REVIEW ARTICLE
Immunogenicity, Effectiveness, and Safety of COVID-19 Vaccines among Patients with Immune-Mediated Dermatological Diseases: A Systematic Review and Meta-analysis
Sonphet CHIRASUTHAT1, Yanisa RATANAPOKASATIT1, Kunlawat THADANIPON1,2 and Kumutnart CHANPRAPAPH1
1Division of Dermatology, Department of Medicine, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand, and 2Department of Clinical Epidemiology and Biostatistics, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Immunocompromised individuals, primarily attributable to using immunosuppressants, face heightened COVID-19 risks. Despite the proven efficacy of COVID-19 vaccines, their impact on patients with immune-mediated dermatological diseases remains unclear. This study aims to thoroughly examine vaccine immunogenicity, effectiveness, and safety in immune-mediated dermatological disease patients. Clinical studies in adults that compared vaccinated immune-mediated dermatological disease patients with vaccinated healthy controls or unvaccinated immune-mediated dermatological disease patients in terms of vaccine immunogenicity, COVID-19 infection, adverse events, or exacerbation of immune-mediated dermatological diseases were searched via electronic databases. Seventeen studies (1,348,690 participants) were included. Seroconversion rates between immune-mediated dermatological disease patients and healthy controls were not different. However, among individuals aged ≤55 years, immune-mediated dermatological disease patients had lower mean anti-SARS-CoV-2 IgG levels. Immunosuppressed immune-mediated dermatological disease patients also had lower titres and were less likely to achieve T-cell response. In terms of safety, the risk of adverse events was higher in atopic dermatitis patients, but those with psoriasis had a reduced risk. Additionally, immunosuppressed patients had fewer adverse events. Vaccinated immune-mediated dermatological disease patients had a lower risk of COVID-19 infection than unvaccinated patients but a higher risk than healthy controls; however, disease exacerbation may be induced. In conclusion, immune-mediated dermatological diseases showed a reduced vaccine response in our meta-analysis, yet vaccination remained effective against COVID-19 infection and well tolerated.
SIGNIFICANCE
The lack of clarity on specific immunogenicity in patients with immune-mediated dermatological diseases despite their elevated risk of COVID-19 infection led to this study where a comprehensive review and analysis of vaccine effectiveness and safety was performed in this population, comparing the outcomes with healthy controls and unvaccinated immune-mediated dermatological diseases. The study found that while immune-mediated dermatological disease patients show a comparable overall immune response to COVID-19 vaccination as healthy controls, they have a lower risk of breakthrough infections and hospitalization than unvaccinated immune-mediated dermatological diseases. Vaccination appears to be effective and well-tolerated in preventing COVID-19 infection in immune-mediated dermatological disease patients.
Key words: COVID-19 vaccines; immune system diseases; immunosuppression therapy; meta-analysis; skin diseases.
Citation: Acta Derm Venereol 2024; 104: adv40009. DOI https://doi.org/10.2340/actadv.v104.40009.
Copyright: © 2024 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Jan 30, 2024. Accepted after revision: Apr 9, 2024. Published: May 2, 2024
Corr: Kumutnart Chanprapaph, Division of Dermatology, Department of Medicine, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand. E-mail: kumutnartp@hotmail.com
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Since the start of the current COVID-19 epidemic, attempts have been made globally to produce SARS-CoV-2 vaccines as vaccination is one of the most important preventive measures to keep infectious diseases under control. In addition to preventing the transmission of the virus, vaccination against COVID-19 will help reduce the risk of severe COVID-19 and its complications (1). There have been multiple randomized controlled trials and meta-analyses proving the efficacy and safety of various types of COVID-19 vaccines (2–6). Immunocompromised patients are at a higher risk of COVID-19 infection (7,8). Not only has this group of patients experienced more severe and persistent infections, but there have also been reports of prolonged viral shedding, which has led to current recommendations for immunocompromised patients to receive COVID-19 vaccine (9–11). However, due to the use of immunosuppressants and the disease itself, these patients appear to have lower immunogenicity, such as a lower rate of seroconversion after the vaccination. Current studies have included and summarized the efficacy and safety of the vaccine in patients with various immunocompromised conditions (e.g. organ transplant, cancer, rheumatic diseases, and chronic inflammatory bowel diseases) (12–18). Nevertheless, there is no clear conclusion from studies conducted in patients with immune-mediated dermatological diseases (IMDDs). Vaccine types, immunosuppressant class and dosage, and the disease itself are among the many factors that could affect the efficacy and safety of COVID-19 vaccines in this group of patients. Thus, data associated with COVID-19 vaccines among IMDD patients are necessary to justify the risks and benefits of the COVID-19 vaccination to perhaps prepare ourselves for the next pandemic. This study aims to investigate the immunogenicity, effectiveness, and safety of COVID-19 vaccines among IMDD patients compared with healthy controls (HCs) and unvaccinated IMDD patients through a systematic review and meta-analysis.
MATERIALS AND METHODS
Definitions
IMDDs in this study included but were not limited to autoimmune bullous diseases (AIBDs), psoriasis, atopic dermatitis (AD), chronic spontaneous urticaria (CSU), and cutaneous lupus erythematosus (CLE) that were diagnosed by dermatologists. COVID-19 vaccination was defined as receiving at least one dose of any type or brand of COVID-19 vaccine. Patients using different COVID-19 vaccine platforms was known as heterogeneous vaccination. Immunogenicity of COVID-19 vaccines comprised both humoral, including the production of antibodies such as neutralizing antibodies, and cellular immune responses, which involve the activation of T cells and other components of the cellular immune system. A change from negative to positive specific IgG antibodies was referred to as seroconversion. The effectiveness of a COVID-19 vaccine was assessed by evaluating its impact on the incidence and severity of COVID-19 infection, encompassing asymptomatic COVID-19, symptomatic COVID-19, COVID-19-associated hospitalization, COVID-19 requiring intensive care, and mortality. The safety of a COVID-19 vaccine was defined based on the number (i.e. local and systemic) and severity (minor to serious, including hospitalization, prolonged hospitalization, persistent disability, life-threatening events, and death) of adverse events (AEs) using the WHO guidelines. Additionally, exacerbation of IMDDs, characterized by the worsening of the diseases, was evaluated with consideration for severity index changes, which may or may not be identified. The exacerbation of IMDDs also included morphologic changes (e.g. transition from chronic plaque-type to guttate, pustular, or erythrodermic psoriasis) observed after vaccination. This assessment incorporated patient self-reports and physicians’ diagnoses. Immunosuppressed patients in this study were defined as those taking systemic drugs with immunosuppressive or immunomodulatory properties.
Search strategy
This systematic review and meta-analysis was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (19). The protocol of this study was registered on PROSPERO (CRD42022356088). Electronic databases, including PubMed-MEDLINE, Scopus, and Embase, were searched for eligible articles published in November 2022. The detailed search strategy is shown in Table SI. The references of the selected articles were further searched manually. There was no restriction on geography or language of publication.
