ORIGINAL REPORT
Telangiectasia Macularis Multiplex Acquisita and its Potential Association with Calcium Channel Blockers: A Retrospective Study of 46 Chinese Patients
Tian CHEN, Jia-Wei LIU, Yue-Tong QIAN, Xing-Yu LI, Xiao MA, Jing-Wen WANG and Dong-Lai MA
Department of Dermatology, Peking Union Medical College Hospital, State Key Laboratory of Complex Severe and Rare Diseases, Chinese Academy of Medical Science and Peking Union Medical College, National Clinical Research Center for Dermatologic and Immunologic Diseases, Beijing, China
Abstract
Telangiectasia macularis multiplex acquisita is an acquired cutaneous telangiectasis of unknown aetiology, and it lacks both effective and cost-efficient treatment. This study aims to identify a novel potential associated factor of the disease and explore feasible therapeutic interventions. In this retrospective case series study, 46 Chinese patients diagnosed with telangiectasia macularis multiplex acquisita between 1 January 2007 and 18 May 2023 were included. The median age of onset was 43 years (23 to 60 years), and the male to female ratio was 10.5:1. Besides previously reported associations including chronic liver disorders, alcohol consumption, and smoking, a potential association was found between use of calcium channel blockers and development of telangiectasia macularis multiplex acquisita. Twenty-two of 27 hypertensive patients took calcium channel blockers, with 17 followed up. Ten out of 17 displayed a range of improvements following the cessation of calcium channel blockers; 1 patient reported no lesion change post-discontinuation of calcium channel blockers; 1 patient continued their medication but showed partial improvement after 2 pulsed dye laser treatments; 1 patient observed lesion colour lightening without altering hypertensive medication or other specific treatments; and another 4 kept their previous hypertensive regimen due to blood pressure stability concerns, with no change in their lesions. The study proposes that cessation of calcium channel blockers can be a novel therapeutic approach for affected individuals.
SIGNIFICANCE
Telangiectasia macularis multiplex acquisita is an acquired cutaneous telangiectasis of unknown aetiology, which lacks both effective and cost-efficient treatment. In our study, 46 Chinese patients diagnosed with telangiectasia macularis multiplex acquisita were included. We found that 22 of 27 patients with hypertension took calcium channel blockers, and 10 out of 17 patients taking calcium channel blockers at follow-up displayed improvements following the cessation of the medication. The study proposes that intake of calcium channel blockers is a potential trigger of telangiectasia macularis multiplex acquisita. The discontinuation of calcium channel blockers can be a novel therapeutic option for this disease.
Key words: telangiectasia macularis multiplex acquisita; telangiectasis; calcium channel blockers.
Citation: Acta Derm Venereol 2024; 104: adv40447. DOI: https://doi.org/10.2340/actadv.v104.40447.
Copyright: 2024 © The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Mar 29, 2024. Accepted after revision: Sep 17, 2024. Published: Oct 10, 2024
Corr: Dong-Lai Ma, MD, PhD, Department of Dermatology, Peking Union Medical College Hospital, State Key Laboratory of Complex Severe and Rare Diseases, Chinese Academy of Medical Science and Peking Union Medical College, National Clinical Research Center for Dermatologic and Immunologic Diseases, Beijing, China. E-mail: mdonglai@sohu.com & mdonglai@yeah.net
Competing interests and funding: The authors have no conflicts of interest to declare.
The research is supported by National High Level Hospital Clinical Research Funding 2022-PUMCH-A-161.
INTRODUCTION
Telangiectasia macularis multiplex acquisita (TMMA) is infrequently documented acquired cutaneous telangiectasis characterized by multiple symmetrical, asymptomatic, or mildly pruritic telangiectatic vessels overlaying erythematous or brown macules, with a predilection for the extensor sides of bilateral upper arms. These macules may exhibit a focal annular configuration (1). Mild surface atrophy or scaling is occasionally seen (1). Another 2 newly described acquired bilateral telangiectasia types in the literature are acquired bilateral telangiectatic macules and acquired bilateral naevoid telangiectasia, which share similar manifestations to TMMA. However, TMMA may be underreported due to its potential misdiagnosis as other telangiectatic diseases. Its aetiology is unknown, but it has been proposed that congenital defects on vessel walls or the ageing process may contribute to the pathogenesis of TMMA (1). TMMA predominantly affects middle-aged to elderly adults, and its prognosis is generally favourable with enduring existence. Although the telangiectasia blanches upon diascopy, the presence of the brown macule persists. Dermoscopy of the telangiectatic macules has revealed tortuous/arborizing vessels and diffuse brownish pigmentation (2). Histopathological findings of TMMA are nonspecific, mainly manifesting as hyperpigmentation in the basal layer of the epidermis and superficial dermal capillary dilation and/or proliferation with or without mild perivascular lymphocytic infiltration. Absence of dermal telangiectasia might be due to vasoconstriction induced by epinephrine in local anaesthetics (1). The amount of mast cell infiltration is within normal range. Several disease associations have been observed, including liver diseases (such as hepatitis, liver cirrhosis, hepatocellular carcinoma, and cholangiocarcinoma), hypertension, diabetes, smoking, alcohol consumption (1, 3–5).
