ORIGINAL REPORT
Identifying Key Drivers in the Pathogenesis of Martorell Hypertensive Ischaemic Leg Ulcer: A Comparative Analysis with Chronic Venous Leg Ulcer
Jamila HESS1, Marjam-Jeanette BARYSCH-BONDERER1, Corsin SEELI1, Julia LAUBE1, Adhideb GHOSH2, Julia DEINSBERGER3, Benedikt WEBER3, Jürg HAFNER1 and Barbara MEIER-SCHIESSER1
1Department of Dermatology, University Hospital Zurich, Zurich, 2Functional Genomis Center, University of Zurich and ETH Zurich, Zurich, Switzerland, and 3Department of Dermatology, Medical University of Vienna, Vienna, Austria
Martorell hypertensive ischaemic leg ulcer (Martorell HYTILU) is a rare but significant cause of distal leg ulcers. Although hypertension and diabetes are known factors in its development, the precise pathogenesis of Martorell HYTILU remains elusive. To reach a better understanding of Martorell HYTILU, transcriptomic analysis was conducted through RNA sequencing and immunohistochemical comparison of Martorell HYTILU (n = 17) with chronic venous ulcers (n = 4) and healthy skin (n = 4). Gene expression analysis showed a marked activation of immune-related pathways in both Martorell HYTILU and chronic venous ulcers compared with healthy skin. Notably, neutrophil activity was substantially higher in Martorell HYTILU. While pathway analysis revealed a mild downregulation of several immune pathways in Martorell HYTILU compared with chronic venous ulcers, keratinization, cornification, and epidermis development were significantly upregulated in Martorell HYTILU. Additionally, STAC2, a gene encoding for a protein promoting the expression of the calcium channel Cav1.1, was significantly upregulated in Martorell HYTILU and was detected perivascularly in situ (Martorell HYTILU n = 24; chronic venous ulcers n = 9, healthy skin n = 11). The high expression of STAC2 in Martorell HYTILU suggests that increased calcium influx plays an important role in the pathogenesis of the disease. Consequently, calcium channel antagonists could be a promising treatment avenue for Martorell HYTILU.
Key words: Martorell hypertensive ischaemic leg ulcer; inflammation; STAC2.
SIGNIFICANCE
Martorell hypertensive ischaemic leg ulcer is a severe form of chronic leg ulcer with a vascular origin, characterized by arteriolosclerosis and medial calcinosis. While its exact pathophysiology remains unclear, our study analysed lesional skin using RNA sequencing and immunohistochemistry. Both Martorell hypertensive ischaemic leg ulcer and chronic venous ulcers share upregulated immune-related pathways compared with healthy skin. Martorell hypertensive ischaemic leg ulcer also exhibits heightened neutrophil activity and upregulation of STAC2, promoting calcium channel Cav1.1 expression. This suggests increased calcium influx in disease pathogenesis. We propose calcium channel antagonists as a potential treatment avenue for Martorell hypertensive ischaemic leg ulcer.
Citation: Acta Derm Venereol 2024; 104: adv40090. DOI https://doi.org/10.2340/actadv.v104.40090.
Copyright: © 2024 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Feb 12, 2024; Accepted: Apr 24, 2024; Published: May 30, 2024
Corr: Barbara Meier-Schiesser, Department of Dermatology, University Hospital Zurich, CH-8901 Zurich, Switzerland. E-mail: Barbara.Meier-Schiesser@usz.ch
Competing interests and funding: The authors have no conflict of interest to declare.
INTRODUCTION
Martorell hypertensive ischaemic leg ulcer (Martorell HYTILU) represents a manifestation of chronic leg ulcers of vascular origin. The condition is characterized by ischaemic subcutaneous arteriolosclerosis, leading to a swiftly progressing skin infarction typically localized on the laterodorsal lower leg and the Achilles tendon.
The ischaemic wound border is discerned by a violaceous hue and an undermined appearance. Individuals afflicted by Martorell HYTILU endure intense pain, disrupted sleep, and a pervasive sense of exhaustion (1–3). Histological examination reveals subcutaneous arterioles exhibiting thickened walls, often at the expense of a narrow lumen. Hallmarks include diminished cellularity manifesting as a paucity of smooth muscle cell nuclei and subendothelial hyalinosis. Notably, a distinctive form of medial calcification is evident in three-quarters of histology slides (3). The mean age of onset is 74.5 years and all afflicted patients are affected by hypertension, which is, however, usually well controlled (2). Additionally, on average, 58% of the patients suffer from diabetes (3).
