SHORT COMMUNICATION
Majocchi’s Granuloma with Epidermal Cysts due to Trichophyton rubrum: Ultrastructural Observations
Naomi TANI1*, Nanako YAMADA1, Kazushi ANZAWA2, Takashi MOCHIZUKI2 and Osamu YAMAMOTO1
1Division of Dermatology, Department of Medicine of Sensory and Motor Organs, Faculty of Medicine, Tottori University, 86 Nishi-cho, Yonago, Tottori 683-8504, Japan, and 2Department of Dermatology, Kanazawa Medical University, Ishikawa, Japan. *E-mail: taninaomi@tottori-u.ac.jp
Citation: Acta Derm Venereol 2024; 104: adv40148. DOI https://doi.org/10.2340/actadv.v104.40148.
Copyright: 2024 © The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Feb 21, 2024; Accepted after review: Aug 12, 2024; Published: Sep 15, 2024
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Majocchi’s granuloma is a rare fungal infection in the dermis or deep tissue that is mainly caused by dermatophytes (1–3). In this study, we report a case of Majocchi’s granuloma due to Trichophyton rubrum accompanied by epidermal cysts, with a focus on ultrastructural observations.
CASE REPORT
An 85-year-old woman with a 10-month history of multiple facial nodules was referred to us. She was taking prednisolone (5 mg/day) for systemic lupus erythematosus. She had previously been administered topical steroids to treat facial skin lesions. Physical examination revealed multiple nodules on the forehead, upper eyelid, buccal region, and lower jaw (Fig. 1A–B). The histopathology of a biopsied specimen obtained from the right temple showed an abscess in the deep dermis (Fig. 1C). Part of torn hair was observed in the abscess, and fungal elements were observed within the hair shaft. Periodic acid-Schiff (PAS) staining revealed branching septate hyphae within and around the hair shafts (Fig. 1D). A cystic structure was also observed (Fig. 1E). The orifice of the cyst was opened at the skin surface and the lumen of the cyst was filled with keratinized materials and fragmented hair shafts. Grocott staining revealed many hyphae in the keratinized material and horny cells in the epithelium of the cyst (Fig. 1E). Three other nodules on the upper eyelid were surgically removed at the request of the patient. Histopathological examination of 2 of the 3 specimens revealed epidermal cysts in the dermis (Fig. 1F). There were keratin materials with Grocott-positive septate hyphae in the epidermal cysts (Fig. 1G). Granulomas containing multinucleated giant cells were observed near the cysts. These cells phagocytized the PAS-positive septate hyphae (Fig. 1H). Another specimen showed keratin surrounded by aggregated neutrophils in the deep dermis. Hyphae were observed in the keratin materials. Transmission electron microscopy (TEM) of the lesion on the right upper eyelid revealed fungal hyphae in histocytes (Fig. 2A). The fungal hyphae had a 160-nm-thick cell wall that maintained its laminated structure. Organelles and rough endoplasmic reticulum (rER) were observed in the cytoplasm (Fig. 2B). Microscopic examination of the interdigital scales revealed the presence of filamentous fungi. We performed fungal cultures using 3 biopsy specimens from the upper eyelid and interdigital scales. All 4 cultures resulted in the formation of a white cottony colony on the surface (KMU 10705, 10706, 10707, and 10708) after 2 weeks of incubation on Sabouraud dextrose agar at 27°C (Fig. 2C). Sequence analysis of the internal transcribed spacer (ITS) regions of the ribosomal DNA genes of all 4 cultures (KMU 10705, 10706, 10707, and 10708) was performed using BLAST in GenBank. The fungus was identified as T. rubrum. Based on these findings, we diagnosed Majocchi’s granuloma due to T. rubrum infection in an immunosuppressed patient. Oral administration of terbinafine (125 mg/day) was initiated. Seven weeks later, the nodules on the face had almost disappeared, and 2 nodules remained on the upper eyelid. The remaining nodules were resected. Histopathological examination of both nodules revealed ruptured epidermal cysts, containing keratin in the dermis. PAS-positive septate hyphae were detected in the multinucleated giant cells of granuloma around the cysts and in the keratin materials in the cysts. Terbinafine was then administered for 12 weeks. No recurrence was observed during the observation period.