Study selection
We intended to include either experimental or observational comparative studies between adult IMDD patients and HCs who both received COVID-19 vaccines, or between vaccinated and unvaccinated adult IMDD patients, with any of the following outcomes: immunogenicity of COVID-19 vaccines, COVID-19 infection and its severity, AEs, and exacerbation of IMDDs. Studies lacking full-text articles were excluded. Two reviewers (SC and YR) independently screened each title and abstract for eligibility and reviewed the full-text article when a decision could not be made from the title and abstract. If necessary, abstracts and manuscripts published in languages other than English were translated. Disparities were resolved through consensus among the reviewer team.
Data extraction
Data from the selected articles were extracted via a data extraction form by two independent reviewers (SC and YR). Data on study characteristics comprised bibliographic information, setting, study design, follow-up time, inclusion, and exclusion criteria. The number of participants, characteristics of the control group, ethnicity, age, sex, type of IMDDs, severity and disease duration, treatment for IMDDs including immunosuppressive regimens, comorbidity, and relevant laboratory data were all part of the participant data. COVID-19 vaccine data included vaccine brands and types, number of doses, and interval between doses. The outcomes data encompassed the number of participants exhibiting seroconversion and/or T-cell response, the mean, standard deviation, median, and interquartile range of antibody levels, the incidence of COVID-19 infection and its severity, as well as the occurrence of AEs, its type and severity and/or exacerbation of IMDDs. Outcome-related data comprised the types and measures of outcomes evaluated in the study, the method of evaluation, and interval from vaccination to blood sampling evaluation.
Study quality assessment
Quality of the eligible studies was assessed independently by the same reviewers. The assessment of studies comparing vaccinated IMDD patients with vaccinated HCs was conducted using the Newcastle-Ottawa Scale (NOS), as the study factor (i.e. IMDDs) does not represent an intervention. NOS is classified into 3 categories: low (≥ 7 stars), moderate (5–6 stars), and high risk of bias (≤ 4 stars) with a 9-star rating for overall quality (20). Meanwhile, studies that compared vaccinated and unvaccinated IMDD patients were assessed by using the Risk Of Bias In Non-randomized Studies – of Interventions (ROBINS-I) tool (21). This tool includes 7 domains, and a judgement is assigned for each domain as low, moderate, serious, and critical risk of bias.
Statistical analysis
Meta-analysis was performed to pool risk ratios (RR) and mean differences of the outcomes. If the mean and standard deviation of continuous outcomes were not available, they were estimated from the sample size, median, and interquartile range by using a method proposed by Wan et al. (22). To pool the mean differences in anti-SARS-CoV-2 IgG antibody titres, the titres in arbitrary units/mL (AU/mL) or units/mL (U/mL) from different manufacturers were converted to binding antibody units/mL (BAU/mL), a universal immunological unit, by using standardized conversion factors recommended by the WHO international standard for anti-SARS-CoV-2 immunoglobulin (23), as indicated in Table SII. Random-effects models with the DerSimonian–Laird method were used to pool estimates in the presence of heterogeneity, i.e. Higgin’s I2 ≥25% or p-value of Cochrane’s Q test <0.1. Otherwise, fixed-effect models with the inverse-variance method were used. When data were available, subgroup analysis was performed to investigate the possible source of heterogeneity by using study design, mean age, COVID-19 vaccine type, number of vaccine doses, vaccination-to-blood sampling interval, IMDDs, type of immunosuppressants, and use of biologic drugs. The studies were subdivided based on the characteristics indicated by the majority of participants (i.e. >50% of participants in the studies). Publication bias was assessed visually by inspecting the funnel plots and contour-enhanced funnel plots. Statistical analyses were performed with Stata 16.0 (StataCorp LLC, College Station, TX, USA). Two-sided p-values of <0.05 were considered statistically significant.
RESULTS
Study characteristic
Our search identified a total of 1,533 articles after removing duplicates. Then, 1,336 articles were excluded after screening of titles and abstracts. A total of 197 articles were assessed for eligibility through full-text review. Finally, 17 eligible studies, comprising 1,348,067 participants, were included. All of these were observational, with the cohort study design. Among them, 13 studies compared vaccinated IMDD patients with vaccinated HCs, while 4 studies examined the comparison between vaccinated and unvaccinated IMDD patients. The process is demonstrated in the PRISMA flow diagram (Fig. S1). Eleven studies had low risk of bias, five had moderate risk, and one had high risk (Table SIII and Table SIV). Of these studies, 12 included patients with psoriasis, 5 with AD, 5 with AIBD, 3 with CSU, and 1 with CLE. COVID-19 vaccine administered in the studies included mRNA vaccines (Pfizer-BioNTech, BNT162b2 and Moderna, mRNA-1273), recombinant viral vector vaccines (Oxford-AstraZeneca, AZD1222; Janssen, Ad26.COV2.S; and Gamaleya, Sputnik V), inactivated vaccines (Sinopharm, BBIBP-CorV and Sinovac, Coronavac), and heterogeneous vaccines. There were no studies of protein subunit vaccine users that were eligible. One study was excluded from the quantitative analysis due to the use of geometric mean concentration of anti-SARS-CoV-2 spike protein IgG as a representative of the immune response (24). Table I summarizes characteristics of the included studies. Tables II and III present the pooled effect sizes on outcomes of interest in vaccinated IMDD patients compared with vaccinated HCs and unvaccinated patients, respectively.