The management of Martorell HYTILU necessitates a multidisciplinary approach, encompassing optimal control of underlying diabetes and hypertension, pain management, and wound care such as debridement of necrotic material and split-thickness skin grafts (4–7).
Pathogenetically, it is hypothesized that chronic hypertension induces stenosing arteriolosclerosis, typically characterized by a narrowed vessel lumen and thickened vessel walls (medial hyperplasia). This process compromises skin perfusion, ultimately resulting in skin infarction. Subsequent tissue hypoxia triggers the release of proinflammatory cytokines and favours the proliferation of smooth vessel muscles, which promotes arteriolosclerosis. Additionally, inflammation, particularly involving neutrophils, has been demonstrated to play a significant role (4). The medial calcinosis of the subcutaneous arterioles might be due to an increased transfer of calcium during this inflammatory process. However, a precise understanding of the pathomechanisms leading to Martorell HYTILU is missing to date.
The differential diagnosis for Martorell HYTILU includes other forms of vascular leg ulcers and other atypical leg ulcers. In this study, the lesional skin from Martorell HYTILU and chronic venous leg ulcers – the most common type of chronic leg ulcer – as well as healthy skin, were compared at gene expression and histological levels. A better understanding of the distinct characteristics of both diseases will assist healthcare professionals in accurately diagnosing and differentiating between the two conditions and ultimately optimizing therapeutic interventions. This, in turn, will lead to more appropriate treatment plans and improved patient outcomes.
MATERIALS AND METHODS
Patient cohort and sampling
Patients with Martorell HYTILU and chronic venous leg ulcers were diagnosed via medical history, clinical evaluation, and histology. Healthy skin samples were taken from lower legs of patients undergoing surgery for other indications; no tumorous or inflammatory tissue was included. Skin samples taken between 2012 and 2021 at the Department of Dermatology of the University Hospital Zurich were included in this study (Table I). All human samples were collected after informed written patient consent and according to the principles of Helsinki with approval of the ethics committee. Biopsies were taken from lesional skin (ulcers) or healthy non-diseased skin as control.
Immunohistochemical staining
Paraffin-embedded skin sections from 24 Martorell HYTILU, 9 venous leg ulcers, and 11 healthy individuals were included. Immunohistochemistry was performed using antibodies targeting myeloperoxidase (MPO; Agilent, Santa Clara, CA, US), CD3 (DAKO; Carpinteria, CA, US), CD68 (DAKO; Carpinteria, CA, US), and STAC2 (LS Bio, Seattle, Washington, US). Paraffin-embedded skin sections underwent deparaffinization and rehydration. To expose antigens, the slides were subjected to 25 minutes of heating using Target Retrieval solution (DAKO). Following a 1-hour blockage with 5% BSA in PBS, the sections were incubated with anti-MPO, anti-CD3, anti-CD68, and anti-STAC2 antibodies. Primary antibodies were identified using a biotin-streptavidin secondary antibody and positivity was visualized by an AEC chromogen substrate (Abcam, Cambridge, UK). Haematoxylin solution was used to counterstain. After fixation with DAKO mounting medium, the slides were scanned using ScanScope (Leica Biosystems, Wetzlar, Germany), and semi-quantification was performed using the Aperio ImageScope software (Leica Biosystem).