This study analyses the clinicopathological and dermoscopic manifestations, disease association, and prognosis of TMMA in the Chinese population at our institution, and aims to summarize new possible risk factors and provide new therapeutic options.
MATERIALS AND METHODS
Study population
This retrospective hospital-based study was approved by the ethics committee of the Peking Union Medical College Hospital in accordance with the Declaration of Helsinki. Patients had been prospectively recruited at the outpatient clinic of the Dermatological Department at the Peking Union Medical College Hospital. First, patients diagnosed with “cutaneous telangiectasia” were identified through an electronic search of the hospital information system at Peking Union Medical College Hospital, based on the ICD-9 diagnosis code. Ultimately, a total of 46 patients who met the diagnostic criteria of TMMA identified at our Department of Dermatology from 1 January 2007 to 18 May 2023 were included.
Clinical data
We extracted clinical data including sex, age at visit, disease duration, lesion location and distribution, symptoms, trigger factors, underlying diseases, therapy, and therapeutic response. During the first telephone follow-up, we systematically documented their prior treatment methods employed for TMMA. Treatment recommendations, particularly lifestyle modifications, were provided. Every 3 months subsequent to the initial follow-up, these patients were contacted to monitor the treatment effect.
The diagnosis of TMMA was confirmed mainly through clinical photographs and medical records, and reconfirmed by 2 experienced dermatologists. The clinical criteria for diagnosis of TMMA included: (a) erythematous to brown macules with telangiectasia symmetrically on bilateral upper arms, possibly extending to the forearms, shoulders, V-shaped area of the anterior chest, back, abdomen, or neck; (b) no mucosal or systemic involvement; (c) not associated with autoimmune diseases, such as lupus erythematosus, dermatomyositis, or systemic scleroderma that may induce cutaneous telangiectasia; and (d) no ataxia or unsteady gait. Patients were excluded if they (a) revealed large segmental involvement, usually appearing first on the lower legs and then spreading to the upper legs, abdomen, and arms; (b) presented unilateral large punctate and stellate telangiectases; (c) had lesions on the dorsal aspects of forearms in postmenopausal women; (d) showed increased infiltrates of mast cells around dilated capillaries and venules in histopathology.
Dermoscopy and pathological assessment
Digital dermoscopy was performed using a high-resolution digital dermoscope. Skin biopsy specimens were re-examined by 2 dermatopathologists, and histopathological features were recorded. Haematoxylin-eosin staining was utilized to examine the general histopathologic changes in the skin lesions, and immunohistochemical staining of CD 117, and histochemical staining of Giemsa and toluidine blue was used to mark mast cells in pathological assessment.
Statistical analysis
The clinical data and demographic variables for the TMMA were evaluated using descriptive statistics and frequency tabulation. Categorical data were described by the number of patients with percentages.
Ethical statement
The present study was conducted in accordance with the Declaration of Helsinki (initially published in 1964) on Ethical Principles for Medical Research Involving Human Subjects. This study was approved by the ethics committee of the Peking Union Medical College Hospital (ethics number I-23PJ1959).
RESULTS
Demographic and clinical features of enrolled patients
The demographic and clinical data of the patients are systematically documented in Table I. The study included 46 patients, comprising 42 males and 4 females with a male to female ratio of 10.5:1. The median age of onset was 43 years, spanning from 23 to 60 years. The median duration of lesions at first visit to our clinic was 5 years, with a range from 1 month up to 30 years. All patients had Fitzpatrick skin types III and IV. None of the patients reported a family history of similar skin lesions.
| Pat. No. | Sex/age at visit, years | Disease duration, years | Affected site | Symptom | Darier’s sign | Aggravation factors | Therapy/durationa | Liver diseases | Smoking/alcohol | Diabetes | Skin biopsy/dermoscopy | Treatment/ prognosis |
| 1 | M/61 | 30 | Both upper arms and forearms, V-shaped area on the chest, and back | N | N | Sunlight | Y/levamlodipine besylate/14/N | N | N/N | Y | Y/N | N./Loss to follow-up |