| Author (year) | Country | Study design | Participants, n | Type of vaccine(s) | Type of IMDD(s) | Treatment(s) for IMDDs | Seroconversion threshold |
| Boekel (2022) (57) | Netherland | Prospective cohort | 381 IMDDs, 822 HCs | BNT162b2, mRNA-1273, AZD1222, Ad26.COV2.S, heterogeneous vaccine | AD, psoriasis, pemphigus, vitiligo, and others | MTX, MMF, TNFi, anti-CD20, or other immunosuppressants | Anti-RBD IgG ≥4.0 AU/mL |
| Stalman (2022) (58) | Netherland | Prospective cohort | 288 IMDDs, 161 HCs | BNT162b2, mRNA-1273, AZD1222, Ad26.COV2.S | AD, psoriasis, pemphigus, vitiligo, and others | MTX, MMF, TNFi, anti-CD20, and other immunosuppressants | Anti-RBD IgG ≥4.0 AU/mL |
| Cao (2022) (59) | China | Retrospective cohort | 37 IMDDs, 1,545 HCs | BBIBP-CorV, Coronavac | AD | Not identified | - |
| Chanprapaph (2022) (32) | Thailand | Prospective cohort | 127 IMDDs, 97 HCs | AZD1222 | Psoriasis, pemphigus, pemphigoid, CSU, CLE | Prednisolone, cyclosporine, MTX, AZA, MMF, secukinumab, ixekizumab, guselkumab, ustekinumab, omalizumab, etanercept, and rituximab | Surrogate viral neutralization tests > 5% (wild-type strain) and > 0% inhibition (delta variant) |
| Cristaudo (2022) (33) | Italy | Prospective cohort | 48 IMDDs, 48 HCs | BNT162b2 | Psoriasis | TNFi, IL-12/23i, IL-17i, IL-23i, and infliximab + MTX | - |
| Özgen (2022) (26) | Turkey | Retrospective cohort | 175 IMDDs, 69 HCs | BNT162b2, AZD1222, Coronavac | Pemphigus vulgaris, pemphigus foliaceus | Systemic corticosteroids, MTX, MMF, AZA, dapsone, and rituximab | - |
| Mahil (2021) (27) | England | Prospective cohort | 67 IMDDs, 15 HCs | BNT162b2 | Psoriasis | MTX, TNFi, IL-17i, and IL-23i | EC50 of anti-SARS-CoV-2 IgG titres ≥25 |
| Mahil (2021) (28) | England | Prospective cohort | 84 IMDDs, 17 HCs | BNT162b2 | Psoriasis | MTX, TNFi, IL-17i, and IL-23i | EC50 of anti-SARS-CoV-2 IgG titres ≥25 |
| Megna (2022) (37) | Italy | Prospective cohort | 44 IMDDs, 57 HCs | BNT162b2, mRNA-1273 | Psoriasis | TNFi, IL-12/23i, IL-17i, and IL-23i | IgG antibodies to COVID-19 protein spike ≥50 BAU/mL |
| Pakhchanian (2022) (29) | USA | Retrospective cohort | 15,306 IMDDs, 1,247,000 HCs | BNT162b2, mRNA-1273, Ad26.COV2.S | AD | Immunosuppressants/immunomodulatory therapy | - |
| Parlotsky (2022) (35) | Israel | Prospective cohort | 51 IMDDs, 3,306 HCs | BNT162b2 | Psoriasis | MTX, TNFi, ustekinumab, IL-17i, or IL-23i | Anti-RBD IgG ≥1 S/mL or ≥150 AU/mL, antibodies neutralization activity ≥30% inhibition |
| Piros (2022) (60) | Hungary | Prospective cohort | 102 IMDDs, 55 HCs | BNT162b2, mRNA-1273 | Psoriasis | TNFi, IL-17i, IL-23i, or IL-12/23i | - |
| Seree-aphinan (2021) (36) | Thailand | Prospective cohort | 14 IMDDs, 18 HCs | Coronavac | Psoriasis, pemphigus, CSU | No immunosuppressants used, prednisolone, cyclosporine, AZA, MMF, MTX, or biologic drugs (secukinumab, ixekizumab, and omalizumab) | Surrogate neutralizing antibody ≥35% inhibition |
| Baloghová (2022) (61) | Slovakia | Retrospective cohort | 188 vaccinated IMDDs, 144 unvaccinated IMDDs | BNT162b2, mRNA-1273, AZD1222, Sputnik V, Ad26.COV2.S, heterogeneous vaccine | Psoriasis | Topicals, MTX, cyclosporine, apremilast, adalimumab, etanercept, ustekinumab, secukinumab, ixekizumab, brodalumab, risankizumab, or guselkumab | – |
| Huang (2021) (30) | Taiwan | Prospective cohort | 51 vaccinated IMDDs, 32 unvaccinated IMDDs | mRNA-1273, AZD1222 | Psoriasis | Non-biologic or biologic drugs | – |
| Yıldırım (2021) (31) | Turkey | Retrospective cohort | 28 vaccinated IMDDs, 8 unvaccinated IMDDs | BNT162b2, Coronavac, heterogeneous vaccine | CSU | Omalizumab | – |
| Kridin (2022) (25) | Israel | Retrospective cohort | 58,582 vaccinated IMDDs, 19,100 unvaccinated IMDDs | BNT162b2 | AD | Phototherapy, cyclosporine, AZA, MMF, MTX, or dupilumab | – |
| AD: atopic dermatitis; RBD: receptor binding domain; AU: arbitrary units; AZA: azathioprine; CLE: cutaneous lupus erythematosus; CSU: chronic spontaneous urticaria; EC50: half-maximal effective concentration; HC: healthy control; i: inhibitor; Ig: immunoglobulin; IL: interleukin; IMDD: immune-mediated dermatological disease; MMF: mycophenolate mofetil; mRNA: messenger ribonucleic acid; MTX: methotrexate; S: S1 units; TNF: tumour necrosis factor. | |||||||
| Outcome | Studies n | n | Pooled risk ratio/mean difference (95% CI) | I2 (%) |
| Seroconversion: Overall | 6 | 3,887 | 0.96 (0.88,1.06) | 80.03 |
| Diseases | ||||
| Psoriasis | 4 | 3,631 | 0.99 (0.90, 1.09) | 84.62 |
| Other IMDDs | 2 | 256 | 0.88 (0.78, 1.00) | 0.00 |
| Biologics | ||||
| Yes | 4 | 3,631 | 0.99 (0.90, 1.09) | 84.62 |
| No | 2 | 256 | 0.88 (0.78, 1.00) | 0.00 |
| Doses of vaccine | ||||
| One dose | 1 | 94 | 0.80 (0.69, 0.92) | – |
| Two doses | 5 | 3,793 | 1.01 (0.93, 1.09) | 70.09 |
| Vaccination-to-blood sampling interval | ||||
| < 28 days | 1 | 79 | 1.02 (0.94, 1.12) | – |
| ≥ 28 days | 5 | 3,808 | 0.94 (0.84, 1.06) | 84.00 |
| Anti-SARS-CoV-2 IgG antibody*: Overall | 5 | 610 | –36.26 (–117.22, 44.70) | 49.03 |
| Age | ||||
| ≤ 55 years | 2 | 133 | –96.15 (–165.95, –26.34) | 0.00 |
| > 55 years | 3 | 477 | 28.18 (–29.04, 85.40) | 0.00 |
| Diseases | ||||
| Psoriasis | 3 | 354 | –69.46 (–202.63, 63.71) | 0.00 |
| Other IMDDs | 2 | 256 | –28.83 (–145.60, 87.95) | 82.70 |
| Immunosuppressants | ||||
| Yes | 4 | 386 | –85.71 (–152.56, –18.87) | 0.00 |
| No | 1 | 224 | 28.10 (–30.94, 87.14) | – |
| Biologics | ||||
| Yes | 3 | 354 | –69.46 (–202.63, 63.71) | 0.00 |
| No | 2 | 256 | –28.83 (–145.60, 87.95) | 82.70 |
| Vaccine type | ||||
| mRNA vaccines | 3 | 354 | –69.46 (–202.63, 63.71) | 0.00 |
| Other vaccines | 2 | 256 | –28.83 (–145.60, 87.95) | 82.70 |
| Vaccination-to-blood sampling interval | ||||