RNA isolation and sequencing
Biopsies from 17 Martorell HYTILU, 4 venous leg ulcers, and 4 healthy individuals were taken under sterile conditions and stored in RNA later at –20°C. Samples were unthawed and RNA was extracted using TRizol in combination with the Qiagen RNeasy kit (https://www.qiagen.com/us) following the manufacturer’s instructions. For RNA sequencing, total RNA (100–1,000 ng/per sample) was depleted with ribosomal RNA, reverse-transcribed into double-stranded cDNA and selectively enriched with polymerase chain reaction (PCR). The quality and quantity of the enriched libraries were validated using the Fragment Analyzer (Agilent, Santa Clara, CA, USA). The libraries were normalized to 10nM in Tris-Cl 10 mM, pH 8.5 with 0.1% Tween 20. Novaseq 6000 (Illumina Inc, San Diego, CA, USA) was used for cluster generation and sequencing according to standard protocol. Raw sequencing data was processed using the SUSHI framework developed at the Functional Genomics Center Zurich (FGCZ). Low-quality reads and adapters were trimmed off using fastp v0.20 (8). Filtered reads were pseudo-aligned against the human reference genome assembly GRCh38.p13 and gene expression level was quantified using Kallisto v0.46.1 (9). Differential gene expression analysis was performed between different conditions using the R package edgeR v3.36 (10). Gene set enrichment analysis was performed using the R package clusterProfiler v4.8.1 (11) based on the gene ontology biological process terms.
RESULTS
Majority of genes are downregulated in Martorell HYTILU compared with chronic venous leg ulcers
To study possible differences in the gene expression pattern of Martorell HYTILU, chronic venous leg ulcers, and healthy skin, a bulk RNA sequencing analysis of lesional ulcer and healthy skin was performed. Hierarchical cluster analysis of the 2,000 most variable genes across all samples revealed a clear clustering of the healthy skin samples, whereas Martorell HYTILU samples clustered partially with chronic venous leg ulcers, as illustrated by a heat-map (Fig. 1).
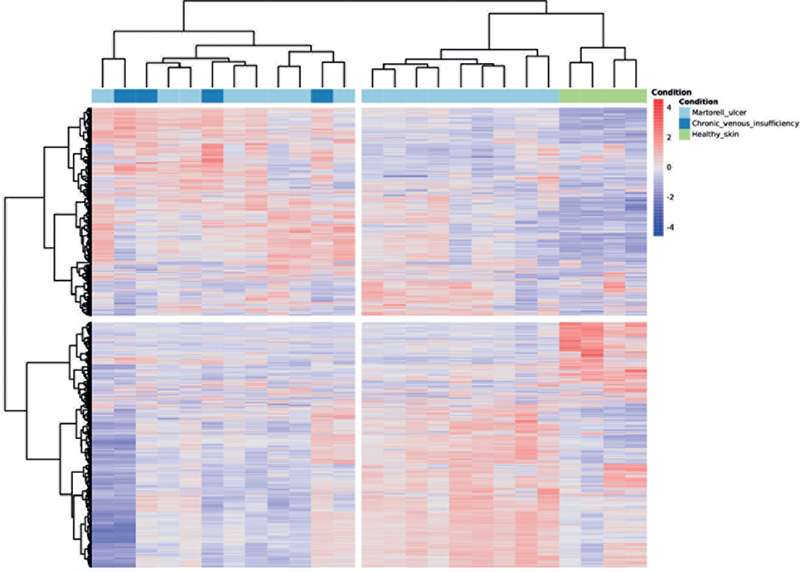
Fig. 1. Comparison of gene expression patterns in Martorell HYTILU, CVU, and healthy skin. Heatmap illustrating hierarchical clustering of lesional (Martorell HYTILU and CVU) and healthy skin samples displaying the gene expression profiles across samples. Rows representing genes and columns representing individual samples. The intensity of colour represents the relative expression levels of genes (red = high expression; blue = low expression). Clustering algorithms were applied to group similar samples based on their gene expression patterns.
A total of 1,669 significantly differentially expressed genes (|log2| > 1.5; p-value < 0.05) were detected between Martorell HYTILU and healthy skin (Fig. 2A), and 2,088 differently significantly expressed genes (|log2| > 1.5; p-value < 0.05) between chronic venous leg ulcers and healthy skin. Notably (Fig. 2B), only 280 genes were significantly differentially expressed between Martorell HYTILU and chronic venous leg ulcers (|log2| > 1.5; p-value < 0.05) (Fig. 2C). When comparing Martorell HYTILU with healthy skin, both upregulated and downregulated genes could be detected with a higher portion of downregulated genes (Fig. 2A). In contrast, more upregulated genes were detected in CVU in comparison with healthy skin (Fig. 2B). Interestingly, the comparison of Martorell HYTILU and CVU revealed that the vast majority of genes were downregulated in Martorell HYTILU compared with CVU (196/280 genes; Fig. 2C).