| 2 | M/48 | 0.167 | Both upper arms and forearms, V-shaped area on the chest, and back | N | N | N | Y/levamlodipine besylate/5/4.833 | Fatty liver | Y/Y | N | Y/N | Discontinuation of levamlodipine besylate/slight lesional regres-sion and colour lightening |
| 3 | M/65 | 5 | Both upper arms, V-shaped area on the chest, and back | N | N | N | N | N | N/N | N | Y/N | N/loss to follow-up |
| 4 | F/56 | 0.5 | Both upper arms and forearms | N | N | N | N | N | N/N | N | Y/Y | N/unchanged |
| 5 | M/49 | 5 | Both upper arms and forearms, V-shaped area on the chest, and back | N | N | Heat | Y/nifedipine/7/2 | N | Y/Y | N | Y/N | Discontinuation of nifedipine/slight lesional regression and colour lighte-ning |
| 6 | M/53 | 2 | Both upper arms and forearms, V-shaped area on the chest, and back | N | N | N | N | HCV infection | N/N | N | Y/N | N/loss to follow-up |
| 7 | M/62 | 5 | Both upper arms, V-shaped area on the chest, and back | N | N | N | Y/nifedipine/Unknown/Unknown | N | Y/Y | N | Y/N | N/loss to follow-up |
| 8 | M/53 | 4 | Both upper arms and V-shaped area on the chest | N | N | Heat and sunlight | N | N | N/N | N | Y/N | N/loss to follow-up |
| 9 | M/57 | 7 | Both upper arms and forearms, V-shaped area on the chest, and back | N | N | Heat and sunlight | Y/telmisartan/unknown/unknown | N | Y/N | N | Y/N | N/area reduction |
| 10 | M/40 | 5 | Both upper arms and forearms | N | N | Heat, sunlight | N | N | Y/Y | N | N/Y. | N/unchanged |
| 11 | M/43 | 1 | Both upper arms and back | N | N | N | Y/amlodipine besylate/3/2 | N | Y/Y | N | Y/N | N/slight colour lightening |
| 12 | M/37 | 3 | Both upper arms, V-shaped area on the chest, and back | N | N | Sunlight, and alcohol consumption | N | N | Y/Y | N | N/N | N/colour lightening |
| 13 | M/44 | 10 | Both upper arms and forearms, V-shaped area on the chest, and back | N | N | Heat, sunlight, and alcohol consumption | Y/nifedipine/4/N | N | Y/N | N | Y/N | N/unchanged |
| 14 | M/48 | 1 | Both upper arms and forearms, V-shaped area on the chest, and back | N | N | N | N | N | N/N | N | Y/N | N/loss to follow-up |
| 15 | M/44 | 6 | Both upper arms, V-shaped area on the chest, and back | N | N | Heat, sunlight, and alcohol consumption | N | Fatty liver | Y/N | N | Y/N | N/unchanged |
| 16 | M/50 | 4 | Both upper arms and forearms, V-shaped area on the chest, and back | N | N | Heat, sunlight, and alcohol consumption | Y/nifedipine/10/6 | N | Y/Y | N | Y/N | Discontinuation of nifedipine/no aggregation after heat and alcohol con-sumption |
| 17 | M/51 | 0.083 | Both upper arms and forearms, V-shaped area on the chest, and back | N | N | N | N | HBV infection and liver carcinoma | N/N | N | Y/N | N/loss to follow-up |
| 18 | M/51 | 7 | Both upper arms, V-shaped area on the chest, and back | N | N | N | N | N | N/N | N | Y/N | N/loss to follow-up |
| 19 | M/57 | 1 | Both upper arms and forearms, V-shaped area on the chest, and back | Pruritus | N | Heat, sunlight, and alcohol consumption | Y/amlodipine besylate/unknown/unknown | N | Y/Y | Y | Y/N | N/loss to follow-up |
| 20 | M/47 | 10 | Both upper arms and forearms, V-shaped area on the chest, back, abdomen, and neck | N | N | Heat, sunlight, and alcohol consumption | Y/nifedipine/15/5 | N | Y/Y | N | Y/N | Discontinuation of nifedipine/significant lesional regression |
| 21 | F/39 | 1 | Both upper arms | N | N | Heat and sunlight | N | N | N/N | N | N/Y | N/colour lightening |
| 22 | M/39 | 10 | Both upper arms | N | N | Heat, sunlight, and alcohol consumption | N | N | Y/N | N | Y/N | N/unchanged |
| 23 | M/43 | 20 | Both upper arms, V-shaped area on the chest, and back | N | N | Sunlight, and alcohol consumption | Y/one type of CCB (unrecalled)/4/N | Fatty liver | Y/Y | N | Y/N | Discontinuation of CCB/unchanged |
| 24 | M/50 | 7 | Both upper arms, V-shaped area on the chest, and back | N | N | Heat and sunlight | Y/telmisartan hydrochloro-thiazide/5/2 | N | Y/Y | N | Y/N | N/area increase on forearms and hands, and number increase on original affect-ed sites |
| 25 | M/43 | 5 | Both upper arms | N | N | N | N | N | N/N | N | Y/N | N/loss to follow-up |
| 26 | M/33 | 2 | Both upper arms and forearms, V-shaped area on the chest, and back | N | N | Heat | N | N | Y/Y | N | Y/N | N/Unchanged |
| 27 | F/48 | 10 | Both upper arms and forearms, V-shaped area on the chest, and back | N | N | N | Y/unknown/unknown/unknown | HBV infection | Y/Y | N | Y/N | Cessation of smoking/complete regression |
| 28 | M/43 | 8 | Both upper arms and forearms, V-shaped area on the chest, and back | N | N | Heat, sunlight, and alcohol consumption | N | N | Y/Y | N | N/N | N/unchanged |