| <28 days | 1 | 157 | 335.0 (–566.41, 1236.41) | – |
| ≥28 days | 4 | 453 | –39.76 (–123.76, 44.23) | 58.59 |
| T-cell response: Overall | 3 | 394 | 0.86 (0.69, 1.06) | 69.98 |
| Doses of vaccine | ||||
| One dose | 1 | 93 | 1.23 (0.87, 1.73) | – |
| Two doses | 2 | 301 | 0.79 (0.71, 0.88) | 0.00 |
| Vaccination-to-blood sampling interval | ||||
| < 8 days | 1 | 77 | 0.74 (0.61, 0.88) | – |
| ≥28 days | 2 | 317 | 0.97 (0.65, 1.44) | 78.83 |
| Breakthrough COVID-19 infection: Overall | 5 | 1,264,141 | 1.20 (0.79, 1.83) | 67.68 |
| Diseases | ||||
| Psoriasis | 2 | 183 | 0.22 (0.01, 3.48) | 0.00 |
| Other IMDDs | 1 | 1,262,306 | 1.63 (1.28, 2.07) | – |
| Immunosuppressants: Yes | 4 | 1,835 | 0.97 (0.74, 1.28) | 4.78 |
| Biologics: Yes | 2 | 183 | 0.22 (0.01, 3.48) | 0.00 |
| mRNA vaccines: Yes | 4 | 1,263,692 | 1.57 (1.26, 1.95) | 0.00 |
| Adverse events: Overall | 5 | 1,264,291 | 1.24 (0.82, 1.87) | 92.14 |
| Diseases | ||||
| AD | 2 | 1,263,888 | 2.19 (1.05, 4.58) | 89.64 |
| Psoriasis | 2 | 179 | 0.84 (0.72, 0.97) | 0.00 |
| Unclassified | 1 | 224 | 0.92 (0.72, 1.17) | – |
| Immunosuppressants: Yes | 3 | 403 | 0.86 (0.76, 0.97) | 0.00 |
| Biologics | ||||
| Yes | 2 | 179 | 0.84 (0.72, 0.97) | 0.00 |
| No | 1 | 224 | 0.92 (0.72, 1.17) | – |
| Vaccine type | ||||
| mRNA vaccines | 3 | 1,262,485 | 1.29 (0.62, 2.69) | 95.33 |
| Other vaccines | 2 | 1,806 | 1.17 (0.71, 1.92) | 85.60 |
| Doses of vaccine | ||||
| One dose | 2 | 1,679 | 1.11 (0.62, 2.00) | 91.93 |
| Two doses | 2 | 306 | 0.89 (0.73, 1.07) | 0.00 |
| *Pooled mean difference is reported; otherwise the pooled risk ratio is reported. AD: atopic dermatitis; CI: confidence interval; Ig: immunoglobulin; mRNA: messenger ribonucleic acid. |
||||
Immunological response owing to COVID-19 vaccination
Six studies examined the seroconversion rates after COVID-19 vaccination in IMDD patients and HCs. Five studies focused on the seroconversion rate after the second dose of COVID-19 vaccination, while 1 study investigated the seroconversion rate after the first dose. The serologic tests were performed between 14 and 32 days after the vaccination. Among these 6 studies, 3 used serum anti-SARS-CoV-2 IgG antibody concentration, 2 used antibody neutralizing activity, and 1 used both methods. The results showed no significant difference in seroconversion rate between IMDD patients and HCs (pooled RR: 0.96; 95% confidence interval [CI]: 0.88, 1.06) with high heterogeneity (I2=80.03%). The subgroup analysis based on underlying IMDDs, biologic drug use, number of doses, and vaccination-to-blood sampling interval did not reveal the source of heterogeneity or between-group differences. The mean differences in anti-SARS-CoV-2 IgG antibody levels, for which all included studies used the chemiluminescent immunoassay method, were likewise consistently pointing in the same direction (pooled mean difference: –36.26 BAU/mL; 95% CI: –117.22, 44.70; I2=49.03%). However, among participants aged 55 years or younger, the IMDD group appeared to have lower antibody titres than HCs (pooled mean difference: –96.15 BAU/mL; 95% CI: –165.95, –26.34) as shown in Fig. 1. Studies in which the majority of participants were immunosuppressed also had lower antibody titres (pooled mean difference: –85.71 BAU/mL; 95% CI: –152.56, –18.87). Most heterogeneity was also eliminated (i.e. I2=0.0%) among each subgroup of studies with participants aged ≤ 55 years and > 55 years, as well as non-immunosuppressed patients and immunosuppressed patients. However, psoriasis, biologic drug use, mRNA vaccine, and vaccination-to-blood sampling interval were factors not significantly affecting the serum anti-SARS-CoV-2 IgG antibody level. As for the cellular immune response, there were 3 studies, including 2 using spike-specific T-cell production combining interferon-γ, IL-2, and IL-21 (cytokine-secreting cells per million peripheral blood mononuclear cells) to represent the cellular immune response and 1 using interferon-γ concentration (milli-international units per mL) to represent the cellular immune response. The meta-analysis of this outcome revealed no significant difference in T-cell response between IMDD patients and HCs (pooled RR 0.86; 95% CI: 0.69–1.06; I2=69.98%), but an apparently inferior T-cell response of IMDD patients compared with HCs was shown after the second vaccination (pooled RR: 0.79; 95% CI: 0.71–0.88; I2=0.0%). Heterogeneity was also eliminated with those vaccinated with the second dose of COVID-19 vaccine (I2=0.0%), while the vaccine-to-blood sampling time did not impact the heterogeneity.
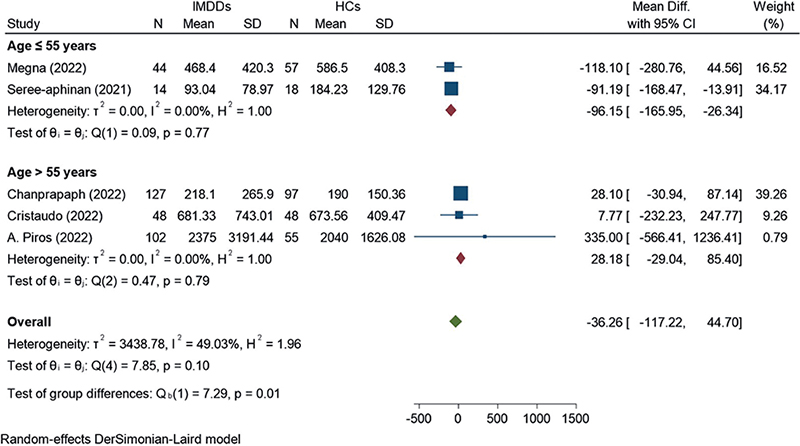
Fig. 1. Pooled mean differences in anti-SARS-CoV-2 IgG antibody level between vaccinated immune-mediated dermatological disease (IMDD) patients and healthy controls (HCs) stratified by mean age. CI: confidence interval; Ig: immunoglobulin.
Breakthrough COVID-19 infection and COVID-19-associated hospitalization
The pooled results from 4 studies showed that the incidence of COVID-19 infection in vaccinated IMDD patients was significantly lower than those unvaccinated (pooled RR: 0.34; 95% CI: 0.16, 0.72; I2=89.71%) (Fig. 2). This was true even among immunosuppressed patients (pooled RR: 0.43; 95% CI: 0.19, 0.99) and non-biologic drug users (pooled RR: 0.25; 95% CI: 0.18, 0.36). Patients immunized with 2 doses of COVID-19 vaccine had a reduced risk of COVID-19 infection (pooled RR: 0.22; 95% CI: 0.18, 0.28); on the other hand, 1 vaccine dose may not have a preventive benefit (pooled RR: 0.74; 95% CI: 0.51, 1.09). The number of COVID-19 vaccine doses is also a source of heterogeneity (I2=0.0%, p-value <0.001) for the COVID-19 infection outcome.