Fig. 2. Illustration of up- and downregulated genes in Martorell HYTILU, CVU and hs. Volcano plot demonstrating the upregulated and downregulated genes when comparing Martorell HYTILU over hs (A), CVU over HS (B) and Martorell over CVU (C). The volcano plot depicts Log2 fold change (cut off: Log2 0.5, p-value 0.05) on the x-axis and – log10p p-value on the y-axis. Single genes are depicted as dots. Upregulated genes are illustrested in Red, downregulated genes in Blue. HYTILU: hypertensive ischaemic leg ulcer; CVU: chronic venous ulcer, hs: healthy skin.
Transcriptional differences between Martorell HYTILU and chronic venous leg ulcers
Even though the majority of genes turned out to be downregulated in Martorell HYTILU compared with CVU, we were interested in classifying upregulated genes in Martorell HYTILU. We found elevated levels of a metalloproteinase (MMP7), which is known for its catalytic activity leading to tissue destruction. Furthermore, genes related to lipid metabolism (FABP4; ABCA9; APOD; ANGPTL4; PLIN2; LIPE) and glucose metabolism (PPP1R1; PCSK1; PDK4) were upregulated in Martorell HYTILU compared with CVU (12). Conversely, the vast majority of genes upregulated in CVU in comparison with Martorell HYTILU were coding for immunoglobulin light and heavy chains (Fig. 3C), indicative of persistent inflammation.

Fig. 3. Top upregulated genes in Martorell HYTILU and CVU. Heatmap illustrating illustrating top 50 upregulated genes when comparing Martorell HYTILU over hs (A), Martorell HYTILU over CVU (B) and CVU over Martorell HYTILU (cut-off: log2 fold: 1.5, p-value=0.05). Rows represent top 50 genes and columns represent individual samples. The intensity of colours represents the relative expression levels of genes (Red = high expression; Blue = low expression). HYTILU: hypertensive ischaemic leg ulcer; CVU: chronic venous ulcer, hs: healthy skin
Keratinization, cornification, and epidermis development represent predominant pathways in Martorell HYTILU compared with chronic venous leg ulcers
To put the gene expression pattern into a biological context, a gene set enrichment analysis was performed. Compared with healthy skin, both Martorell HYTILU and CVU show upregulated immune-related and angiogenesis-related pathways. Moreover, keratinization was elevated in Martorell HYTILU compared with healthy skin and this has not been detected in CVU (Fig. 4A, B). The direct comparison of Martorell HYTILU and CVU revealed a significant upregulation of genes related to keratinization, cornification, and epidermis development in Martorell HYTILU (Fig. 4C).

Fig. 4. Analysis of prominent biological pathways in Martorell HYTILU and CVU. A value inferior to zero on the x-axis indicates a downregulation of the indicated biological pathway and superior to zero indicates an upregulation of the indicated biological pathway. The most relevant biological pathways are listed on the y-axis. HYTILU: hypertensive ischaemic leg ulcer; CVU: chronic venous ulcer, hs: healthy skin.
Upregulation of neutrophil pathways and distinct distribution pattern in Martorell HYTILU
The gene set enrichment analysis revealed that in both Martorell HYTILU and chronic venous leg ulcers some biological pathways related to neutrophils were upregulated compared with healthy skin. Specific to Martorell HYTILU was an elevated neutrophil chemotaxis through the upregulation of S100A8, S100A9, S100A12, PDE4N, CCL23, and CD300H (12). Three of these genes also encode calcium-binding proteins (S100A8, S100A9, S100A12). Calcium-binding proteins are, among other things, known for their role in cytokine production, chemotaxis, and increased oxidative stress through toll-like receptors (TLR). An upregulated neutrophil degranulation has been detected in both ulcer groups. However, the neutrophil degranulation was higher in the case of Martorell HYTILU, with 165 upregulated genes versus 110 upregulated genes for chronic venous leg ulcers. A predominance of neutrophils both in Martorell HYTILU and in CVU could be confirmed on the protein level in situ by immunohistochemistry using an antibody against myeloperoxidase (MPO). A difference could be seen in the distribution of cells: while neutrophils are located mainly in the upper dermis in CVU, they are highly present throughout the whole skin and periarteriolar in Martorell HYTILU (Fig. 5A, B).