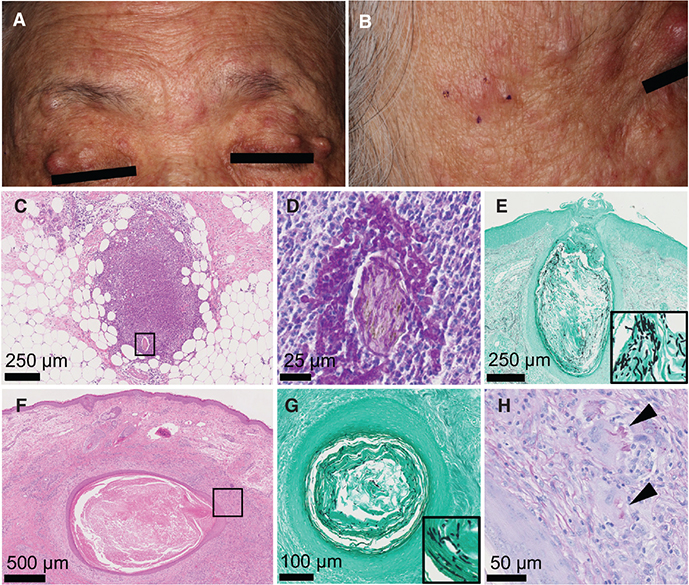
Fig. 1. Clinical and histological findings. (A, B) Multiple papules and nodules on the forehead, upper eyelid, and buccal region at the first visit. (C) Abscess around the hair shaft in the deep dermis (haematoxylin and eosin (HE) staining, bar=250 µm). (D) Septate hyphae within and around the hair shaft and in the abscess in the square of Fig. 1C (periodic acid-Schiff [PAS] staining, bar=25 µm). (E) Many hyphae in the dilated hair follicles continuous from the epidermis (Grocott staining, bar=250 µm). (F) Cyst containing keratin materials in the dermis (HE staining, bar=500 µm). (G) Cyst containing septate hyphae (Grocott staining, bar=100 µm). (H) Multinucleated giant cells phagocytosed septate hyphae in the square of Fig. 1F. (PAS staining, bar=50 µm).
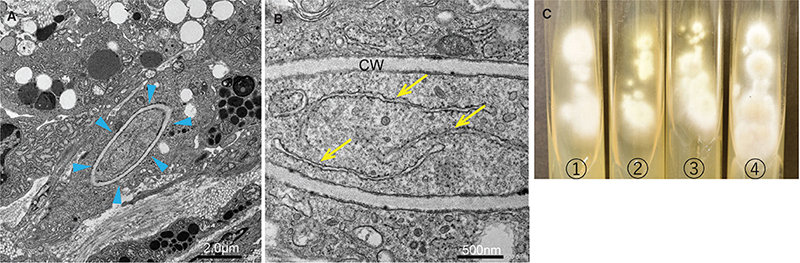
Fig. 2. (A–B) Transmission electron microscopy (JEM-1400 transmission electron microscope [JEOL, Tokyo, Japan]) around the cyst of the right upper eyelid. (A) A histiocyte contained fungal hyphae. Arrowheads: fungal hypha. Scale bar: 2.0 µm. (B) The fungal hypha has a cell wall of about 160 nm in thickness. The cell wall shows a regular lamination. Intracellular organelles and rough endoplasmic reticulum in the cytoplasm of a fungal hypha were observed clearly. Arrows: rough endoplasmic reticulum. CW: cell wall. Scale bar: 500 nm. (C) Colony surface on Sabouraud dextrose agar at 27°C after 2 weeks of incubation. ➀ nodule of the right upper eyelid (KMU 10705) ➁ nodule of the superior part of the left upper eyelid (KMU 10706) ➂ nodule of the lower part of the left upper eyelid (KMU 10707) ➃ interdigital scales (KMU 10708).
DISCUSSION
Majocchi’s granuloma was first described in 1883 by Professor Domenico Majocchi (1) and is characterized by perifollicular granulomatous inflammation (2, 3). It is classified as one of the clinical types of localized invasive dermatophytosis (2). Boral et al. reviewed 33 cases (21 men and 12 women) of Majocchi’s granuloma published in the English literature between 2011 and 2017 (4). The mean age of the patients was 38 years. Around 38% of the patients were immunosuppressed and 62% of the patients were immunocompetent. The most common predisposing factor (in 55% of patients) was the use of topical steroid cream. The most common causative dermatophytosis was T. rubrum (55.6%), followed by T. mentagrophytes (18.5%), T. interdigitale (7.4%), T. tonsurans (7.4%), and T. violaceum (3.7%). Regarding the pathogenicity of the fungi in granuloma trichophyticum, Nishiyama et al. experimentally investigated the conversion process of T. rubrum from hyphae to yeast-like cells by the shaking culture and agar-implantation method. The parasitic forms of the strain of T. rubrum isolated from tinea superficialis converted from hyphal to spherical in the peritoneal cavity of mice, and the isolates survived for 16 weeks. In contrast, the isolates from granuloma trichophyticum survived for more than 26 weeks and grow in hyphal forms (5). In another study, Miyazi and Nishimura reported that spherical cells of T. rubrum survived longer than hyphae in the peritoneal cavities of mice (6). In the present case, the parasitic form of T. rubrum in the granulomas was hyphal. We further investigated the ultrastructure of T. rubrum in lesions using TEM. Fungal hyphae in the histiocytes showed a regularly laminated cell wall, and there was no noticeable damage to the plasma membrane. The rER was clearly visible in the cytoplasm. This suggests that fungal hyphae are active in granulomas without keratinized tissue.