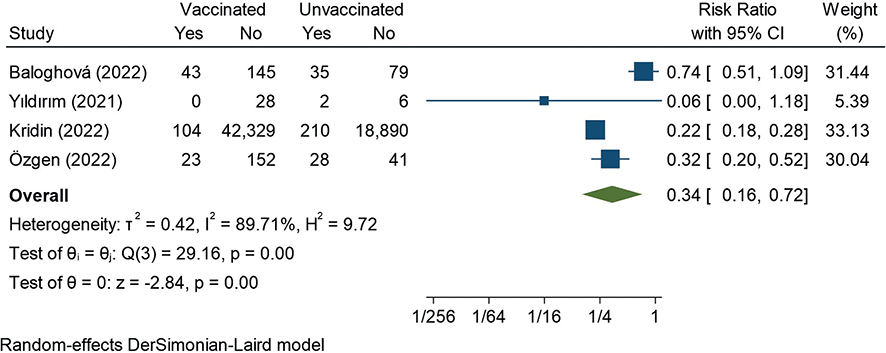
Fig. 2. Pooled risk ratio for COVID-19 infection between vaccinated and unvaccinated immune-mediated dermatological disease patients. CI: confidence interval.
In terms of severity of COVID-19 infection, vaccinated IMDD patients had a lower risk of COVID-19-associated hospitalization (pooled RR: 0.11; 95% CI: 0.06, 0.2; I2=0.0%). Kridin et al. (25) also reported COVID-19-associated mortality, which was 2/42,433 (0.005%) in vaccinated patients and 9/19,100 (0.047%) in unvaccinated patients, while Özgen et al. (26) reported a mortality rate of 0.4% (1/244) among vaccinated patients who succumbed to COVID-19, although no control group was included. It is important to note that vaccinated IMDD patients still faced a higher risk of COVID-19 infection when compared with vaccinated HCs, particularly in mRNA vaccine studies (pooled RR: 1.57; 95% CI: 1.26, 1.95; I2=67.68%). Subgroup analysis revealed no significant difference in COVID-19 infection among vaccinated IMDD patients with psoriasis (pooled RR: 0.22, 95% CI: 0.01, 3.48), immunosuppressant users (pooled RR: 0.97, 95% CI: 0.74, 1.28), or biologic drug users (pooled RR: 0.22, 95% CI: 0.01, 3.48), in comparison with vaccinated HCs. Two studies by Mahil et al. (27,28), conducted in patients with psoriasis using methotrexate, TNF inhibitors, IL-17 inhibitors, or IL-23 inhibitors immunized with BNT162b2, reported no evidence of COVID-19 infection.
Adverse events and immune-mediated dermatological diseases exacerbation from COVID-19 vaccination
Although the incidence of AEs, based on data from 15,617 vaccinated IMDD patients and 1,248,674 vaccinated HCs, was not different between the two groups (pooled RR: 1.24; 95% CI: 0.82, 1.87; I2=92.17%), subgroup analysis by specific diseases showed that patients with AD had a higher risk of AEs (pooled RR: 2.19; 95% CI: 1.05, 4.58). The largest study, including 15,306 AD patients, by Pakhchanian et al. (29), reported that 28 (0.2%) patients experienced more one-day immediate events (RR: 3.23; 95% CI: 2.21, 4.71) and 48 (0.4%) patients had more AEs of special interest (as defined by the FDA) within 90 days after the vaccination (RR: 1.34; 95% CI: 1.00, 1.77), relative to HCs. Conversely, those with psoriasis had a lower risk for AEs (pooled RR: 0.84; 95% CI: 0.72, 0.97) according to 2 studies in this specific group of patients (Fig. 3). In addition, immunosuppressed patients had a lower incidence of AEs than HCs, without heterogeneity (pooled RR: 0.86; 95% CI: 0.76, 0.97; I2=0.0%). Subgroup analysis by the number of doses and mRNA vaccines did not show significant differences. The subgroup analysis based on type or severity of AEs cannot be performed due to insufficient data and disparities in definition between the included studies. Although only 2 studies showed exacerbation of IMDD in the vaccinated compared with the unvaccinated, COVID-19 vaccination has been observed to increase the risk of disease exacerbation among IMDD patients, as evidenced by the higher incidence among vaccinated individuals compared with those unvaccinated (pooled RR: 3.57; 95% CI: 0.99, 12.89). These studies, by Huang et al. (30) and Koç Yıldırım et al. (31), were conducted in patients with psoriasis and CSU, respectively. The mean interval between vaccination and exacerbation in the study by Huang et al. was 9.3 ± 4.1 days, and 3 (5%) of the vaccinated patients reported a morphologic change from chronic plaque-type to guttate psoriasis, whereas none of the unvaccinated patients experienced disease flares. Koç Yıldırım et al. report 1 case of CSU exacerbation after 4 weeks of the first dose of mRNA vaccine.
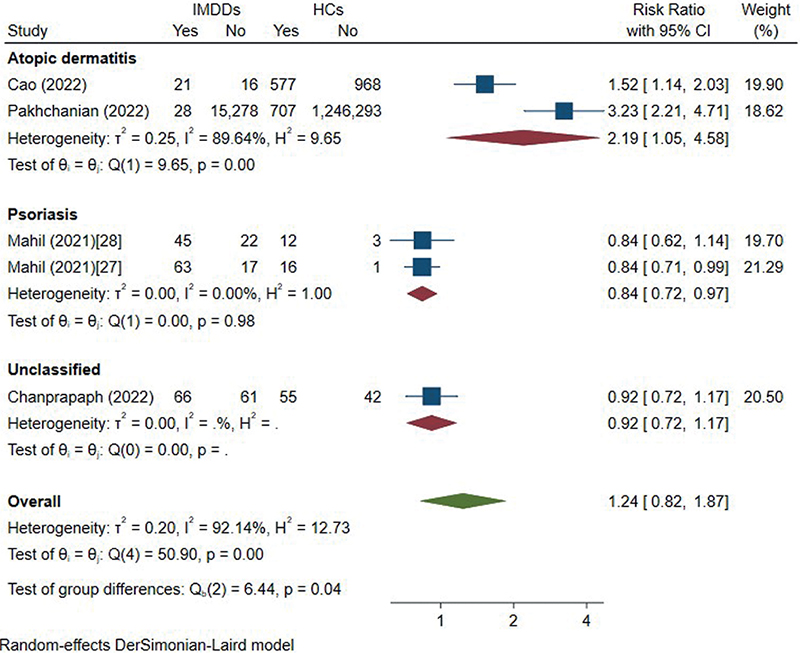
Fig. 3. Pooled risk ratios for adverse events between vaccinated immune-mediated dermatological disease (IMDD) patients and healthy controls (HCs) stratified by underlying IMDDs. CI: confidence interval.
