ORIGINAL REPORT
A European Consensus on the Consistent Use of the Term “Keratinocyte Cancer”
Wolfgang G. PHILIPP-DORMSTON1,2, Lasse R. BRAATHEN3, Colin A. MORTON4, Merete HAEDERSDAL5, Yolanda GILABERTE6, Nicole BASSET-SEGUIN7,8, Elena SOTIRIOU9, Stine Regin WIEGELL10, Piergiacomo CALZAVARA-PINTON11,12, Thomas DIRSCHKA13, Hans Christian WULF10, Günther HOFBAUER14,15 and Rolf Markus SZEIMIES16
1Hautzentrum Köln (Cologne Dermatology), Köln, Germany, 2Faculty of Health, University Witten-Herdecke, Witten, Germany, 3Private Office, Bern, Switzerland, 4Stirling Community Hospital, Stirling, UK, 5Department of Dermatology, Bispebjerg & Frederiksberg Hospital, University of Copenhagen, Copenhagen, Denmark, 6Department of Dermatology, Miguel Servet University Hospital, IIS Aragón, Universidad de Zaragoza, Zaragoza, Spain, 7Hôpital Saint-Louis, Paris, France, 8Université de Paris, Paris, France, 9First Department of Dermatology and Venereology, School of Medicine, Aristotle University, Thessaloniki, Greece, 10Department of Dermatology, Bispebjerg Hospital, University of Copenhagen, Copenhagen, Denmark, 11Department of Dermatology, University of Brescia, Brescia, Italy, 12Department of Dermatology, ASST Spedali Civili di Brescia, Brescia, Italy, 13CentroDerm Wuppertal, Wuppertal, Germany, 14Medical Faculty, University of Zürich, Zürich, Switzerland, 15Dermatology Department, University Hospital of Zürich, Zürich, Switzerland, and 16Klinikum Vest GmbH, Knappschaftskrankenhaus Recklinghausen, Germany
Keratinocyte-derived skin cancers comprise basal cell carcinoma, squamous cell carcinoma, its precursor actinic keratosis, and Bowen’s disease. Historically, this group of neoplasms has been subsumed under the term non-melanoma skin cancer. However, the term non-melanoma skin cancer can be misleading and lacks precision. Therefore, more precise and reasonable terminology, valuing the relevance of keratinocyte-derived cancer, appears pertinent to meet its clinical and scientific significance. A group of experienced dermato-oncologists initiated a consensus approach to promote the use of the term “keratinocyte cancer” instead of “non-melanoma skin cancer” when referring to carcinomas and their precursors that are derived from keratinocytes. The vote among members of the consensus group indicated unanimous agreement on the consistent use of the term “keratinocyte cancer” instead of “non-melanoma skin cancer”. International delegates also voted in favour of the revised terminology. The more precise and, by means of etiopathogenesis, correct term “keratinocyte cancer” should be consistently used for malignancies originated from keratinocytes. This is expected to have a positive impact on patient–physician communication and gives better justice to this important group of keratinocyte-derived cancers.
SIGNIFICANCE
Different types of skin cancer originate from different cells in the body. In the most common type, cancer cells derive from cells building the superficial skin layer, called keratinocytes. To distinguish this type of skin cancer from pigment cell skin cancer called melanoma, it is summarized under the term “non-melanoma skin cancer”. However, the term is vague and misleading. Therefore, experts are proposing a name change that is expected to have a positive impact on communication between patient and doctor. In a vote among experts, the name change to “keratinocyte cancer” instead of non-melanoma skin cancer was unanimously approved.
Key words: consensus; keratinocyte cancer; non-melanoma skin cancer; actinic keratosis; squamous cell carcinoma; basal cell carcinoma.
Citation: Acta Derm Venereol 2024; 104: adv40601. DOI: https://doi.org/10.2340/actadv.v104.40601.