Fig. 5. Marker expression in Martorell HYTILU, CVU and hs in situ. Immunohistochemistry stainings with antibodies against myeloperoxidase, MGP, Osteopontin, BMP2 and STAC2. Representative stainings of meloperoxidase in lesional skin of Martorell HYTILU (A) and CVU (B). Semi-quantification MGP, Osteopontin and BMP2 represented as percentage of endothelial cells (C). Representative staining of lesional Martorell HYTILU skin (D), semi-quantification illustrated by staining intensity (E). HYTILU: hypertensive ischaemic leg ulcer; CVU: chronic venous ulcer, hs: healthy skin.
STAC2 is a potential driver of calcification in Martorell HYTILU
Specific genes and proteins are known to play a role in the pathophysiology of diseases with association with dysregulated calcification of vessels. Counted among these are MGP1, BMP2, or osteopontin (13–15). Notably, none of these genes were found to be differentially regulated in Martorell HYTILU compared with chronic venous leg ulcers or healthy skin in our bulk RNAseq analysis. This finding could be confirmed by immunohistochemistry staining for BMP2 and osteopontin, which revealed no significant increase or decrease in Martorell HYTILU’s vessels compared with CVU. MGP1 expression was significantly higher in Martorell HYTILU compared with CVU and healthy skin, indicating a post-transcriptional regulation of the protein (Fig. 5C).
On the contrary, STAC2, a gene coding for a protein that has been shown to regulate calcium channel inactivation (16, 17), was upregulated in Martorell HYTILU compared with CVU (log2 ratio 2.1983; p = 0.0119) (Fig. 4B). To confirm these findings on the protein level and to identify the location of STAC2 in situ, immunohistochemical staining was performed showing that STAC2 was mainly detected perivascularly (Fig. 5D, E).
DISCUSSION
Martorell HYTILU, a rare yet severe complication of uncontrolled hypertension, manifests as painful leg ulcers (4–7). Although the involvement of neutrophils in the disease’s development has been identified (4), the precise underlying pathomechanism remains elusive. To improve understanding of the physiopathology of Martorell HYTILU, a comparison of Martorell HYTILU and CVU, the most common form of chronic leg ulcer, was performed using bulk RNA sequencing and immunohistochemistry.
Significant differences in gene expression profiles between Martorell HYTILU and healthy skin have been observed. However, notable similarities in gene expression between Martorell HYTILU and chronic venous leg ulcers (CVU) have also been detected. This suggests the possibility of a concomitant CVU in patients with Martorell HYTILU.
Enhanced angiogenesis has been observed in both Martorell HYTILU and chronic venous leg ulcers, despite the lack of corresponding clinical manifestations. This phenomenon could suggest an endeavour towards repair (18); however, it seems insufficient to counterbalance the high levels of inflammation and necrosis. In instances of chronic venous insufficiency, microangiopathy is already recognized as a characteristic feature (19). Furthermore, in Martorell HYTILU, the metabolism of retinol, lipids, and glucose was found to be upregulated compared with chronic venous ulcers (CVU). The increased activity in retinol metabolism likely indicates stimulation of epithelial growth, granulation tissue formation, and angiogenesis (20). The heightened lipid and glucose metabolism may be associated with underlying diabetes.
The upregulation of matrix metalloproteinases (MMPs), particularly MMP7 and MMP19, was noted in Martorell HYTILU, suggesting that tissue destruction in Martorell HYTILU is partially due to MMPs and their catalytic mechanisms. In CVU, high MMP expression is linked to increased inflammation and early venous dilation. As compression therapy has been shown to be effective in reducing MMPs in CVU (21), it could be a viable treatment for Martorell HYTILU patients with concomitant chronic venous insufficiency. However, conventional compression may be painful for these patients, making intermittent pneumatic compression a preferable alternative due to its comfort and effectiveness in improving microcirculation (22).