| 29 | M/56 | 20 | Both upper arms, and V-shaped area on the chest | Pruritus | N | Heat, sunlight, and alcohol consumption | Y/nifedipine/22/2 | N | Y/Y | N | Y/N | Discontinuation of nifedipine/significant colour lightening |
| 30 | M/61 | 3 | Both upper arms and forearms, V-shaped area on the chest, and back | N | N | Heat and sunlight | Y/amlodipine besylate/6/3 | N | Y/N | N | N/N | Discontinuation of amlodipine besylate/slight regression and colour lighte-ning |
| 31 | M/44 | 0.75 | Both upper arms, V-shaped area on the chest, and back | N | N | Heat and alcohol consumption | Y/nifedipine/8/7.25 | N | Y/Y | N | Y/N | Discontinuation of nifedipine/significant lesio-nal regres-sion and colour lightening |
| 32 | M/49 | 8 | Both upper arms and forearms | N | N | Alcohol consumption | Y/levamlodipine besylate/16/8 | N | N/N | N | N/Y | Discontinuation of levamlodipine besylate/slight lesional regre-sion, colour lightening, and no aggregation after alcohol consumption |
| 33 | M/56 | 2 | Both upper arms, V-shaped area on the chest, and back | N | N | Heat and sunlight | Y/levamlodipine besylate/6/4 | N | Y/Y | N | Y/N | Discontinuation of levamlodipine besylate/slight lesional regres-sion and colour lightening |
| 34 | M/58 | 2 | Both upper arms and forearms, V-shaped area on the chest, and back | N | N | Heat, sunlight, and alcohol consumption | Y/amlodipine besylate/17/15 | HBV infection and fatty liver | Y/Y | Y | Y/Y | Discontinuation of amlodipine besylate/signi-ficant lesional regression and colour lighte-ning |
| 35 | M/48 | 10 | Both upper arms and forearms, V-shaped area on the chest, and back | N | N | N | Y/unknown/unknown/unknown | HBV infection | N/N | Y | Y/N | N/loss to follow-up |
| 36 | M/52 | 1 | Both upper arms | N | N | Heat and sunlight | N | N | Y/Y | N | Y/N | N/unchanged |
| 37 | M/44 | 10 | Both upper arms and forearms, V-shaped area on the chest, and back | N | N | N | Y/levamlodipine besylate/3/N | N | Y/N | N | Y/N | N/loss to follow-up |
| 38 | M/59 | 1 | Both upper arms | N | N | N | Y/unknown/5/4 | N | Y/N | N | Y/N | N/unchanged |
| 39 | M/55 | 10 | Both upper arms and forearms, V-shaped area on the chest, and back | N | N | Heat, sunlight, and alcohol consumption | Y/nifedipine/20/10 | N | N/Y | N | Y/N | N/unchanged |
| 40 | M/53 | 2 | Both upper arms and forearms, and V-shaped area on the chest | Pruritus | N | Heat | Y/felodipine/15/13 | N | Y/Y | N | Y/N | Pulsed dye laser treatment/slight lesional regres-sion |
| 41 | M/52 | 10 | Both upper arms and forearms, V-shaped area on the chest, back, abdomen, and back of neck | N | N | Heat and sunlight | Y/amlodipine besylate/23/13 | N | Y/N | N | Y/N | N/unchanged |
| 42 | M/55 | 2 | Both upper arms, V-shaped area on the chest, and back | N | N | Heat and sunlight | Y/nifedipine/16/14 | HBV infection and HCV infection | Y/Y | N | Y/N | N/unchanged |
| 43 | M/45 | 3 | Both upper arms and forearms, V-shaped area on the chest, and back | N | N | Heat and sunlight | Y/nifedipine/22/19 | N | Y/Y | N | Y/N | N/loss to follow-up |
| 44 | M/50 | 10 | Both upper arms and forearms | N | N | Sunlight, and alcohol consumption | N | N | Y/Y | N | Y/N | N/unchanged |
| 45 | F/42 | 10 | Both upper arms | N | N | N | N | N | N/N | N | Y/N | N/unchanged |
| 46 | M/52 | 10 | Both upper arms, V-shaped area on the chest, and back | N | N | Heat | N | N | N/N | N | Y/N | N/unchanged |
| aHypertension/antihypertensive therapy/duration of antihypertensive therapy at first presentation, years/duration of Antihypertensive therapy before lesions appear, years. M: male; F: female; N: none; Y: yes; HBV: hepatitis B virus; HCV: hepatitis C virus. | ||||||||||||
Clinically, all 46 patients exhibited round to oval or irregular, dark-red to brown telangiectatic macules that developed insidiously (Fig. 1). The majority of the patients (43/46, 93.48%) experienced asymptomatic lesions, while mild pruritus was reported by another 3 patients (3/46, 6.52%). All cases tested negative for Darier’s sign.

Fig. 1. Clinical images of study patients. Round to oval or irregular, dark red to brown telangiectatic macules on upper arms (A1–4), forearms (B1–4), the V-shaped area of the anterior chest (C1–4), back (D1–5), abdomen (C3–4), and neck (E1–2).
The distribution of the affected skin areas was extensive, encompassing both upper arms (46/46, 100%), both forearms (26/46, 56.52%), the V-shaped area of the anterior chest (35/46, 76.09%), and back (33/46, 71.74%) (Table I). The abdomen and neck were also affected in 2 patients (2/46, 4.35%).
