadv.v104.39982.
Copyright: © 2024 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Jan 27, 2024; Accepted after revision: Jul 15, 2024; Published: Aug 7, 2024
Corr: Špela Šuler Baglama, Clinic of Dermatovenereology, University Medical Centre Ljubljana, Gradiškova ulica 10, 1000 Ljubljana, Slovenia. E-mail: spela.baglama@gmail.com
Competing interests and funding: All authors declare no conflicts of interest in relation to this research.
INTRODUCTION
Lichen sclerosus (LS) is a chronic inflammatory skin condition that primarily affects the anogenital region and can occur at any age in individuals of both sexes with a female-to-male ratio between 3:1 and 10:1. There are indications of sex-specific differences in comorbidity occurrence in LS. However, these are poorly described (1). Therefore, the primary objective of this systematic review and meta-analysis was to comprehensively examine diseases associated with LS across both sexes, aiming to identify any sex-based discrepancies in comorbidity occurrence and advocate for potential sex-specific screening protocols. This examination of comorbidities in LS not only enhances care organization but also provides valuable insights into the underlying pathobiology of the disease.
MATERIALS AND METHODS
This systematic review was registered in PROSPERO (registration number CRD42022333520) and was performed according to the EQUATOR Reporting Guidelines. A comprehensive search of the MEDLINE, Embase, and PsycINFO databases from inception to 29 February 2024, was conducted through Ovid (https://www.wolterskluwer.com/en-gb/solutions/ovid) with the help of an experienced librarian using the key search terms lichen sclerosus and all its synonyms, later combined using OR to generate citations as can be seen in Appendix S1. All records retrieved by this search were screened for eligible studies independently by two authors (ŠŠB, KT) using Rayyan (https://www.rayyan.ai/). Any disagreement was discussed with a third author (GBEJ). After duplicate removal, titles and/or abstracts and, if necessary, full texts of the retrieved records were evaluated using the following inclusion criteria: (i) case-control study of comorbidities in LS written in English with at least 10 participants; (ii) comorbidities of LS, defined as any concurrent non-neoplastic diseases in individuals with LS, reported as absolute numbers or frequencies; (iii) the data disaggregated by sex; (iv) quality of the study, graded with the Newcastle-Ottawa Scale checklist at more than 3 stars (assessed by ŠŠB and KT). Later, the reference lists of relevant articles were additionally checked. Studies that reported outcomes regarding laboratory results rather than clinical diagnoses were excluded from the analysis. All authors agreed on the final studies for inclusion and, from each, data concerning authors, country, year of publication, study source, study population, sex, mean age, method of LS diagnosis, method of identification of comorbidities and comorbidities were extracted into an Excel sheet (Microsoft Corp, Redmond, WA, USA) (ŠŠB, KT).
All comorbidities associated with LS were compared with the control group, with separate analyses conducted for males and females, using odds ratios (OR) and 95% confidence intervals (CI). These OR and CI were calculated for each comorbidity using the DerSimonian and Laird random-effects model, which assigns more weight to studies with less variability and adjusts for additional variability across studies. Each study is weighted based on the inverse of its variance and a between-study variance component. Heterogeneity among the studies was evaluated using the I2 (%) statistic and the Q test (p-value) when a comorbidity had at least 3 included studies. Publication bias was evaluated through funnel plots and Egger’s test, with statistical significance set at a p-value < 0.05. All analyses were performed by custom Python scripts, using “statsmodels” and “scipy” libraries. The recommendations were graded by the Quality Rating Scheme for Studies and Other Evidence provided by the Oxford Centre for Evidence-Based Medicine.