Publication bias
Figs S2 and S3 show the funnel plots and contour-enhanced funnel plots for meta-analyses of the seroconversion, anti-SARS-CoV-2 IgG antibody, breakthrough COVID-19 infection, and AE outcomes in vaccinated IMDD patients compared with vaccinated HCs and breakthrough COVID-19 infection in vaccinated IMDD patients compared with unvaccinated IMDD patients, respectively. All the funnel plots appeared asymmetric, but the contour-enhanced funnel plots for the meta-analyses of the comparisons between vaccinated IMDD patients and vaccinated HCs contained considerable numbers of studies in the non-significant areas (see Fig. S2), suggesting heterogeneity as a source of the asymmetry. Nonetheless, the contour-enhanced funnel plot for the meta-analysis on breakthrough COVID-19 infection between vaccinated and unvaccinated IMDD patients lacked studies in the non-significant area (see Fig. S3), thus publication bias was likely present in this meta-analysis.
DISCUSSION
This is the first systematic review and meta-analysis that evaluates the immunogenicity, effectiveness, and safety of COVID-19 vaccines among IMDD patients in comparison with HCs and unvaccinated IMDD counterparts. While the pooled seroconversion rates between IMDD patients and HCs were not different, IMDD aged ≤55 and immunosuppressed patients exhibited lower mean anti-SARS-CoV-2 IgG levels compared with HCs. T-cell responses remained similar between groups. Vaccinated IMDD patients had a reduced risk of breakthrough COVID-19 infection and COVID-19-associated hospitalization, albeit a higher risk of COVID-19 infection compared with HCs. Although vaccination can prevent COVID-19 infection, it may exacerbate certain IMDDs. AEs were more common in AD patients compared with HCs, while psoriasis patients had a lower risk. Furthermore, immunosuppressed patients had a lower incidence of AEs.
Previous studies on IMDD patients’ humoral immune responses in psoriasis, AIBD, and CSU patients showed no statistically significant differences from HCs (27, 32–37). By stratifying participants of the IMDD group into individual diseases, Chanprapaph et al. demonstrated that AIBD patients exhibit poor immune responses, whereas psoriasis patients develop comparable post-vaccination immune responses to a healthy population (32). As most of the included studies investigated immune responses in psoriasis patients, this is consistent with our findings that the pooled seroconversion rate was comparable between groups. However, this result is somewhat contradictory to previous studies conducted in immune-mediated inflammatory disease and inflammatory bowel disease patients, where inferior immunological responses were demonstrated (12, 15, 38–40). This may be due to more aggressive treatment regimens for immune-mediated diseases of other organs compared with the skin. Studies on other vaccines such as influenza and hepatitis showed that these vaccines were able to induce a significant humoral response in autoimmune disease patients, but the antibody response was reduced in those treated with methotrexate, azathioprine, mycophenolate mofetil, or rituximab (41–46). Our data addressed the fact that patients aged ≤ 55 had a lower antibody response than HCs, while those aged > 55 years had a comparable response. The latter finding may be explained by the reduced immunogenicity of vaccines in the elderly that is likely attributed to the age-related decline in immune function, also known as immunosenescence, in which both innate and adaptive immune responses are impaired (47–49). There are several studies that demonstrate lower vaccine response in association with older age and comorbidities (12, 28, 40, 41). Our results also showed that IMDD patients receiving immunosuppressive drugs had a lower anti-SARS-CoV-2 IgG level than HCs. This is consistent with prior studies of immunosuppressed patients taking rituximab, mycophenolate, azathioprine, and glucocorticoids (15, 16, 38). However, one should be cautious that the same medications may not exert the same degree of immunosuppression in different diseases. For instance, methotrexate may suppress vaccine responses in psoriatic arthritis patients, but does not appear to do the same for psoriasis (32). Similar to humoral immunity, the cellular immune responses in IMDD patients were comparable to HCs. This is believed to be an important component of protective response against SARS-CoV-2 infection, even in some situations where neutralizing response is not robust (39, 50).
In terms of clinical outcomes, vaccinated IMDD patients had a lower risk of breakthrough COVID-19 infection compared with those unvaccinated. Meanwhile, the vaccinated IMDD patients had a higher risk of COVID-19 infection than HCs. Additionally, IMDD patients seem to have higher risk of COVID-19 infection relative to patients with immune-mediated diseases affecting other organs such as inflammatory bowel disease (16, 17, 39). Based on our results, we propose that the seroconversion rate and likelihood of COVID-19 infection may be influenced by the immune-mediated disease itself, together with the severity and immunosuppressants used.
An effective strategy for COVID-19 vaccination in immunosuppressed IMDD individuals involves establishing an appropriate interval between immunosuppressant administration and vaccination (51). Additional doses, including both primary and booster doses of COVID-19 vaccines, are also crucial, as they have the potential to enhance SARS-CoV-2-specific immunity and delay breakthrough COVID-19 infections, respectively (52). However, it is important to remain vigilant regarding the reactogenicity after the booster dose, especially following an asymptomatic priming cycle with the same types of COVID-19 vaccine, due to an excessive stimulation of the immune response (53).
The ongoing pandemic presents challenges with various immune-mediated skin manifestations following vaccination, such as CLE, bullous pemphigoid, cutaneous vasculitis, and vasculopathy, the pathogenic mechanisms of which are not fully understood (54,55). On the other hand, individuals with IMDDs may be prone to COVID-19 vaccination-related AEs, as indicated by our results showing that patients with AD experienced a high frequency of such events. This aligns with earlier findings regarding smallpox vaccination in this population, which demonstrated increased rates of administration site and cutaneous reactions, albeit being transient and requiring no medication (56). These findings emphasize the need for physicians to exercise greater caution when vaccinating AD patients.
Limitations
This systematic review and meta-analysis was subject to some limitations. First, the study did not take into account demographic variables including age, sex, disease severity, and comorbidities, and there was heterogeneity or data paucity in respect of immunosuppressants used, type of vaccines, and timing of various determined outcomes. We attempted to minimize the heterogeneity through subgrouping the studies by their participants’ characteristics, including age group and immunosuppressants. Additionally, it is crucial to note that the use of different assays to assess the antibodies against SARS-CoV-2 and seroconversion rate among the studies could influence the outcomes. Moreover, IMDDs were analysed collectively owing to the limited number of studies. Also, as there was disparity of definition of type and severity of AEs among studies, we were unable to perform pooled estimates on these outcomes. Finally, there is a lack of studies on booster doses of COVID-19 vaccines and non-mRNA vaccines.
Conclusion
This systematic review and meta-analysis revealed that COVID-19 vaccination in patients with IMDDs elicited seroconversion rates and T-cell responses comparable to HCs. COVID-19 vaccination among IMDD patients can reduce the risk of breakthrough COVID-19 infection and COVID-19-associated hospitalization. While using immunosuppressant lowered antibody titres, it also mitigated the risk of AEs. The type of IMDD influenced the risk of AEs. Finally, COVID-19 vaccination remains an effective and well-tolerated strategy for preventing COVID-19 in this population.
REFERENCES
- Pormohammad A, Zarei M, Ghorbani S, Mohammadi M, Razizadeh MH, Turner DL, et al. Efficacy and safety of COVID-19 vaccines: a systematic review and meta-analysis of randomized clinical trials. Vaccines 2021; 9: 467.
- Sharif N, Alzahrani KJ, Ahmed SN, Dey SK. Efficacy, immunogenicity and safety of COVID-19 vaccines: a systematic review and meta-analysis. Front Immunol 2021; 12: 714170.