Factors that aggravated the condition were heat (26/46, 56.52%), sunlight (25/46, 54.35%), and alcohol consumption (15/46, 32.61%). Notably, the influence of the above factors on the skin lesions was temporary. After stopping or eliminating these factors, their lesions soon returned to the original appearance.
Dermoscopic and histopathologic findings
Dermoscopic examinations conducted on 5 patients (5/46, 10.87%) revealed tortuous/arborizing vessels and diffuse brownish pigmentation on the upper arms (Fig. 2). Another 41 patients had not had dermoscopy performed examination due to the limitation of medical conditions at that time. Histopathologic analysis performed on 40 patients (40/46, 86.96%) demonstrated slight hyperpigmentation in the basal layer of the epidermis and superficial dermal capillary dilation and/or proliferation with or without mild perivascular lymphocytic infiltration on haematoxylin-eosin staining (Fig. 3). Immunohistochemical staining of CD117 was performed in 9 patients (9/46, 19.57%). Histochemical staining was performed with Giemsa in 3 out of 46 patients (6.52%) and with toluidine blue in 2 out of 46 patients (4.35%). It was observed that, using CD117, Giemsa, or toluidine blue staining, lesional skin samples contained fewer than 5 perivascular mast cells at each high-power view. Another 6 patients declined further skin biopsy, and diagnosis was made according to their typical clinical manifestations.
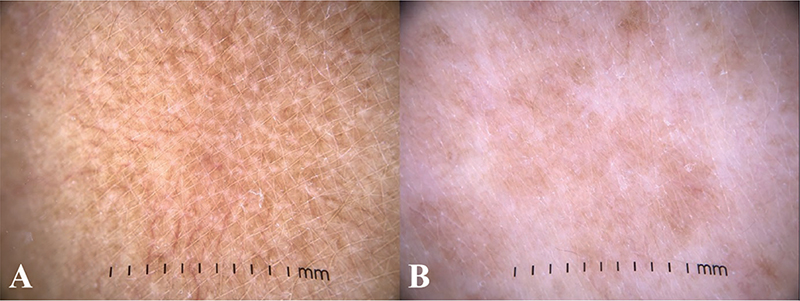
Fig. 2. Dermoscopic findings of study patients. (A) Tortuous/arborizing vessels and (B) diffuse brownish pigmentation on dermoscopy.
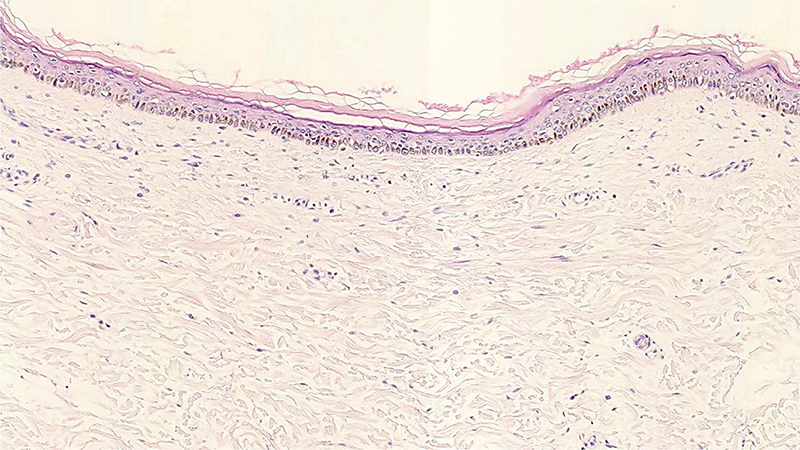
Fig. 3. Histochemical and immunohistochemical features in lesional samples. Slight hyperpigmentation in the epidermal basal layer and superficial dermal capillary proliferation, with mild perivascular lymphocytic infiltration (H&E staining, original magnification×100).
Associated factors of telangiectasia macularis multiplex acquisita
In this study, 19.57% of the patients (9 out of 46) had chronic liver disorders, encompassing hepatitis B virus infection, hepatitis C virus infection, fatty liver, or liver carcinoma. The prevalence of long-term alcohol consumption and smoking among the patients was observed to be 52.17% (24 out of 46) and 67.39% (31 out of 46) respectively. Additionally, 58.70% (27 out of 46) of the patients had a history of hypertension, with 47.83% (22 out of 46) being treated with calcium channel blockers (CCBs), including amlodipine besylate, levamlodipine besylate, nifedipine, or felodipine. Among these 22 patients, 17 had received CCBs earlier than the onset of lesions. The median duration of CCB treatment before lesions appeared was 6 years, spanning from 2 to 19 years. Notably, patient No. 11 reported the emergence of telangiectatic lesions post-initiation of amlodipine besylate therapy, and patient No. 13 observed a significant increase in lesions while on nifedipine. Some 8.70% (4 out of 46) of the patients had diabetes. These details were systematically tabulated in Tables I and II.