RESULTS
Study selection and data synthesis
Initially, a total of 9,936 records were identified. After assessing the full texts of 198 articles for eligibility against all inclusion criteria, 21 case-control studies were ultimately included in the meta-analysis (2–22). PRISMA flow diagram can be seen in Fig. 1. Included studies collectively involved 13,765 females with LS and 21,702,053 females without it, as well as 1,589 males with LS and 8,900 non-LS male controls. Further details, such as the Newcastle-Ottawa quality of study assessment (Table SI), a summary of the key characteristics of the included studies (Table SII), and the PRISMA checklist (Table SIII), are available under Supplementary material. The diagnosis of LS was established through clinical examination, histological confirmation, or a combination of both methods in 17 studies, but the method was not clearly specified in the remaining 4. A total of 75 comorbidities were identified, but only 16/75 (21.3%) were studied in both sexes, while the remaining were investigated exclusively within 1 sex. All meta-analysis results are presented in Fig. 2, with comorbidities examined in both sexes highlighted in Fig. 3. Only significant findings common to both sexes are listed in the results section. Assessment of heterogeneity and publication bias including the Q statistic, I², and p-value of Egger’s test are presented in Table SIV (for women) and Table SV (for men). The included studies employed diverse terminology for defining certain diseases, rendering their data integration challenging, but we made concerted efforts to merge them coherently.

Fig. 1. PRISMA flow diagram illustrating the selection process of studies included in the meta-analysis.
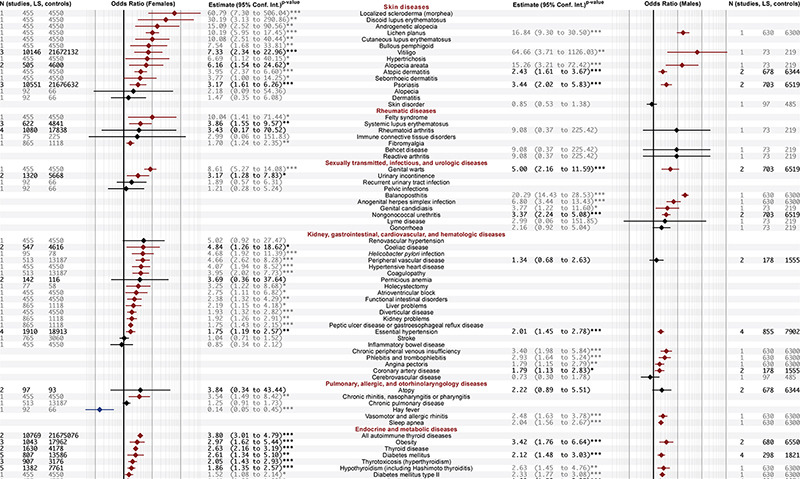
Fig. 2. Forest plot displaying pooled odds ratios and 95% confidence intervals for comorbidities associated with lichen sclerosus, separated by sex. Significant ORs greater than 1 are shown in red, significant ORs less than 1 are shown in blue, and non-significant ORs are shown in black. Numbers and estimates that rely on data from more than 1 study are emphasized, indicating stronger evidence. Legend: N: number, OR: odds ratio, *p < 0.05, **p < 0.01, ***p < 0.001.
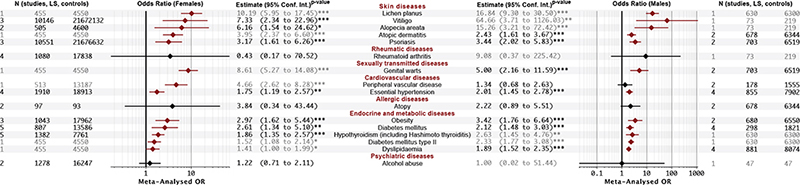
Fig. 3. Forest plot highlighting pooled odds ratios and 95% confidence intervals for comorbidities associated with lichen sclerosus, analysed across both sexes. Significant ORs greater than 1 are shown in red, and non-significant ORs are shown in black. Numbers and estimates that rely on data from more than 1 study are emphasized, indicating stronger evidence. Legend: N: number, OR: odds ratio, *p < 0.05, **p < 0.01, ***p < 0.001.