Martorell HYTILU and chronic venous leg ulcers share a significant upregulation of immune pathways and infiltration, compared with healthy skin.
Central to this process are neutrophils, which play a key role, as evidenced by increased neutrophil chemotaxis and degranulation. These changes mirror the clinical features of Martorell HYTILU, particularly the extensive tissue damage. Furthermore, immunohistochemistry staining revealed a notable difference in neutrophil distribution between Martorell HYTILU and chronic venous leg ulcers. To our best knowledge, this difference in neutrophil localization in the skin has not been described to date.
Martorell HYTILU exhibits a significant downregulation of various immunoglobulins and immunoglobulin chains compared with chronic venous ulcers (CVU). This difference may be attributed to the differing temporal progression of the two conditions. Martorell HYTILU typically develops suddenly and progresses quickly, mainly involving elements of the innate immune response. Conversely, CVU develops gradually, facilitating a more pronounced involvement of the adaptive immune system. In conventional wound healing, the presence of immunoglobulins usually indicates enhanced healing (23). However, this principle does not apply to CVU, where accumulation of immunoglobulin at the wound site may exacerbate the inflammation rather than promoting wound healing.
This variance in immunoglobulin expression between Martorell HYTILU and CVU suggests distinct immune mechanisms underlying these conditions. Peschen et al. demonstrated that the activation of ICAM-1 and VCAM-1 on endothelial cells leads to lymphocyte infiltration in chronic venous insufficiency (24). This infiltration, likely including active plasmocytes, may contribute to immunoglobulin accumulation at the wound’s periphery. While the study did not find a marked increase in anti-CD30 staining in CVU compared with Martorell HYTILU, it did not specifically examine the presence of plasmocytes.
Gene set enrichment analysis revealed a notable increase in keratinization, cornification, and epidermal proliferation in Martorell HYTILU compared with chronic venous leg ulcers (CVU). Given the significantly faster onset of Martorell HYTILU, a decrease in these pathways might be expected (21). However, their upregulation could be due to a higher rate of cellular turnover in Martorell HYTILU compared with CVU. Despite this, the chronic nature and difficult healing process of Martorell HYTILU suggest that this increased turnover is still inadequate. In contrast, CVU undergoes a perpetual cycle of cell regeneration and immediate destruction caused by inflammation (25). This could lead to increased cellular senescence, possibly accounting for the reduced keratinization, cornification, and epidermal proliferation observed in CVU (26).
Calcific arteriolosclerosis is commonly observed in Martorell HYTILU, yet its precise role remains unclear (27). Interestingly, there is an upsurge in Matrix Gla protein (MGP1) expression in Martorell HYTILU, a known inhibitor of vascular calcification. This could indicate a compensatory response against calcification. However, as suggested by Nigwekar et al. (13), the uncarboxylated form of MGP1, which requires vitamin K-dependent carboxylation for activation, might potentially contribute to increased vascular calcification in these cases. The observed upregulation of uncarboxylated MGP1 in Martorell HYTILU might contribute to the increased vascular calcification seen in these cases. While genes like BMP2 and osteopontin, known for their roles in calcification (14, 15), were not significantly altered, STAC2 showed notable upregulation. STAC2, a gene located on chromosome 17, encodes a protein found in various tissues including the skin, brain, and retina. It belongs to the SH3 and Cysteine Rich Domain (STAC) protein family, comprising STAC1, STAC2, and STAC3. These proteins enhance the activity of the calcium channel Cav1.1 and reduce the inactivation rate of Cav1.2 (16). The role of L-type calcium channel isoforms in hypertension, and their management through calcium channel blockers, is well-documented. Wong King Yuen et al. (17) highlighted STAC proteins’ crucial role in skeletal muscle contraction via the Cav1.1 channel and in decreasing the inactivation rate of Cav1.2 through STAC2 and STAC3. Cav1.1 is primarily found in the heart, whereas Cav1.2 is present in smooth muscle, pancreatic cells, fibroblasts, and neurons. Notably, Cav1.2 has been linked to aortic valve calcification (28, 29).