Regarding follow-up data, 71.74% of the patients (33 out of 46) were observed, while 28.26% (13 out of 46) were lost to follow-up. The median duration of the follow-up period was 2.38 years, ranging from 7 months to 10.67 years. Of the 22 patients prescribed CCBs, 17 were followed up, and 5 were lost to follow-up. Within the followed-up group on CCBs, 58.83% (10 out of 17) exhibited various degrees of lesion regression, colour lightening, and/or diminished lesion aggregation after exposure to heat or alcohol consumption subsequent to the discontinuation of previously administered CCBs; 5.88% (1 out of 17) reported no alteration in lesions post-CCB discontinuation; 5.88% (1 out of 17) retained CCB therapy but showed partial improvement following 2o sessions of pulsed dye laser treatment; 5.88% (1 out of 17) reported colour lightening of lesions without medication alteration or specific treatment; and 23.53% (4 out of 17) maintained their CCB regimens due to concerns over blood pressure stability, with no change in lesions. Among the other 16 patients who were not hypertensive or not on CCBs at follow-up, 6.25% (1 out of 16) noted complete regression of lesions after quitting smoking; without specific treatments, 6.25% (1 out of 16) experienced a partial increase in lesions and 18.75% (3 out of 16) observed colour lightening or lesion area reduction; the remaining 68.75% (11 out of 16) reported no significant changes in their lesions. These details were summarized in Table I.
DISCUSSION
In our study, the individual lesions observed in patients with TMMA remained consistent, manifesting as telangiectatic vessels overlaying erythematous or brown macules. However, the characteristics of the rashes varied among different patients in terms of size, number, and intensity of redness prior to treatment. The number of rashes among different patients ranged from several to hundreds, with colours varying from pale red to vivid crimson. In our case series, the lateral side of both upper limbs was the most commonly affected site, followed by the V-shaped area of the anterior chest, back, and both forearms. The involvement of abdomen and neck was uncommon but was observed in some patients with widespread lesions. Notably, the morphology of widespread lesions is a tendency to coalesce into patches with an annular arrangement. The lesions predominantly affected middle-aged men. Aggravating factors such as heat, sunlight exposure, and alcohol consumption may act synergistically in contributing to the onset and progression of this condition. However, the effects of these factors on the skin lesions appear to be temporary; upon cessation or elimination of these influences, the lesions generally revert to their original appearance.
Consistent with prior findings, a high prevalence of smoking and alcohol consumption was noted among TMMA patients in this case series. Specifically, 67.39% of the patients were regular smokers. Nicotine has been associated with reduced cutaneous capillary and arteriolar blood flow, leading to chronic dermal ischaemia through increased levels of vasopressin, a vasoconstrictor (6–8). This chronic ischaemia is believed to stimulate the proliferation of small blood vessels and cause epidermal atrophy, thus making telangiectasia more apparent (9). One patient demonstrated complete lesion regression after ceasing smoking, lending support to the hypothesized role of nicotine in TMMA pathogenesis. Additionally, 52.17% of the patients reported long-term alcohol consumption, with many experiencing lesion aggravation post-alcohol intake. Ethanol’s role in vascular relaxation is mediated by redox-sensitive and NO–cGMP-dependent pathways, involving direct effects on reactive oxygen species production and nitric oxide signalling (10). Compared with previous reports (1, 2), the proportion of TMMA patients with liver diseases in our series was significantly lower. The potential mechanisms linking telangiectasia to liver diseases are proposed to involve a generalized hyperdynamic circulation, increased levels of plasma vascular endothelial growth factor and basic fibroblast growth factor, and elevated substance P (11, 12). Additionally, heat and sunlight may exacerbate the lesions, potentially due to their role in promoting telangiectasia.
Hypertension may result in increased peripheral circulation pressure, leading to compensatory vasodilation, which subsequently contributes to the development of telangiectasia and TMMA rash. However, we have observed that patients prescribed antihypertensive therapy typically initiated treatment after being diagnosed as having hypertension. During the therapy, their blood pressure control was generally stable, typically maintained within the range of 120–140/70–90 mmHg. Therefore, we conclude that the observed changes in the condition are likely not directly related to blood pressure levels. Noticeably, we discovered that the predominant antihypertensive medication regimen in patients with TMMA and hypertension mainly primarily involved CCBs, such as amlodipine besylate, levamlodipine besylate, nifedipine, and felodipine. In our study, 2 patients noted either the onset or exacerbation of TMMA following the initiation of CCB therapy. Furthermore, within the followed-up patients on CCBs, 11 out of 17 patients discontinued previously administered CCBs. Remarkably, 90.91% (10 out of 11) of these patients displayed various degrees of improvement in lesions after their medication alteration, while the remaining 9.09% (1 out of 11) ceased CCB usage in a relatively short time, resulting in insignificant changes in his rash. Consequently, we hypothesize a potential link between the onset of TMMA and the utilization of CCBs. Existing literature has reported instances of photodistributed telangiectasia induced by CCBs, including nifedipine (13, 14), amlodipine (15, 16), felodipine (17), and diltiazem (18). Photodistributed telangiectasia resulting from CCBs typically manifests as asymptomatic widely distributed spider-like telangiectasia on the face, V area of the chest, extensor aspects of the arms, and the upper back after 1 month to 1 year of use. Skin eruptions have been observed to improve rapidly following the discontinuation of CCB treatment (19). Histopathology reveals enlarged capillaries in the upper dermis, devoid of any signs of vasculitis. The clinical manifestations and histopathology of TMMA and photodistributed telangiectasia from CCBs is strikingly similar, leading us to propose the classification of photodistributed telangiectasia induced by CCBs as a subtype of TMMA. Notably, most of the reported cases regarding CCB-induced photodistributed telangiectasia are from dihydropyridines. The hypothetical mechanisms of the phenomenon include their greater vascular smooth muscle effects relative to cardiac effects than other types of CCBs (20), and the ability to generate ROS such as pyridine, nitrosopyridine, and nitropyridine on ultraviolet exposure (21). The process is reversible under normal skin conditions following the discontinuation of CCBs.