Skin diseases
Both female and male LS patients exhibited significantly elevated odds of developing lichen planus (females, OR = 10.19, 95% CI = 5.95–17.45; males, OR = 16.84, 95% CI = 9.30–30.50), vitiligo (females, OR = 7.33, 95% CI = 2.34–22.96; males, OR = 64.66, 95% CI = 3.71–1126.03), alopecia areata (females, OR = 6.16, 95% CI = 1.54–24.62; males, OR = 15.26; 95% CI = 3.21–72.42), atopic dermatitis (females, OR = 3.95, 95% CI = 2.37–6.60; males, OR = 2.43, 95% CI = 1.61–3.67), and psoriasis (females, OR = 3.17, 95% CI = 1.61–6.26; males, OR = 3.44, 95% CI = 2.02–5.83) compared with non-LS controls.
Sexually transmitted diseases
Both female and male LS patients showed significantly increased odds of having genital warts (females, OR = 8.61, 95% CI = 5.27–14.08; males, OR = 5.00, 95% CI = 2.16–11.59) compared with non-LS controls.
Cardiovascular diseases
Both female and male LS patients exhibited significantly elevated odds of developing essential hypertension (females, OR = 1.75, 95% CI = 1.19–2.57; males, OR = 2.01, 95% CI = 1.45–2.78) compared with non-LS controls.
Endocrine and metabolic diseases
Significantly higher odds were observed in both sexes with LS compared with the non-LS control group for obesity (females, OR = 2.97, 95% CI = 1.62–5.44; males, OR = 3.42, 95% CI = 1.76–6.64), diabetes mellitus (females, OR = 2.61, 95% CI = 1.34–5.10; males, OR = 2.12, 95% CI = 1.48–3.03), diabetes mellitus type 2 (females, OR = 1.52, 95% CI = 1.08–2.14; males, OR = 2.33, 95% CI = 1.77–3.08), hypothyroidism (including Hashimoto thyroiditis; females, OR = 1.86, 95% CI = 1.35–2.57; males, OR = 2.63, 95% CI = 1.45–4.76), and dyslipidaemia (females, OR = 1.41, 95% CI = 1.00–1.99; males, OR = 1.89, 95% CI = 1.52–2.35).
DISCUSSION
This systematic review indicates that a broad range of diseases may be associated with LS. Both female and male LS patients showed significantly increased odds of common dermatological conditions (i.e., lichen planus, vitiligo, alopecia areata, atopic dermatitis, and psoriasis), various cardiovascular risk factors (i.e., essential hypertension, obesity, dyslipidaemia, diabetes mellitus, and diabetes mellitus type 2), genital warts, and hypothyroidism, including Hashimoto thyroiditis compared with non-LS controls. The subsequent exploration of potential different screening protocols for LS comorbidities based on sex found no contrasting associations between men and women, highlighting that certain health risks are similar for both sexes. Due to selection bias, where 13 out of 21 case-control studies focused on female comorbidities, male comorbidities were largely unexplored. This may explain the perceived sex-dependent difference in comorbidities in LS, emphasizing the need to prioritize and intensify research efforts towards understanding comorbidities in male LS patients (1).
As additional diseases were not investigated in both sexes, a direct analysis of further comorbidities in LS based on sex is limited. By focusing on associations examined in more than 1 study, which increases statistical power despite being restricted to 1 sex, females with LS additionally showed significant associations with systemic lupus erythematosus, urinary incontinence, coeliac disease, depression, and other thyroid diseases, while males with LS were significantly associated with nongonococcal urethritis and coronary artery disease. Further evidence from individual studies corroborated the association of LS with diverse cardiovascular conditions in both sexes and additional genital infections in males with LS.
While some associated diseases in LS may be incidental (e.g., genital infections and skin diseases found due to surveillance bias) or the result of a previous incorrect diagnosis carried forward (e.g., lichen planus in classification bias), they nevertheless represent a clinically relevant catalogue (see Fig. 2 for all results). It is suggested that these diseases are brought to clinicians’ attention when doing a work-up of LS patients. Our findings especially suggest the need for thorough skin examinations and regular screenings for cardiovascular risk factors and thyroid diseases in all LS patients to detect common comorbidities.