In our study, the localization of STAC2 was demonstrated to be perivascular. This suggests that increased calcium influx through Cav1.2 might lead to medial calcinosis in the subcutaneous arterioles, a common finding in Martorell HYTILU. Additionally, the degradation of elastic fibres seems to cause calcium phosphate salt deposits, resulting in microscopic calcification (30). This indicates that medial calcification might be a secondary effect, known as dystrophic calcification. The upregulation of STAC2 might explain why only a small proportion of patients with diabetes and arterial hypertension develop Martorell HYTILU. A noteworthy consideration is the potential use of calcium channel antagonists in treating Martorell HYTILU. These drugs are key in managing hypertension and may reduce the risk of developing Martorell HYTILU. They might also help by blocking CaV1.2, potentially decreasing medial calcinosis in the arterioles. On the other hand, calcium channel antagonists are known to facilitate peripheral oedema. Therefore, patients could benefit from concomitant compression therapy. However, these hypotheses need to be validated through clinical studies.
The study encountered several limitations that warrant discussion. First, variations in sample sizes across different groups may introduce biases and compromise the robustness of the findings. Moreover, the study is solely descriptive and does not provide detailed pathomechanistic insights through functional experiments.
In conclusion, our study identified STAC2 as a potential driver of calcification in Martorell HYTILU. The use of calcium channel antagonists represents a promising treatment strategy for the underlying hypertension and the reduction of arteriole calcification. This insight could pave the way for more effective treatments for this challenging condition.
ACKNOWLEDGEMENT
This work was supported by the Bruno Bloch foundation.
REFERENCES
- Glutz von Blotzheim L, Tanner FC, Noll G, Brock M, Fischler M, Hafner J, et al. Pulmonary hypertension in patients with Martorell hypertensive leg ulcer: a case control study. Respir Res 2012; 13: 45.
- Alavi A, Mayer D, Hafner J, Sibbald RG. Martorell hypertensive ischemic leg ulcer: an underdiagnosed Entity©. Adv Skin Wound Care 2012; 25: 563–574.
- Deinsberger J, Brugger J, Tschandl P, Meier-Schiesser B, Anzengruber F, Bossart S, et al. Differentiating arteriolosclerotic ulcers of Martorell from other types of leg ulcers based on vascular histomorphology. Acta Derm Venereol 2021; 101: adv00449.
- Hafner J, Nobbe S, Partsch H, Läuchli S, Mayer D, Amann-Vesti B, et al. Martorell hypertensive ischemic leg ulcer: a model of ischemic subcutaneous arteriolosclerosis. Arch Dermatol 2010; 146: 961–968.
- Deinsberger J, Sirovina S, Bromberger S, Böhler K, Vychytil A, Meier-Schiesser B, et al. Microstructural comparative analysis of calcification patterns in calciphylaxis versus arteriolosclerotic ulcer of Martorell. Eur J Dermatol 2021; 31: 705–711.
- Deinsberger J, Felhofer M, Kläger JP, Petzelbauer P, Gierlinger N, Weber B. Raman spectroscopy reveals collagen and phospholipids as major components of hyalinosis in the arteriolosclerotic ulcer of Martorell. J Eur Acad Dermatol Venereol 2021; 35: 2308–2316.
- Weber B, Deinsberger J, Hafner J, Beltraminelli H, Tzaneva S, Böhler K. Localization-mapping of arteriolosclerotic ulcers of Martorell using two-dimensional computational rendering reveals a predominant location on the mid-lateral lower leg. J Eur Acad Dermatol Venereol 2021; 35: e40–e42.
- Chen S, Zhou Y, Chen Y, Gu J. fastp: an ultra-fast all-in-one FASTQ preprocessor. Bioinformatics 2018; 34: i884–i890.
- Bray NL, Pimentel H, Melsted P, Pachter L. Erratum: Near-optimal probabilistic RNA-seq quantification. Nat Biotechnol 2016; 34: 525–>527. Erratum in: Nat Biotechnol 2016; 34: 888.
- Robinson MD, McCarthy DJ, Smyth GK. edgeR: a Bioconductor package for differential expression analysis of digital gene expression data. Bioinformatics 2010; 26:139–140.
- Wu T, Hu E, Xu S, Chen M, Guo P, Dai Z, et al. clusterProfiler 4.0: aA universal enrichment tool for interpreting omics data. Innovation (Camb) 2021; 2: 100141.