- Liu Q, Qin C, Liu M, Liu J. Effectiveness and safety of SARS-CoV-2 vaccine in real-world studies: a systematic review and meta-analysis. Infect Dis Poverty 2021; 10: 132.
- Zeng B, Gao L, Zhou Q, Yu K, Sun F. Effectiveness of COVID-19 vaccines against SARS-CoV-2 variants of concern: a systematic review and meta-analysis. BMC Med 2022; 20: 200.
- Rotshild V, Hirsh-Raccah B, Miskin I, Muszkat M, Matok I. Comparing the clinical efficacy of COVID-19 vaccines: a systematic review and network meta-analysis. Sci Rep 2021; 11: 22777.
- Wu Q, Dudley MZ, Chen X, Bai X, Dong K, Zhuang T, et al. Evaluation of the safety profile of COVID-19 vaccines: a rapid review. BMC Med 2021; 19: 173.
- Manuel O, Estabrook M. RNA respiratory viral infections in solid organ transplant recipients: guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin Transplant 2019; 33: e13511.
- Couch RB, Englund JA, Whimbey E. Respiratory viral infections in immunocompetent and immunocompromised persons. Am J Med 1997; 102: 2–9.
- Coronavirus Disease 2019 (COVID-19) Treatment guidelines. Bethesda (MD): National Institutes of Health (US); 2021.
- Jayasinghe S, Patel C, Armstrong L, Chiu C, Macartney K, Flanagan K, et al. ATAGI Targeted Review 2021: the national COVID-19 vaccination program. Commun Dis Intell (2018) 2023; 47.
- Shoham S, Batista C, Ben Amor Y, Ergonul O, Hassanain M, Hotez P, et al. Vaccines and therapeutics for immunocompromised patients with COVID-19. EClinicalMedicine 2023; 59: 101965.
- Sakuraba A, Luna A, Micic D. Serologic response to coronavirus disease 2019 (COVID-19) vaccination in patients with immune-mediated inflammatory diseases: a systematic review and meta-analysis. Gastroenterology 2022; 162: 88–108.
- Lee ARYB, Wong SY, Tay SH. Booster COVID-19 vaccines for immune-mediated inflammatory disease patients: a systematic review and meta-analysis of efficacy and safety. Vaccines 2022; 10: 668.
- Sakuraba A, Luna A, Micic D. A systematic review and meta-analysis of serologic response following coronavirus disease 2019 (COVID-19) vaccination in solid organ transplant recipients. Viruses 2022; 14: 1822.
- Sood A, Tran M, Murthy V, Gonzalez E. Immunogenicity and safety of SARS-CoV-2 vaccination in patients with rheumatic diseases: a systematic review and meta-analysis. J Clin Rheumatol 2022; 28: 381–389.
- Sung KY, Chang TE, Wang YP, Lin CC, Chang CY, Hou MC, et al. SARS-CoV-2 vaccination in patients with inflammatory bowel disease: a systemic review and meta-analysis. J Chin Med Assoc 2022; 85: 421–430.
- Bhurwal A, Mutneja H, Bansal V, Goel A, Arora S, Attar B, et al. Effectiveness and safety of SARS-CoV-2 vaccine in inflammatory bowel disease patients: a systematic review, meta-analysis and meta-regression. Aliment Pharmacol Ther 2022; 55: 1244–1264.
- James D, Jena A, Bharath PN, Choudhury A, Singh AK, Sebastian S, et al. Safety of SARS-CoV-2 vaccination in patients with inflammatory bowel disease: a systematic review and meta-analysis. Dig Liver Dis 2022; 54: 713–721.
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021; 372: 71.
- Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol 2010; 25: 603–605.
- Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016; 355: i4919.
- Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol 2014; 14: 135.
- Kristiansen PA, Page M, Bernasconi V, Mattiuzzo G, Dull P, Makar K, et al. WHO International Standard for anti-SARS-CoV-2 immunoglobulin. Lancet 2021; 397: 1347–1348.
- Graceffa D, Sperati F, Bonifati C, Spoletini G, Lora V, Pimpinelli F, et al. Immunogenicity of three doses of anti-SARS-CoV-2 BNT162b2 vaccine in psoriasis patients treated with biologics. Front Med 2022; 9: 961904.
- Kridin K, Schonmann Y, Onn E, Bitan DT, Weinstein O, Cohen AD. Determinants and effectiveness of BNT162b2 mRNA vaccination among patients with atopic dermatitis: a population-based study. Am J Clin Dermatol 2022; 23: 385–392.
- Özgen Z, Aksoy H, Akın Çakıcı Ö, Koku Aksu AE, Erdem O, Kara Polat A, et al. COVID-19 severity and SARS-Cov-2 vaccine safety in pemphigus patients. Dermatol Ther 2022; 35: e15417.
- Mahil SK, Bechman K, Raharja A, Domingo-Vila C, Baudry D, Brown MA, et al. Humoral and cellular immunogenicity to a second dose of COVID-19 vaccine BNT162b2 in people receiving methotrexate or targeted immunosuppression: a longitudinal cohort study. Lancet Rheumatol 2022; 4: 42–52.
- Mahil SK, Bechman K, Raharja A, Domingo-Vila C, Baudry D, Brown MA, et al. The effect of methotrexate and targeted immunosuppression on humoral and cellular immune responses to the COVID-19 vaccine BNT162b2: a cohort study. Lancet Rheumatol 2021; 3: 627–637.
- Pakhchanian H, Raiker R, Wolf M, Trotter SC. Examining the risk of breakthrough infection and COVID-19 vaccination safety in patients with atopic dermatitis. Br J Dermatol 2022; 187: 251–253.
- Huang YW, Tsai TF. Exacerbation of psoriasis following COVID-19 vaccination: report from a single center. Front Med 2021; 8: 812010.
- Koç Yıldırım S, Demirel Öğüt N, Erbağcı E. Retrospective evaluation of patients with chronic spontaneous urticaria using omalizumab during the COVID-19 pandemic. J Cosmet Dermatol 2022; 21: 431–434.
- Chanprapaph K, Seree-Aphinan C, Rattanakaemakorn P, Pomsoong C, Ratanapokasatit Y, Setthaudom C, et al. A real-world prospective cohort study of immunogenicity and reactogenicity of ChAdOx1-S[recombinant] among patients with immune-mediated dermatologic diseases. Br J Dermatol 2023; 188: 268–277.
- Cristaudo A, Graceffa D, Pimpinelli F, Sperati F, Spoletini G, Bonifati C, et al. Immunogenicity and safety of anti-SARS-CoV-2 BNT162b2 vaccine in psoriasis patients treated with biologic drugs. J Eur Acad Dermatol Venereol 2022; 36: 266–268.
- Piros ÉA, Cseprekál O, Görög A, Hidvégi B, Medvecz M, Szabó Z, et al. Seroconversion after anti-SARS-CoV-2 mRNA vaccinations among moderate-to-severe psoriatic patients receiving systemic biologicals: prospective observational cohort study. Dermatol Ther 2022; 35: e15408.