Finally, understanding comorbid diseases provides valuable insights into the complex nature of LS. For example, comorbid autoimmune diseases may contribute to the diminished suppressive function of regulatory T cells, triggering an immune response against extracellular matrix self-antigens observed in LS (23–27). Additionally, cardiovascular risk factors and diseases may exacerbate endothelial dysfunction and decrease microvascular density in LS tissue (28, 29).
Limitations
In addition to selection and potential surveillance and classification biases, this study has several other limitations. First, while all cases and controls were sex-matched, only 15/21 studies were additionally age-matched, leading to potential bias in reporting comorbidity frequencies. Additionally, race was matched in only 6/21 studies, while socioeconomic status was not standardized. If any of these factors are independently associated with LS and were not evenly distributed among groups, this could potentially affect the results. Moreover, the majority (13/21) of controls originated from the same institution but were diagnosed with conditions other than LS. The control group came from the community in only in 2 studies, while others were sourced from various health facilities or insurance company databases. This may not accurately represent the overall population. Next, in 17/21 studies, LS was confirmed either histologically or clinically, while in 4 studies the method of confirmation was not specified. Conversely, only 1 study excluded LS histologically in the control group, and in 10/21 studies the exclusion method was not specified. This lack of specification raises concerns that subclinical LS diagnoses may have been missed in the control group, potentially introducing bias into the results. Additionally, data reliance on various sources such as International Classification of Diseases codes (7/19), chart reviews (6/19), questionnaires/interviews (7/19), and/or clinical examination/other tests (4/19) may have led to the omission of unrecognized comorbidities, recall bias, or underreporting due to coding errors. What is more, the increased occurrence of comorbidities in LS might stem from frequent doctor’s visits prompted by these conditions rather than direct associations with LS, or LS may be more readily diagnosed when patients seek medical attention for other reasons. Conversely, individuals who avoid seeking medical advice may not be accurately represented in medical records. It is also possible that patients with LS who seek medical attention may have a higher disease burden and, thus, more comorbidities. Additionally, sex-related medical help-seeking behaviours may contribute to the underreporting of certain medical conditions.
Despite our efforts to limit heterogeneity in this meta-analysis, heterogeneity remained considerable for hypothyroidism (including Hashimoto thyroiditis), psoriasis, essential hypertension, vitiligo, and obesity in females and essential hypertension in males. On the other hand, the p-values of Egger’s test were far above the significant threshold of 0.05, indicating a low likelihood of publication bias in the meta-analysis results. However, with only a small number of available studies that were included in the meta-analysis, the ability to explore and explain heterogeneity and publication bias is limited. The rating of quality of evidence for this meta-analysis is categorized as Grade 3a, according to the Quality Rating Scheme for Studies and Other Evidence provided by the Oxford Centre for Evidence-Based Medicine, as it combines data from case-control studies.
Conclusion
Our meta-analysis underscores the significant association between LS and various skin, sexually transmitted, cardiovascular, metabolic, and endocrine diseases in both males and females. It is suggested that these diseases are brought to clinicians’ attention when doing a work-up of LS patients. In practical terms, the findings of this study indicate the need to conduct thorough skin examinations and routinely screen all LS patients for cardiovascular risk factors and thyroid diseases to identify common comorbidities. However, further prospective case-control studies are needed to validate the findings of this meta-analysis and to enhance our understanding of the complex comorbidities associated with LS.
ACKNOWLEDGEMENTS
Disclosures: The meta-analysis was conducted without financial support or funding disclosures.
Ethics statement: This review article does not involve the collection, analysis, or reporting of original data involving human subjects, animals, or any sensitive information. As such, ethical approval and formal consent were not deemed necessary for this review, in accordance with the guidelines and regulations of the National Medical Ethics Committee of the Republic of Slovenia. The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki.
Data availability statement: The datasets generated and/or analysed during the current study are available upon request to the corresponding author.
REFERENCES
- Kirtschig G, Kinberger M, Kreuter A, Simpson R, Günthert A, van Hees C, et al. EuroGuiDerm guideline on lichen sclerosus [Internet]. 2023 [cited 2024 May 19]. Available from: https://www.guidelines.edf.one//uploads/attachments/clmub3q4l0an5uhjrluc4r0yq-lichen-sclerosus-gl.pdf.
