SHORT COMMUNICATION
Clinical and Laboratory Differences between Steroid-associated and Non-steroid-associated Rosacea: A Retrospective Study
Tae Min KIM1 and Soyun CHO1,2*
1Department of Dermatology, Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Seoul National University, 20 Boramae Road 5-gil, Dongjak-gu, Seoul 07061, Korea, and 2Department of Dermatology, Seoul National University College of Medicine, Seoul, Korea. *E-mail: sycho@snu.ac.kr
Citation: Acta Derm Venereol 2024; 104: adv40045. DOI: https://doi.org/10.2340/actadv.v104.40045.
Copyright: © 2024 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Feb 4, 2024; Accepted after revision: Apr 11, 2024. Published: May 6, 2024
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Excessive use of topical steroids for over 2 months is well known to cause steroid-induced rosacea, with mechanisms such as rebound vasodilation and pro- inflammatory cytokine secretion proposed as pathogenesis (1, 2). Specifically, when applied to the facial area, the thin corneal layer and high skin permeability through numerous sebaceous glands increase the risk (2, 3). It is known that the risk of adrenocortical insufficiency due to the use of topical steroids increases when they are used on areas with thin skin, such as the face, or when high-potency steroids are used for an extended period (4). While there exists descriptive research on the clinical classification and accompanying symptoms of steroid-associated rosacea based on lesion distribution, in-depth investigation into its clinical and laboratory characteristics is lacking (1, 2, 5, 6).
MATERIALS AND METHODS
We retrospectively analysed the medical records of patients diagnosed with rosacea who visited the Dermatology Department at Boramae Medical Center between September 2020 and March 2023. Following an IRB-approved protocol, we assessed steroid usage history, rosacea type, affected areas, and baseline laboratory features including serum cortisol and adrenocorticotropic hormone (ACTH) levels. The study participants were categorized based on their previous history of steroid use. Those with no prior history of steroid use were included in the non-steroid-associated group, while those with a history of topical steroid use for more than 1 month, systemic steroid use regardless of duration, or confirmed use of other forms of steroids (intraarticular, etc.) at least once were classified into an all steroid-associated group. Participants in whom only the use of topical steroids was confirmed were classified into a topical steroid-associated group as a subgroup, while those who exclusively reported systemic steroid intake without the use of other steroid forms were categorized into a systemic steroid-associated group.
Statistical analysis
We performed all statistical analyses using the Statistical Package for the Social Sciences (SPSS, version 23.0; IBM Corp, Armonk, NY, USA). Continuous variables are presented as the mean and standard deviation (SD), while categorical variables are represented as frequencies. The χ2 test was used to assess the correlation between steroid usage history and categorical or ordinal variables, including sex, comorbidity, and affected areas. To estimate the odds ratio (OR) and 95% confidence interval (CI) for the likelihood of eyelid involvement, an ordinal logistic regression model was performed.
RESULTS
A total of 192 patients with all steroid-associated rosacea, including 103 topical steroid-associated, 46 systemic steroid-associated, 7 other steroid form-associated, and 36 mixed steroid form-associated rosacea, were identified, alongside 264 non-steroid-associated patients. The average ages of both the all steroid-associated group (50.9 ± 16.8 years) and the topical steroid-associated group (51.5 ± 17.6 years) were higher compared with the non-steroid-associated group (46.8 ± 15.7, p < 0.01 and p = 0.018, respectively, Table I). However, there were no significant differences among the groups in terms of gender, BMI, and comorbidities, including diabetes. The steroid usage duration in the all steroid-associated group had an average of 388 ± 740 days, with a median value of 100 days. Both the topical steroid-associated group (median: 150 days, mean: 427 ± 769 days) and the systemic steroid-associated group (median: 150 days, mean: 427 ± 769 days) demonstrated a heterogeneous distribution of steroid usage periods (Table I). Upon examination of rosacea types, it was observed that the all steroid-associated group and topical steroid-associated group had a lower prevalence of phymatous rosacea at 3.1% (p = 0.048) and 1.9% (p = 0.027), respectively, compared with the non-steroid-associated group at 8.3% (Table II). In comparison with the non-steroid-associated group, the odds ratio for eyelid involvement in the all steroid-associated group was 12.1 (95% CI; 5.8–25.2). Additionally, eyelid involvement was significantly more common in the topical steroid-associated group (40.8% vs 3.4%, p < 0.01), but not in the systemic steroid-associated group (8.7%, p = 0.08, Table I). Serum cortisol levels (normal range, 5–25 μg/dL) were lower in the all steroid-associated group at 7.7 μg/dL, compared with the non-steroid-associated group at 14.1 μg/dL (p < 0.01), and the proportion of patients with serum cortisol levels lower than 5 μg/dL was also significantly higher in the all steroid-associated group (27.7% vs. 3.0%, p < 0.01, Fig. 1 and Table II). The HbA1c level was higher in the all steroid-associated group (6.4 vs 5.6%, p = 0.02) and the topical steroid-associated group (7.0%, p = 0.04) compared with the non-steroid-associated group (6.4 vs 5.6 %, p = 0.02, Table SI). Other laboratory features demonstrated no statistically significant differences between the steroid-associated and non-steroid-associated groups (Table SI).