- Pavlotsky F, Segal Z, Barzilai A. Antibody response to BNT162b2 vaccine in immune modifiers-treated psoriatic patients. J Psoriasis Psoriatic Arthritis 2022; 7: 24–28.
- Seree-Aphinan C, Chanprapaph K, Rattanakaemakorn P, Setthaudom C, Suangtamai T, Pomsoong C, et al. Inactivated COVID-19 vaccine induces a low humoral immune response in a subset of dermatological patients receiving immunosuppressants. Front Med 2021; 8: 769845.
- Megna M, Potestio L, Battista T, Camela E, Genco L, Noto M, et al. Immune response to COVID-19 mRNA vaccination in patients with psoriasis undergoing treatment with biologics. Clin Exp Dermatol 2022; 47: 2310–2312.
- Jena A, Mishra S, Deepak P, Kumar MP, Sharma A, Patel YI, et al. Response to SARS-CoV-2 vaccination in immune mediated inflammatory diseases: systematic review and meta-analysis. Autoimmun Rev 2022; 21: 102927.
- Jena A, James D, Singh AK, Dutta U, Sebastian S, Sharma V. Effectiveness and durability of COVID-19 vaccination in 9447 patients with IBD: a systematic review and meta-analysis. Clin Gastroenterol Hepatol 2022; 20: 1456–1479.
- Sakuraba A, Luna A, Micic D. Serologic response following SARS-COV2 vaccination in patients with cancer: a systematic review and meta-analysis. J Hematol Oncol 2022; 15: 15.
- Seyahi E, Bakhdiyarli G, Oztas M, Kuskucu MA, Tok Y, Sut N, et al. Antibody response to inactivated COVID-19 vaccine (CoronaVac) in immune-mediated diseases: a controlled study among hospital workers and elderly. Rheumatol Int 2021; 41: 1429–1440.
- Kostianovsky A, Charles P, Alves JF, Goulet M, Pagnoux C, Le Guern V, et al. Immunogenicity and safety of seasonal and 2009 pandemic A/H1N1 influenza vaccines for patients with autoimmune diseases: a prospective, monocentre trial on 199 patients. Clin Exp Rheumatol 2012; 30: S83–S89.
- Elkayam O, Yaron M, Caspi D. Safety and efficacy of vaccination against hepatitis B in patients with rheumatoid arthritis. Ann Rheum Dis 2002; 61: 623–625.
- Erkek E, Ayaslioglu E, Erkek AB, Kurtipek GS, Bagci Y. Response to vaccination against hepatitis B in patients with Behcet’s disease. J Gastroenterol Hepatol 2005; 20: 1508–1511.
- McMahan ZH, Bingham CO 3rd. Effects of biological and non-biological immunomodulatory therapies on the immunogenicity of vaccines in patients with rheumatic diseases. Arthritis Res Ther 2014; 16: 506.
- Bingham CO 3rd, Looney RJ, Deodhar A, Halsey N, Greenwald M, Codding C, et al. Immunization responses in rheumatoid arthritis patients treated with rituximab: results from a controlled clinical trial. Arthritis Rheum 2010; 62: 64–74.
- Crooke SN, Ovsyannikova IG, Poland GA, Kennedy RB. Immunosenescence and human vaccine immune responses. Immun Ageing 2019; 16: 25.
- Stiasny K, Aberle JH, Keller M, Grubeck-Loebenstein B, Heinz FX. Age affects quantity but not quality of antibody responses after vaccination with an inactivated flavivirus vaccine against tick-borne encephalitis. PLoS One 2012; 7: e34145.
- Müller L, Andrée M, Moskorz W, Drexler I, Walotka L, Grothmann R, et al. Age-dependent immune response to the Biontech/Pfizer BNT162b2 coronavirus disease 2019 vaccination. Clin Infect Dis 2021; 73: 2065–2072.
- Ahmed SF, Quadeer AA, McKay MR. SARS-CoV-2 T cell responses elicited by COVID-19 vaccines or infection are expected to remain robust against Omicron. Viruses 2022; 14: 79.
- Seree-Aphinan C, Ratanapokasatit Y, Suchonwanit P, Rattanakaemakorn P, O-Charoen P, Pisitkun P, et al. Optimal time for COVID-19 vaccination in rituximab-treated dermatologic patients. Front Immunol 2023; 14: 1138765.
- Seree-Aphinan C, Suchonwanit P, Rattanakaemakorn P, Pomsoong C, Ratanapokasatit Y, Setthaudom C, et al. Risk-benefit profiles associated with receiving Moderna COVID-19 (mRNA-1273) vaccine as an additional pre-booster dose in immune-mediated dermatologic disease patients with low SARS-CoV-2-specific immunity following the primary series: a prospective cohort study. J Eur Acad Dermatol Venereol 2023; 37: e572–e575.
- Avallone G, Cavallo F, Astrua C, Caldarola G, Conforti C, De Simone C, et al. Cutaneous adverse reactions following SARS-CoV-2 vaccine booster dose: a real-life multicentre experience. J Eur Acad Dermatol Venereol 2022; 36: e876–e879.
- Nakashima C, Kato M, Otsuka A. Cutaneous manifestations of COVID-19 and COVID-19 vaccination. J Dermatol 2023; 50: 280–289.
- Maronese CA, Zelin E, Avallone G, Moltrasio C, Romagnuolo M, Ribero S, et al. Cutaneous vasculitis and vasculopathy in the era of COVID-19 pandemic. Front Med 2022; 9: 996288.
- von Sonnenburg F, Perona P, Darsow U, Ring J, von Krempelhuber A, Vollmar J, et al. Safety and immunogenicity of modified vaccinia Ankara as a smallpox vaccine in people with atopic dermatitis. Vaccine 2014; 32: 5696–5702.
- Boekel L, Stalman EW, Wieske L, Hooijberg F, van Dam KPJ, Besten YR, et al. Breakthrough SARS-CoV-2 infections with the delta (B.1.617.2) variant in vaccinated patients with immune-mediated inflammatory diseases using immunosuppressants: a substudy of two prospective cohort studies. Lancet Rheumatol 2022; 4: e417–e429.
- Stalman EW, Wieske L, van Dam KPJ, Kummer LY, van Kempen ZLE, Killestein J, et al. Breakthrough infections with the SARS-CoV-2 omicron (B.1.1.529) variant in patients with immune-mediated inflammatory diseases. Ann Rheum Dis 2022; 81: 1757–1766.
- Cao C, Qiu F, Lou C, Fang L, Liu F, Zhong J, et al. Safety of inactivated SARS-CoV-2 vaccines in patients with allergic diseases. Respir Res 2022; 23: 133.
- Piros ÉA, Cseprekál O, Görög A, Hidvégi B, Medvecz M, Szabó Z, et al. Seroconversion after anti-SARS-CoV-2 mRNA vaccinations among moderate-to-severe psoriatic patients receiving systemic biologicals: prospective observational cohort study. Dermatol Ther 2022; 35: e15408.
- Baloghová J, Kampe T, Kolarčik P, Hatalová E. Vaccination, risk factors and outcomes of COVID-19 infection in patients with psoriasis: a single centre real-life experience from eastern Slovakia. Viruses 2022; 14: 1646.