- Harrington CI, Dunsmore IR. An investigation into the incidence of auto-immune disorders in patients with lichen sclerosus and atrophicus. Br J Dermatol 1981; 104: 563–566. https://doi.org/10.1111/j.1365-2133.1981.tb08172.x
- Sideri M, Parazzini F, Rognoni MT, La Vecchia C, Negri E, Garsia S, et al. Risk factors for vulvar lichen sclerosus. Am J Obstet Gynecol 1989; 161: 38–42. https://doi.org/10.1016/0002-9378(89)90228-7
- Meeks J, Qi T, Cashy J, Yang X, Gonzalez C. 849 Role of testosterone in the pathogenesis and treatment of lichen sclerosus. J Urol 2010; 183: e331. https://doi.org/10.1016/j.juro.2010.02.2351
- Bjekić M, Šipetić S, Marinković J. Risk factors for genital lichen sclerosus in men. Br J Dermatol 2011; 164: 325-329. https://doi.org/10.1111/j.1365-2133.2010.10091.x
- Higgins CA, Cruickshank ME. A population-based case-control study of aetiological factors associated with vulval lichen sclerosus. J Obstet Gynaecol 2012; 32: 271–275. https://doi.org/10.3109/01443615.2011.649320
- Becker K, Meissner V, Farwick W, Bauer R, Gaiser MR. Lichen sclerosus and atopy in boys: coincidence or correlation? Br J Dermatol 2013; 168: 362–366. https://doi.org/10.1111/j.1365-2133.2012.11201.x
- Hofer MD, Meeks JJ, Mehdiratta N, Granieri MA, Cashy J, Gonzalez CM. Lichen sclerosus in men is associated with elevated body mass index, diabetes mellitus, coronary artery disease and smoking. World J Urol 2014; 32: 105–108. https://doi.org/10.1007/s00345-013-1090-7
- Blaschko SD, Gaither TW, Alwaal A, Harris CR, McCulloch CE, McAninch JW, et al. Lichen sclerosus comorbidities and complications from a national sample of patients treated with urethroplasty. Urol Pract 2015; 2: 329–334. https://doi.org/10.1016/j.urpr.2015.02.006
- Erickson BA, Elliott SP, Myers JB, Voelzke BB, Smith TG 3rd, McClung CD, et al. Understanding the Relationship between chronic systemic disease and lichen sclerosus urethral strictures. J Urol 2016; 195: 363–368. https://doi.org/10.1016/j.juro.2015.08.096
- Fuchs ME, Beecroft N, Dajusta DG, McLeod DJ. The association between BXO and obesity in boys undergoing circumcision. Glob Pediatr Health 2017; 4: 2333794X17742749. https://doi.org/10.1177/2333794X17742749
- Basile S, Pinelli S, Benedetti Panici P, Angioli R, Plotti F, Giannarelli D, et al. Association between Helicobacter pylori infection and vulvar lichen sclerosus: a clinical comparative study. Eur J Dermatol 2018; 28: 226–227. https://doi.org/10.1684/ejd.2017.3207
- Hu J, Hesson A, Haefner HK, Rominski S. The prevalence of self-reported medical comorbidities in patients with vulvar lichen sclerosus: a single-center retrospective study. Int J Gynaecol Obstet 2021; 153: 340–343. https://doi.org/10.1002/ijgo.13480
- Bieber AK, Steuer AB, Melnick LE, Wong PW, Pomeranz MK. Autoimmune and dermatologic conditions associated with lichen sclerosus. J Am Acad Dermatol 2021; 85: 228–229. https://doi.org/10.1016/j.jaad.2020.08.011
- Hieta N, Rintala M, Söderlund JM, Samu K, Orte K, Hietanen S. Comorbidity of dermal and cardiovascular disorders with lichen sclerosus: a case-control study. Acta Derm Venereol 2021; 101: adv00594. https://doi.org/10.2340/actadv.v101.433