Copyright: 2024 © The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Apr 17, 2024. Accepted after revision: Jun 24, 2024. Published: Aug 5, 2024
Corr: PD Dr. med. Wolfgang G. Philipp-Dormston, Hautzentrum Köln (Cologne Dermatology), Schillingsrotter Str. 39–41, DE-50996 Köln, Germany. E-mail: mail@hautzentrum.com
INTRODUCTION
Keratinocyte-derived skin cancers comprise basal cell carcinoma (BCC), squamous cell carcinoma (SCC), its precursor actinic keratosis (AK), and Bowen’s disease, in situ forms of SCC. Associated with a tremendous medical and social burden, this group of neoplasms represents one of the most common malignancies in the Western world (1). In particular, people over 60 years of age are frequently affected (2). Based on German registry data, the age-standardized incidence in men and women is 122.4 and 152.2 per 100,000 (European standard), respectively (3). Due to underreporting of AK, the actual incidence might be even higher (4). Registry data from Denmark showed that BCC alone is as common as the sum of all other cancers (5). To distinguish BCC, SCC, and AK from melanoma-derived skin cancers, these neoplasms have been historically subsumed under the term non-melanoma skin cancer (NMSC). However, although the term NMSC has been around for decades, it can be misleading on several levels.
Foremost, a medical diagnosis, respectively a group of diagnoses that is defined by “what it is not”, in terms of “anything but melanoma” does not give the appropriate consideration and appreciation to this important group of malignancies and their precursors. On the contrary, the negation of relevance phenomenon leads to the impression of being non-important as negation is often considered a poorer form of meaning than affirmation (6, 7). The implication of negations has been debated among linguists and philosophers for millennia (6). In fact, that negative sentences are less valuable, less specific, and less informative than affirmative ones was first observed by Plato (8).
Furthermore, the term NMSC reveals a lack of clear definition and precision in the way it is commonly used by dermatologists and general practitioners. This is reflected in a search for the term “non-melanoma skin cancer” on PubMed. In total, 95% of the publications with that term in the title refer solely to keratinocyte cancers such as BCC, SCC, or AK. However, depending on the differing defining delineations of NMSC, the term also refers to other malignancies occurring within the epidermis, in the first instance Merkel cell carcinoma.
The British National Healthcare System (NHS) states, “Non-melanoma skin cancer refers to a group of cancers that slowly develop in the upper layers of the skin. The term ‘non-melanoma’ distinguishes these more common kinds of skin cancer from the less common skin cancer known as melanoma, which spreads faster in the body” (9). This statement leaves room for how to categorize Merkel cell carcinoma, which on the one hand originates in the “upper layer of the skin” but does not belong to “slowly” developing cancers that can be treated with “cryotherapy and creams” (9). In addition, the term NMSC is often used even more widely and is correspondingly vague, comprising all malignancies of the “skin” in terms of epidermis, dermis, and subcutis, including angiosarcoma, cutaneous B-cell lymphoma, cutaneous T-cell lymphoma, dermatofibrosarcoma protuberans, and sebaceous carcinoma (10).
Therefore, a more precise and reasonable terminology, valuing the relevance of keratinocyte-derived cancer, appears pertinent to meet its clinical and scientific significance. In Australia and New Zealand the term “keratinocyte cancer” is routinely used for this distinct group of skin cancers. This hereby proposed term, sporadically used in Europe, would be far more precise and applicable. In order to promote a revision in terminology for the group of keratinocyte-derived skin cancers in Europe, leading experts in the field of dermato-oncology have initiated a consensus approach.
MATERIALS AND METHODS
The objective was to obtain consensus on the consistent use of the term keratinocyte cancer instead of non-melanoma skin cancer when referring to carcinomas and their precursors that are derived from keratinocytes. In a first step, a lead group of European dermato-oncologists reviewed and amended the terms and definitions for the consensus approach. They formulated the rationale outlined in the introduction and 5 statements that were presented to the consensus group of 13 European experts in the field of keratinocyte derived cancers.
- i) The term “keratinocyte cancer” offers higher precision and therefore provides a more specific definition.
- ii) The term “keratinocyte cancer” better emphasizes the independence and uniqueness as its own entity or own group of skin cancers.
- iii) The term “keratinocyte cancer” better values the clinical and scientific significance, taking into consideration that this group of skin cancers is by far the most common and epidemiologically relevant.
- iv) The use of the specific term “keratinocyte cancer” might be favourable in patient communication. It might facilitate better patient understanding of the etiopathology, prevention measures, and therapy options. By introducing consistent new terminology, patient awareness might increase.