In the present case, fungal elements were observed inside and around the torn hair shafts of the abscess. A hair follicle is considered an intrusion passage of the fungal hyphae. Oral administration of terbinafine was effective in treating abscesses and granulomas of Majocchi’s granuloma. However, some lesions were resistant to oral terbinafine and were surgically resected. Although the terbinafine-resistant T. rubrum strain is associated with a missense mutation (L393F, F397L, etc.) in the squalene epoxidase (SQLE) gene (7), all 4 sequences (KMU 10705, 10706, 10707, and 10708) in our case were identical and matched the sequence of the T. rubrum SQLE wild-type strain reported in the literature (accession No. OM313296), indicating that these were strains exhibited normal susceptibility. Histopathology of these lesions confirmed the presence of cysts with keratinized epithelium and fungal elements in the keratin materials. Although deep dermatophytosis with the formation of a pseudocyst in subcutaneous tissue is well known as “cystic granuloma trichophyticum” (8–11), deep dermatophytosis with an epidermal cyst has not been reported. In all previous cases of cystic granuloma trichophyticum, the cyst walls were composed of histiocytes or fibrous capsules, and the cases were treated with resection in addition to the administration of an oral antifungal agent (8–11). Kaneko & Kaneko (8) reported a case of cystic granuloma trichophyticum with abscesses encapsulated by fibrous capsules. The patient was treated with surgical resection as in our case (8). They suggested that more invasive therapies, such as surgical resection, should be used for cystic granuloma trichophyticum with fibrous capsules. Our case suggests that surgical treatment should be considered when we encounter systemic antifungal treatment-resistant dermatophyte granuloma due to a possibility of the formation of a pseudocyst with fibrous capsules and a cyst lined with keratinized epidermal cells, as in our case.
In conclusion, we report a rare case of Majocchi’s granuloma caused by T. rubrum with multiple epidermal cysts containing fungal elements that required surgical resection in addition to the administration of an oral antifungal agent. TEM findings showed that the fungal cells in the granuloma had growing hyphae.
REFERENCES
- Majocchi D. A new trichophytic granuloma: clinical and mycological studies. Bull R Acad Med Roma 1883; 9: 220–223.
- Rouzaud C, Hay R, Chosidow O, Dupin N, Puel A, Lortholary O, et al. Severe dermatophytosis and acquired or innate immunodeficiency: a review. J Fungi (Basel) 2015; 2: 4. https://doi.org/10.3390/jof2010004
- Durdu M, Kandemir H, Ilkit M, de Hoog GS. Changing concepts and current definition of Majocchi’s granuloma. Mycopathologia 2020; 185: 187–192. https://doi.org/10.1007/s11046-019-00358-3
- Boral H, Durdu M, Ilkit M. Majocchi’s granuloma: current perspectives. Infect Drug Resist 2018; 11: 751–760. https://doi.org/10.2147/IDR.S145027
- Nishiyama C, Miyaji M, Saheki M, Morioka S. Studies on the parasitic forms of Trichophyton rubrum isolated from patients with granuloma trichophyticum using the “agar-implantation method”. J Dermatol 1985; 12: 325–328. https://doi.org/10.1111/j.1346-8138.1985.tb02849.x
- Miyazi M, Nishimura K. Studies of arthrospore of Trichophyton rubrum (I). Jpn J Med Mycol 1971; 12: 18–23. https://doi.org/10.3314/jjmm1960.12.18
- Bortoluzzi P, Prigitano A, Sechi A, Boneschi V, Germiniasi F, Esposto MC, et al. Report of terbinafine resistant Trichophyton spp. in Italy: clinical presentations, molecular identification, antifungal susceptibility testing and mutations in the squalene epoxidase gene. Mycoses 2023; 66: 680–687. https://doi.org/10.1111/myc.13597
- Kaneko T, Kaneko M. A patient with cystic granuloma trichophyticum who required surgical resection. Med Mycol J 2017; 58: E29–E32. https://doi.org/10.3314/mmj.16-00030
- Kobayashi M, Ishida E, Yasuda H, Yamamoto O, Tokura Y. Tinea profunda cysticum caused by Trichophyton rubrum. J Am Acad Dermatol 2006; 54: S11–S13. https://doi.org/10.1016/j.jaad.2005.03.058
- Matsuzaki Y, Ota K, Sato K, Nara S, Yagushi T, Nakano H, et al. Deep pseudocystic dermatophytosis caused by Trichophyton rubrum in a patient with myasthenia gravis. Acta Derm Venereol 2013; 93: 358–359. https://doi.org/10.2340/00015555-1452
- Toyoki M, Hase M, Hirasawa Y, Umeyama T, Miyazaki Y, Kano R, et al. A giant dermatophyte abscess caused by Trichophyton rubrum in an immunocompromised patient. Med Mycol J 2017; 58: E63–E66. https://doi.org/10.3314/mmj.17-00003