- GeneCards – The human gene database (Internet). Rehovot, Israel: Crown Human Genome Center & Weizmann Institute of Science; 2002 [last accessed August 2022]. Available from: https://www.genecards.org/.
- Nigwekar SU, Bloch DB, Nazarian RM, Vermeer C, Booth SL, Xu D, et al. Vitamin K-dependent carboxylation of matrix Gla protein influences the risk of calciphylaxis. J Am Soc Nephrol 2017; 28: 1717–1722.
- Li X, Yang HY, Giachelli CM. BMP-2 promotes phosphate uptake, phenotypic modulation, and calcification of human vascular smooth muscle cells. Atherosclerosis 2008; 199: 271–277.
- Cho HJ, Cho HJ, Kim HS. Osteopontin: a multifunctional protein at the crossroads of inflammation, atherosclerosis, and vascular calcification. Curr Atheroscler Rep 2009; 11: 206–213.
- Campiglio M, Costé de Bagneaux P, Ortner NJ, Tuluc P, Van Petegem F, Flucher BE. STAC proteins associate to the IQ domain of CaV1.2 and inhibit calcium-dependent inactivation. Proc Natl Acad Sci U S A 2018; 115: 1376–1381.
- Wong King Yuen SM, Campiglio M, Tung CC, Flucher BE, Van Petegem F. Structural insights into binding of STAC proteins to voltage-gated calcium channels. Proc Natl Acad Sci U S A 2017; 114: E9520–E9528.
- Veith AP, Henderson K, Spencer A, Silgar AD, Baker AB. Therapeutic strategies for enhancing angiogenesis in wound healing. Adv Drug Deliv Rev 2019; 146: 97–125.
- Jünger M, Steins A, Hahn M, Häfner HM. Microcirculatory dysfunction in chronic venous insufficiency (CVI). Microcirculation 2000; 7: 3–12.
- Zinder R, Cooley R, Vlad LG, Molnar JA. Vitamin A and wound healing. Nutr Clin Pract 2019; 34: 839–849.
- Raffetto JD. Pathophysiology of chronic venous disease and venous ulcers. Surg Clin North Am 2018; 98: 337–347.
- Liu K, Chen LE, Seaber AV, Johnson GW, Urbaniak JR. Intermittent pneumatic compression of legs increases microcirculation in distant skeletal muscle. J Orthop Res 1999; 17: 88–95.
- Nishio N, Ito S, Suzuki H, Isobe KI. Antibodies to wounded tissue enhance cutaneous wound healing. Immunology 2009; 128: 369–380.
- Peschen M, Lahaye T, Hennig B, Weyl A, Simon JC, Vanscheidt W. Expression of the adhesion molecules ICAM-1, VCAM-1, LFA-1 and VLA-4 in the skin is modulated in progressing stages of chronic venous insufficiency. Acta Derm Venereol 1999; 79: 27–32.
- Martin P, Nunan R. Cellular and molecular mechanisms of repair in acute and chronic wound healing. Br J Dermatol 2015;173: 370–378.
- Deo PN, Deshmukh R. Pathophysiology of keratinization. J Oral Maxillofac Pathol 2018; 22: 86–91.
- Monfort JB, Cury K, Moguelet P, Chasset F, Bachmeyer C, Francès C, et al. Cutaneous arteriolosclerosis is not specific to ischemic hypertensive leg ulcers. Dermatology 2018; 234: 194–197.
- Matsui M, Bouchareb R, Storto M, Hussain Y, Gregg A, Marx SO, et al. Increased Ca2+ influx through CaV1.2 drives aortic valve calcification. JCI Insight 2022; 7:e155569.
- Guauque-Olarte S, Messika-Zeitoun D, Droit A, Lamontagne M, Tremblay-Marchand J, Lavoie-Charland E, et al. Calcium signaling pathway genes RUNX2 and CACNA1C are associated with calcific aortic valve disease. Circ Cardiovasc Genet 2015; 8: 812–822.
- Enoch S, Kupitz S, Miller DR, Harding KG. Dystrophic calcification as a cause for non healing leg ulcers. Int Wound J 2005; 2: 142–147.