The differential diagnoses of TMMA include spider angiomas, generalized essential telangiectasia, and telangiectasia macularis eruptiva perstans (TMEP) (Table III). Despite the similarity in the anatomical distribution of spider angiomas and TMMA, they exhibit distinct morphological characteristics. Spider angiomas are characterized by a central elevated dark erythematous papule (spider body), encircled by multiple, tiny, radial telangiectatic vessels (spider legs) (1, 22). Histopathological examination of spider angiomas shows a central arteriole ascending towards a thin-walled ampulla beneath the epidermis, with small arterial branches extending into the papillary dermis (23). Unlike TMMA, generalized essential telangiectasia typically shows a female preponderance and initially manifests as matted telangiectasia sheets on the lower legs, potentially extending to the trunk, upper limbs, and face, without any known association with liver diseases or other systemic illnesses. Distinguishing TMMA from TMEP poses a diagnostic challenge. Clinically, TMEP also presents with telangiectatic tan to brown macules on the trunk and extremities (24, 25). Histopathological examinations of TMEP reveal increased infiltrations of mast cells, primarily in the upper dermis and often clustered around dilated capillaries and venules (25). Immunohistochemical staining for CD117 and histochemical staining for Giemsa or toluidine blue show positive results for mast cells in TMEP cases.
The limitations of this study include that this was a retrospective investigation in a single medical centre. The information on latent disease was incomplete; further analysis of long-term data is required. Moreover, given the considerable time and financial burdens associated with outpatient visits for many patients, we opted for telephone follow-ups. The reliability of lesional improvement data mainly reliant on the patient’s subjective evaluation was constrained compared with the detailed clinical images furnished during follow-ups.
Telangiectasia macularis multiplex acquisita typically demonstrates persistence with minimal regression propensity, rendering its management particularly challenging. Therapeutic interventions, including pulsed dye laser and intense pulsed light that specifically target vascular and pigmentary elements, may be pursued for cosmetic improvement (26, 27), but these are costly for widely affected lesions. Our study suggests that eliminating related triggers of TMMA could provide an alternative therapeutic strategy. Notably, in our cohort, discontinuation of CCBs in hypertensive individuals and cessation of smoking were identified as both effective and cost-efficient measures for some patients.
ACKNOWLEDGEMENTS
The authors would like to thank Kai Fang, Qian-Nan Jia, and Meng-Xue Gao (Peking Union Medical College Hospital, Beijing, China), who were involved in processing samples for histopathology.
REFERENCES
- Chang CH, Lu PH, Kuo CJ, Yang CH. Telangiectasia macularis multiplex acquisita: a new entity in Chinese populations and an analysis of associated factors. Int J Dermatol 2013; 52: 426–431. https://doi.org/10.1111/j.1365-4632.2011.05331.x
- Zhang ZW, Wu H, Tang KF, Fan YM. Clinicodermoscopic and immunohistochemical observation of hepatitis B virus-associated acquired bilateral telangiectatic macules in a Chinese man. An Bras Dermatol 2021; 96: 791–793. https://doi.org/10.1016/j.abd.2020.08.027
- Wang G, Chen H, Yang Y, Wu K, Sun J. Telangiectasia macularis multiplex acquisita accompanied by hepatitis B infection. Australas J Dermatol 2017; 58: e5–7. https://doi.org/10.1111/ajd.12398
- Kim GW, Shin K, Kim TW, You HS, Jin HJ, Shim WH, et al. The importance of dermoscopy for the diagnosis of acquired bilateral telangiectatic macules: the angioid streak pattern reveals underlying chronic liver disease. J Eur Acad Dermatol Venereol 2018; 32: 1597–1601. https://doi.org/10.1111/jdv.14669
- Jee H, Kim TG, Kim DS, Kim DY, Lee MG. Acquired bilateral nevoid telangiectasia: report of 9 cases. Eur J Dermatol 2013; 23: 736–737. https://doi.org/10.1684/ejd.2013.2141
- Reus WF, Robson MC, Zachary L, Heggers JP. Acute effects of tobacco smoking on blood flow in the cutaneous micro-circulation. Br J Plast Surg 1984; 37: 213–215. https://doi.org/10.1016/0007-1226(84)90011-0