- Nizinski K, Orszulak D, Janik M, Skowronek K, Stojko R, Drosdzol-Cop A. The analysis of coexistence of celiac disease and vulvar lichen sclerosus in girls. Ginekol Pol 2022; 93: 793–798. https://doi.org/10.5603/GP.a2022.0102
- Fan R, Leasure AC, Maisha FI, Little AJ, Cohen JM. Depression and anxiety in patients with lichen sclerosus. JAMA Dermatol 2022; 158: 953–954. https://doi.org/10.1001/jamadermatol.2022.1964
- Fan R, Leasure AC, Maisha FI, Cohen JM, Little AJ. Thyroid disorders associated with lichen sclerosus: a case-control study in the All of Us Research Program. Br J Dermatol 2022; 187: 797–799. https://doi.org/10.1111/bjd.21702
- Hieta NK, Haataja MAM, Tapana L. Comorbidities in male patients with lichen sclerosus: a case-control study. J Low Genit Tract Dis 2023; 27: 378–383. https://doi.org/10.1097/LGT.0000000000000769
- El Khoury J, Andraos J, Kanbar A, Halabi R, Assaf S, Mina A, et al. A potential protective effect of alcohol consumption in male genital lichen sclerosus: a case-control study. Adv Urol 2023; 2023: 7208312. https://doi.org/10.1155/2023/7208312
- Söderlund JM, Hieta NK, Kurki SH, Orte KJ, Polo-Kantola P, Hietanen SH, et al. Comorbidity of urogynecological and gastrointestinal disorders in female patients with lichen sclerosus. J Low Genit Tract Dis 2023; 27: 156–160. https://doi.org/10.1097/LGT.0000000000000727
- Luu Y, Cheng AL, Reisz C. Elevated body mass index, statin use, and cholecystectomy are associated with vulvar lichen sclerosus: a retrospective, case-control study. J Am Acad Dermatol 2023; 88: 1376-1378. https://doi.org/10.1016/j.jaad.2023.01.023
- Chan I. The role of extracellular matrix protein 1 in human skin. Clin Exp Dermatol 2004; 29: 52–56. https://doi.org/10.1111/j.1365-2230.2004.01440.x
- Chan I, Oyama N, Neill SM, Wojnarowska F, Black MM, McGrath JA. Characterization of IgG autoantibodies to extracellular matrix protein 1 in lichen sclerosus. Clin Exp Dermatol 2004; 29: 499–504. https://doi.org/10.1111/j.1365-2230.2004.01573.x
- Sander CS, Ali I, Dean D, Thiele JJ, Wojnarowska F. Oxidative stress is implicated in the pathogenesis of lichen sclerosus. Br J Dermatol 2004; 151: 627–635. https://doi.org/10.1111/j.1365-2133.2004.06142.x
- Gambichler T, Belz D, Terras S, Kreuter A. Humoral and cell-mediated autoimmunity in lichen sclerosus. Br J Dermatol 2013; 169: 183–184. https://doi.org/10.1111/bjd.12220
- Wang L, Yi JL, Chen HY, Wang PL, Shen YL. Level of Foxp3, DNMTs, methylation of Foxp3 promoter region, and CD4 + CD25 + CD127low regulatory T cells in vulvar lichen sclerosus. Kaohsiung J Med Sci 2021; 37: 520–527. https://doi.org/10.1002/kjm2.12356
- Li YZ, Wu Y, Zhang QH, Wang Y, Zhen JH, Li SL. Hypoxia-ischaemia is involved in the pathogenesis of vulvar lichen sclerosus. Clin Exp Dermatol 2009; 34: e531–536. https://doi.org/10.1111/j.1365-2230.2009.03571.x
- Saravanamuthu J, Reid WM, George DS, Crow JC, Rolfe KJ, MacLean AB, et al. The role of angiogenesis in vulvar cancer, vulvar intraepithelial neoplasia, and vulvar lichen sclerosus as determined by microvessel density analysis. Gynecol Oncol 2003; 89: 251–258. https://doi.org/10.1016/S0090-8258(03)00055-6