- v) Do you agree on the consistent use of the term “keratinocyte cancer” instead of “non-melanoma skin cancer”, when referring to carcinomas and their precursors that are derived from keratinocytes?
For questions i–iv members of the consensus group anonymously evaluated statements, indicating their agreement on a 5-point Likert scale (strongly agree/agree/neutral/disagree/strongly disagree). For the dichotomous question v, the members indicated their agreement by voting “yes” or “no”. Consensus was defined as 80% agreement among members. The criteria for participation in the consensus group comprised a great clinical as well as scientific experience in the field of dermato-oncology (ranging from 20 to 55 years) with a focus on keratinocyte-derived cancer as well as relevant participation in clinical trials, publications and academic teaching (Table I).
To gain the opinion of a broader group and to avoid potential bias by solely involving an expert group, in a second step the same polling questions were presented to European delegates during a panel at the 21st Euro-PDT conference (9–10 June 2023, Barcelona, Spain). Delegates could access the questions on their mobile phones via a QR code and place their votes.
RESULTS
The vote among members of the consensus group indicated unanimous agreement (100% strongly agree regarding questions i–iv, Fig. 1; 100% yes regarding question v, Fig. 2a). During the second step, a total of 112 delegates participated in the poll. Table II provides background information on the voters. Among the delegates, 97% agreed or strongly agreed that the term “keratinocyte cancer” offers higher precision and therefore provides a more specific definition. That the term “keratinocyte cancer” better emphasizes the independence and uniqueness as its own entity or own group of skin cancers was agreed or strongly agreed upon by 93% of delegates. A total of 87% agreed or strongly agreed that the term “keratinocyte cancer” better values the clinical and scientific significance, taking into consideration that this group of skin cancers is by far the most common and epidemiologically relevant. Overall, 64% agreed or strongly agreed on the following: The use of the specific term “keratinocyte cancer” might be favourable in patient communication. It might facilitate better patient understanding of the etiopathology, prevention measures and therapy options. By introducing consistent new terminology, patient awareness might increase (see Fig. 1). Finally, 89% of the delegates agreed on the consistent use of the term “keratinocyte cancer” instead of “non-melanoma skin cancer”, when referring to carcinomas and their precursors which are derived from keratinocytes (Fig. 2b). The final results for the publication were evaluated, discussed, and again consented on among the members of the consensus group and delegates in a special session at the annual congress of the European Academy of Dermatology and Venerology (EADV) in Berlin (October 2023).
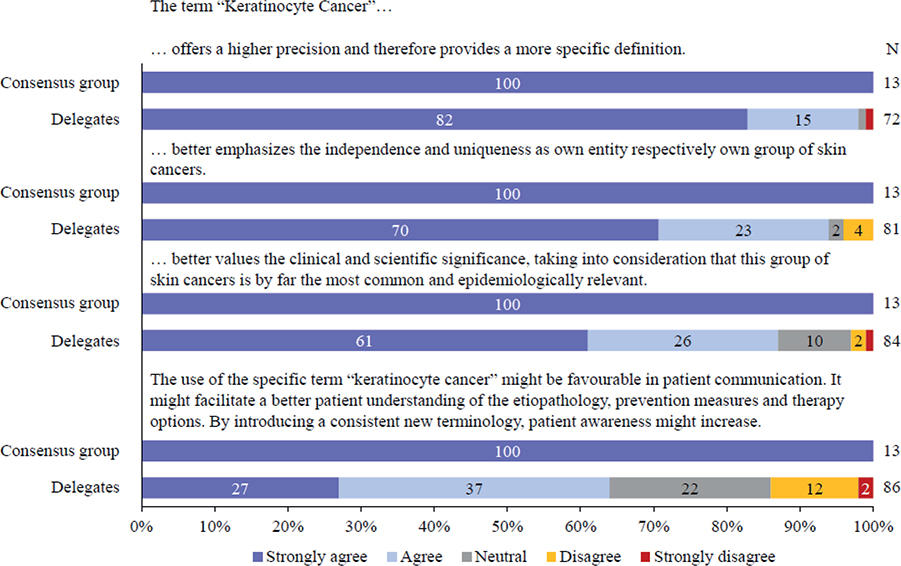
Fig. 1. Results from multiple choice polling questions i–iv presented to the consensus group and delegates at the 21st Euro-PDT conference (9–10 June 2023, Barcelona, Spain).