| Factor | Non-steroid-associated rosacea (n = 264) | All steroid-associated rosacea (n = 192) | p-value | Topical steroid-associated rosacea (n = 103) | p-value | Systemic steroid-associated rosacea (n = 46) | p-value |
| Age, years, mean ± SD | 46.8 ± 15.7 | 50.9 ± 16.8 | 0.010* | 51.5 ± 17.6 | 0.018* | 49.9 ± 17.7 | 0.452 |
| Gender, (%) | |||||||
| Male | 21.2 | 23.4 | 0.572 | 19.4 | 0.734 | 30.4 | 0.22 |
| Female | 78.8 | 76.6 | 80.6 | 69.6 | |||
| BMI, kg/cm2, mean ± SD | 22.9 ± 3.5 | 23.2 ± 4.1 | 0.519 | 22.7 ± 3.5 | 0.91 | 23.9 ± 4.1 | 0.279 |
| Comorbidity, % | |||||||
| Yes | 71.9 | 77.6 | 0.172 | 74.8 | 0.74 | 86.9 | 0.061 |
| No | 28.1 | 22.4 | 25.2 | 13.1 | |||
| Previous steroid use | |||||||
| Oral, n (%) | – | 73 (38.0) | – | – | – | – | – |
| Topical, n (%) | – | 137 (71.4) | – | – | – | – | – |
| Intralesional/intra-articular, n (%) | – | 15 (7.8) | – | – | – | – | – |
| Steroid-use duration, day, mean ± SD | – | 388 ± 740 | – | 427 ± 769 | – | 205 ± 324 | – |
| Steroid-use duration, day, median | – | 100 | – | 100 | – | 90 | – |
| Other steroid forms and mixed steroid form use patients were not included for analysis due to low number of each form and heterogeneity in steroid usage history BMI: body mass index; SD: standard deviation. *p < 0.05. |
|||||||
| Non-steroid-associated rosacea (n = 264) | All steroid-associated rosacea* (n = 192) | p-value | Topical steroid-associated rosacea (n = 103) | p-value | Systemic steroid-associated rosacea (n = 46) | p-value | |
| Rosacea type | |||||||
| Erythematotelangiectatic, % | 66.7 | 73.4 | 0.29 | 73.8 | 0.205 | 69.6 | 0.93 |
| Papulopustular, % | 28.4 | 30.2 | 0.39 | 29.1 | 0.849 | 41.3 | 0.08 |
| Phymatous, % | 8.3 | 3.1 | 0.048* | 1.9 | 0.027* | 2.2 | 0.16 |
| Ocular, % | 0.8 | 1.0 | 0.68 | 1.0 | 0.832 | 2.2 | 0.40 |
| Lesion involved area | |||||||
| Cheek, % | 94.7 | 99.0 | 0.028* | 99.0 | 0.13 | 97.8 | 0.34 |
| Forehead, % | 54.9 | 57.3 | 0.70 | 56.3 | 0.86 | 58.7 | 0.82 |
| Nose, % | 48.5 | 51.6 | 0.77 | 50.5 | 0.84 | 56.5 | 0.31 |
| Chin, % | 49.6 | 51.0 | 0.61 | 47.6 | 0.54 | 47.8 | 0.60 |
| Eyelid, % | 3.4 | 31.3 | < 0.01** | 40.8 | < 0.01** | 8.7 | 0.08 |
| Peri-oral, % | 11.4 | 7.8 | 0.25 | 7.8 | 0.38 | 8.7 | 0.34 |
| Laboratory features | |||||||
| Serum ACTH (pg/mL) | 44.6 | 42.9 | 0.03* | 45.4 | 0.402 | 40.3 | 0.087 |
| % of ACTH > 60 | 20.0 | 16.3 | 0.86 | 15.7 | 0.652 | 19.6 | 0.663 |
| Serum cortisol (μg/dL) | 14.1 | 7.7 | 0.02* | 7.8 | < 0.01** | 7.3 | < 0.01** |
| % of cortisol < 5 | 3.0 | 27.7 | < 0.01** | 26.2 | < 0.01** | 34.8 | < 0.01** |
| Other steroid forms and mixed steroid form use patients were not included for analysis due to low number of each form and heterogeneity in steroid usage history. *p < 0.05, **p < 0.01. |
|||||||
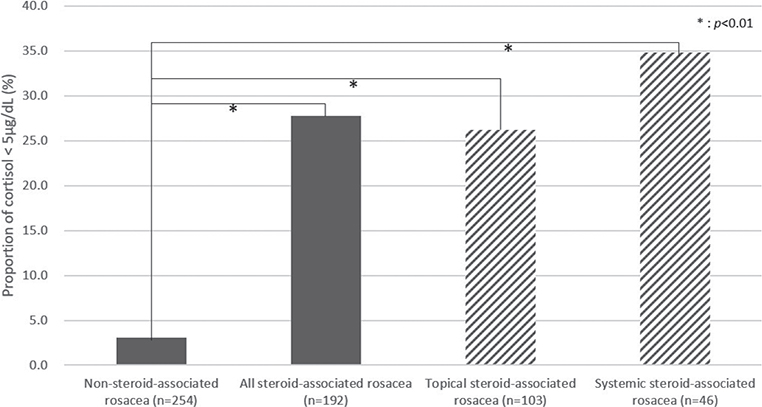
Fig. 1. Difference in proportion of patients with serum cortisol < 5 μg/dL according to rosacea groups.
