SHORT COMMUNICATION
Treatment of Metophyma with Isotretinoin
Stefano VERALDI1* and Giulia MURGIA2
1Dermatological Centre in Milan, Milan, Italy, 2Department of Pathophysiology and Transplantation, Università degli Studi, IRCCS Foundation, Ca’ Granda Ospedale Maggiore Policlinico, Milan, Italy. *E-mail: stefano.veraldi@dcim.it
Citation: Acta Derm Venereol 2024; 104: adv40101. DOI: https://doi.org/10.2340/actadv.v104.40101.
Copyright: © 2024 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Feb 12, 2024; Accepted: May 21, 2024; Published: Jun 20, 2024.
INTRODUCTION
Metophyma is an extremely rare clinical variety of phyma located on the forehead. Other phymas can involve the ears (otophyma, unilaterally or bilaterally), eyelids (blepharophyma, unilaterally or bilaterally), nose (rhinophyma), and the chin (gnatophyma). Rhinophyma is by far the commonest variety of phyma (1). We report a patient with severe metophyma who was treated with oral isotretinoin, with satisfactory, although partial, clinical results.
CASE REPORT
A 27-year-old Caucasian man was admitted because of a swelling located on the forehead. The patient stated that he had been affected by acne from the age of 18 to 22 years. He was successfully treated with topical and oral antibiotics and topical retinoids. The swelling appeared at the age of 25 years and was unsuccessfully treated with oral antibiotics, non-steroidal anti-inflammatory drugs, and corticosteroids. The patient complained of mild itching and a burning sensation. Dermatological examination showed a large erythematous swelling located on the forehead. The surface was irregular because of the presence of small papules and pustules (Fig. 1). Consistency of the lesion was parenchymatous-hard. General physical examination was negative. All laboratory tests were within normal limits. Urea breath test for Helicobacter pylori was negative. The search for Demodex folliculorum was negative.
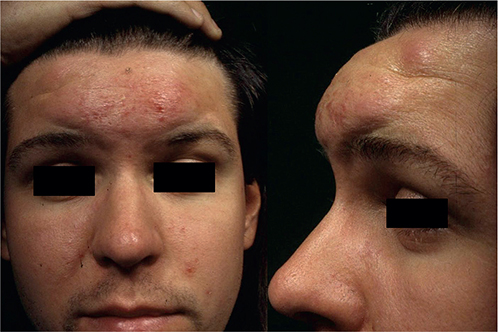
Fig. 1. Severe erythematous swelling on the forehead. Written permission has been given to publish these images.
In consideration of the clinical picture (chronic erythematous swelling located on the forehead, accompanied by mild symptoms), we made a diagnosis of metophyma and suggested a biopsy; however, the patient refused (he stated: “The biopsy scar can further worsen the appearance of my forehead”). The patient was therefore treated with oral isotretinoin (0.5 mg/kg/day for 6 months). A significant reduction of erythema and oedema was observed approximately 6 weeks after the beginning of therapy. Final clinical results are reported in Fig. 2. During the therapy, the patient complained of skin dryness, cheilitis, mild epistaxis, and mild arthralgia: however, it was not necessary to stop the therapy or reduce the dosage. No laboratories abnormalities were detected. Follow-up (at 24 months) was negative.

Fig. 2. Partial remission of erythema and oedema after 6 months of therapy with isotretinoin (0.5 mg/kg/day). Written permission has been given to publish these images.
DISCUSSION
We were able to find only 4 cases of metophyma in the international literature (2–5). The patient described by Chan et al. showed an atypical clinical presentation of metophyma: a large nodule in the centre of the forehead. Histopathological examination showed distended pilosebaceous units, abundant fibrovascular tissue, and a lymphohistiocytic infiltrate around dilated blood vessels (2). The patient reported by Rai and Madan was previously treated with isotretinoin, with reduction of sebaceous gland hyperplasia, but no effect on the phyma. This patient was subsequently treated with carbon dioxide laser (3). This laser was successfully used in another patient with metophyma (5). Er:YAG and pulsed dye laser, surgical excision, cryosurgery, and dermabrasion can also be taken into consideration in phymatous rosacea (5).
In conclusion, we report a patient with severe metophyma who was treated with isotretinoin, with satisfactory, although partial, clinical results.
REFERENCES
- Jansen T, Plewig G. Clinical and histological variants of rhinophyma, including nonsurgical treatment modalities. Facial Plast Surg 1998; 14: 241–253.
- Chan JL, Soliman S, Miner AG, Hughes SM, Cockerell CJ, Perone JB. Metophyma: case report and review of a rare phyma variant. Dermatol Surg 2011; 37: 867–869.
- Rai S, Madan V. Treatment of metophyma with the carbon dioxide laser. Dermatol Surg 2012; 38: 513–515.
- Abdalhafid El-Sherif N, Abdalsalam El-Dibany S. Clinical evaluation of Libyan patients with rosacea and its correlation with seropositivity to Helicobacter pylori. J Dermatol Dermatol Surg 2014; 18: 13–16.
- Weinkle AP, Doktor V, Emer J. Update on the management of rosacea. Clin Cosmet Invest Dermatol 2015; 8: 159–177.