- Richardson D. Effects of tobacco smoke inhalation on capillary blood flow in human skin. Arch Environ Health 1987; 42: 19–25. https://doi.org/10.1080/00039896.1987.9935790
- Francès C, Boisnic S, Hartmann DJ, Dautzenberg B, Branchet MC, Charpentier YL, et al. Changes in the elastic tissue of the non-sun-exposed skin of cigarette smokers. Br J Dermatol 1991; 125: 43–47. https://doi.org/10.1111/j.1365-2133.1991.tb06037.x
- Kennedy C, Bastiaens MT, Bajdik CD, Willemze R, Westendorp RG, Bouwes Bavinck JN, et al. Leiden Skin Cancer Study: effect of smoking and sun on the aging skin. J Invest Dermatol 2003; 120: 548–584. https://doi.org/10.1046/j.1523-1747.2003.12092.x
- Rocha JT, Hipólito UV, Callera GE, Yogi A, Neto Filho Mdos A, Bendhack LM, et al. Ethanol induces vascular relaxation via redox-sensitive and nitric oxide-dependent pathways. Vascul Pharmacol 2012; 56: 74–83. https://doi.org/10.1016/j.vph.2011.11.006
- Ghosn SH, Kibbi AG. Cutaneous manifestations of liver diseases. Clin Dermatol 2008; 26: 274–282. https://doi.org/10.1016/j.clindermatol.2008.02.001
- Li CP, Lee FY, Hwang SJ, Chang FY, Lin HC, Lu RH, et al. Role of substance P in the pathogenesis of spider angiomas in patients with nonalcoholic liver cirrhosis. Am J Gastroenterol 1999; 94: 502–507. https://doi.org/10.1111/j.1572-0241.1999.883_l.x
- Collins P, Ferguson J. Photodistributed nifedipine-induced facial telangiectasia. Br J Dermatol 1993; 129: 630–633. https://doi.org/10.1111/j.1365-2133.1993.tb00501.x
- Tsele E, Chu AC. Nifedipine and telangiectasias. Lancet 1992; 339: 365–366. https://doi.org/10.1016/0140-6736(92)91685-2
- Basarab T, Yu R, Jones RR. Calcium antagonist-induced photo-exposed telangiectasia. Br J Dermatol 1997; 136: 974–975. https://doi.org/10.1111/j.1365-2133.1997.tb03952.x
- Grabczynska SA, Cowley N. Amlodipine induced-photosensitivity presenting as telangiectasia. Br J Dermatol 2000; 142: 1248–1256. https://doi.org/10.1046/j.1365-2133.2000.03572.x
- Karonen T, Stubb S, Keski-Oja J. Truncal telangiectases coinciding with felodipine. Dermatology 1998; 196: 272–273.
- Seggev JS, Lagstein Z. Photosensitivity skin reactions to calcium channel blockers. J Allergy Clin Immunol 1996; 97: 852–855. https://doi.org/10.1016/S0091-6749(96)80164-3
- Bakkour W, Haylett AK, Gibbs NK, Chalmers RJ, Rhodes LE. Photodistributed telangiectasia induced by calcium channel blockers: case report and review of the literature. Photodermatol Photoimmunol Photomed 2013; 29: 272–275. https://doi.org/10.1111/phpp.12054
- Byun JW, Bang CI, Yang BH, Han SH, Song HJ, Lee HS, et al. Photodistributed telangiectasia induced by amlodipine. Ann Dermatol 2011; 23: S30–32. https://doi.org/10.5021/ad.2011.23.S1.S30
- Onoue S, Igarashi N, Yamada S, Tsuda Y. High-throughput reactive oxygen species (ROS) assay: an enabling technology for screening the phototoxic potential of pharmaceutical substances. J Pharm Biomed Anal 2008; 46: 187–193. https://doi.org/10.1016/j.jpba.2007.09.003
- Khasnis A, Gokula RM. Spider nevus. J Postgrad Med 2002; 48: 307–309.
- Requena L, Sangueza OP. Cutaneous vascular anomalies. Part I. Hamartomas, malformations, and dilation of preexisting vessels. J Am Acad Dermatol 1997; 37: 523–549; quiz 549–552. https://doi.org/10.1016/S0190-9622(97)70169-5
- Katsamba AD, Karpouzis AJ, Koumantaki-Mathioudaki E, et al. Mastocytosis with skin manifestations: current status. J Eur Acad Dermatol Venereol 1999; 13: 148–165. https://doi.org/10.1111/j.1468-3083.1999.tb00878.x
- Vano-Galvan S, Alvarez-Twose I, De las Heras E, Morgado JM, Matito A, Sánchez-Muñoz L, Jorizzo JL. Dermoscopic features of skin lesions in patients with mastocytosis. Arch Dermatol 2011; 147: 932–940. https://doi.org/10.1001/archdermatol.2011.190
- Yang JY, Kim SM, Kim YC. Pulsed dye laser therapy in patients with acquired bilateral telangiectatic macules. Eur J Dermatol 2018; 28: 99–100. https://doi.org/10.1684/ejd.2017.3159
- Park JH, Lee DJ, Lee YJ, Jang YH, Kang HY, Kim YC. Acquired bilateral telangiectatic macules: a distinct clinical entity. JAMA Dermatol 2014; 150: 974–977. https://doi.org/10.1001/jamadermatol.2013.10238