DISCUSSION
Steroid-associated rosacea is characterized by a high prevalence of eyelid involvement and low serum cortisol levels, which serve as distinguishing features when compared with non-steroid-associated rosacea. Considering that topical steroid-associated rosacea also exhibits low serum cortisol levels, it is noteworthy that despite lower systemic absorption compared with systemic steroids, the continuous use of high-potency steroids increases the risk of secondary adrenal insufficiency (4, 7). Therefore, it can be speculated that both high potency and longer duration of use contribute to an elevated risk of rosacea development due to topical steroids. Frequent itching of periorbital skin and subsequent steroid application, as well as the thinness of the eyelid skin, may explain the clinical involvement observed (2, 8). When topical steroids are applied to the face, including the eyelids, direct exposure affects the facial skin, particularly due to the thinner stratum corneum and higher drug permeability of the eyelid skin, which may contribute to the characteristic occurrence of steroid-associated rosacea (9–11). Furthermore, in line with previous research findings, the cumulative dose and cumulative duration of topical steroid use are associated with the risk of developing diabetes (12). While this study is limited by its retrospective, single-institution design and the constraints of analysing a heterogeneous group with varied prior steroid usage, it stands as the initial examination of distinctive clinical and laboratory features in patients with steroid-associated rosacea. These findings should alarm dermatologists to suspect the history of topical steroid use in their patients and educate them regarding the risks associated with continued topical steroid use.
ACKNOWLEDGEMENT
Reviewed and approved by Seoul Metropolitan Government Seoul National University Boramae Medical Center (SMG-SNU) Institutional Review Board (No.30-2022-41)
REFERENCES
- Bhat YJ, Manzoor S, Qayoom S. Steroid-induced rosacea: a clinical study of 200 patients. Indian J Dermatol 2011; 56: 30–32.
- Ljubojeviae S, Basta-Juzbasiae A, Lipozenèiae J. Steroid dermatitis resembling rosacea: aetiopathogenesis and treatment. J Eur Acad Dermatol Venereol 2002; 16: 121–126.
- Souto EB, Fangueiro JF, Fernandes AR, Cano A, Sanchez-Lopez E, Garcia ML, et al. Physicochemical and biopharmaceutical aspects influencing skin permeation and role of SLN and NLC for skin drug delivery. Heliyon 2022; 8: e08938.
- Levin C, Maibach HI. Topical corticosteroid-induced adrenocortical insufficiency: clinical implications. Am J Clin Dermatol 2002; 3: 141–147.
- Hameed AF. Steroid dermatitis resembling rosacea: a clinical evaluation of 75 patients. ISRN Dermatology 2013; 2013: 491376.
- Rathi SK, Kumrah L. Topical corticosteroid-induced rosacea-like dermatitis: a clinical study of 110 cases. Indian J Dermatol Venereol Leprol 2011; 77: 42–46.
- AlQadri NG, Aljomah N, Alotaibi HM. Topical corticosteroid-induced adrenal insufficiency: a case report. Case Rep Dermatol 2022; 14: 39–42.
- Chopra K, Calva D, Sosin M, Tadisina KK, Banda A, De La Cruz C, et al. A comprehensive examination of topographic thickness of skin in the human face. Aesthet Surg J 2015; 35: 1007–1013.
- Neittaanmäki H, Kontkanen M, Kallioinen M. Skin atrophy of the eyelid induced by topical ophthalmic corticosteroids. Acta Ophthalmol Scand 1998; 76: 372–373.
- See GL, Sagesaka A, Sugasawa S, Todo H, Sugibayashi K. Eyelid skin as a potential site for drug delivery to conjunctiva and ocular tissues. Int J Pharm 2017; 533: 198–205.
- Emeriewen K, McAuley WJ, Beebeejaun MT, Cook MT, Saleh GM. The permeability of human eyelid skin to topically applied lidocaine. J Drug Deliv Sci Technol 2020; 55: 101357.
- Phan K, Smith SD. Topical corticosteroids and risk of diabetes mellitus: systematic review and meta-analysis. J Dermatolog Treat 2021; 32: 345–349.