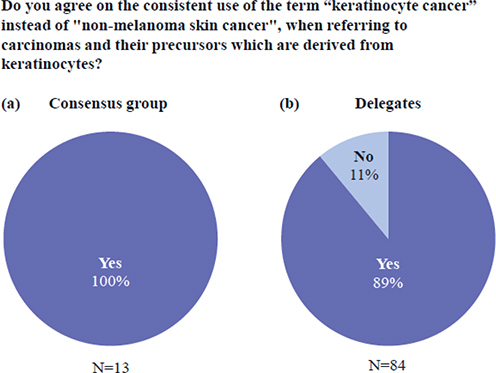
Fig. 2. Results from the dichotomous polling question v presented to (a) the consensus group and (b) delegates at the 21st Euro-PDT conference (9–10 June 2023, Barcelona, Spain).
DISCUSSION
A 100% consensus was reached among members of the consensus group on the consistent use of the term “keratinocyte cancer” instead of “non-melanoma skin cancer”, when referring to carcinomas and their precursors that are derived from keratinocytes. This was mirrored by the delegates who voted in favour of the proposed change.
While this terminology issue has been a matter of debate among dermato-oncologists for more than a decade, Europeans are not the first scientists to attempt a revision in terminology. The established use of revised terminology is reflected in a PubMed search, which delivers 132 results for the term keratinocyte cancer, almost all of them originating from Australia and New Zealand (October 2023). The term has been incorporated in the Cancer Council Clinical Guidelines from Australia (11) and is recognized by patients. In Europe, the term keratinocyte cancer has been used only sporadically. One example is the latest edition of Rooks Textbook of Dermatology (12). How urgently a consistent distinction of keratinocyte cancers from other NMSC is needed becomes apparent when dermatologists talk about NMSC, but mean keratinocyte cancer. To avoid a mix-up in treatment recommendations, disregard of keratinocyte-derived cancers, and trivialization of other cancers such as Merkel cell carcinoma, the consensus group strongly favours a change in terminology. Thus, the use of the accurate term keratinocyte cancer is expected to have a positive impact on patient–physician communications.
Furthermore, it would be logical to completely abandon the term NMSC in the future and to classify all groups of skin cancer according to their etiopathogenesis, e.g., melanoma, Merkel cell carcinoma, keratinocyte cancers (BCC, SCC, and its precursors), adnexal tumours, soft-tissue tumours (e.g., dermatofibrosarcoma protuberans), cutaneous lymphomas, etc. Further scientific considerations and consensus approaches are required. Adapting the International Statistical Classification of Diseases and Related Health Problems (ICD) could also be worth considering.
The unanimous agreement of the consensus group marks an important step in establishing more precise terminology and advancing understanding in patient and physician communication.
ACKNOWLEDGEMENTS
Funding sources: Medical writing assistance was provided by Dr Petra Jöstingmeyer (med:unit GmbH, Germany) and was funded by Galderma Laboratorium GmbH, Germany. The authors had full editorial control of the manuscript and provided their final approval.
Conflict of interest disclosures: WGP-D has been an adviser and/or received speakers’ honoraria and/or received grants and/or participated in clinical trials of the following companies: Almirall, Biofrontera, Galderma, German Medical Engineering, Leo Pharma, Photonamic, Pierre Fabre, and Schulz und Böhm. CAM reports receiving support for attending meetings and/or travel from Biofrontera and Galderma. He is a Board member of Euro-PDT. MH has been an adviser and/or received speakers’ honoraria and/or received grants and/or participated in clinical trials of the following companies: Cherry Imaging, Cynosure, Galderma, GME Medical, Leo Pharma, La Roche-Posay, Lutronic, MiraDry, Procter & Gamble, and Venus Concept. PC-P has been an adviser and/or received speakers’ honoraria and/or received grants and/or participated in clinical trials of the following companies: Abbvie, Galderma, Cantabria, Jannsen, Incyte, Sanofi, Almirall, and Sun Pharma. TD has received support for the present manuscript from Galderma. GH has been an adviser and/or received speakers’ honoraria and/or received grants and/or participated in clinical trials of the following companies: Abbvie, Amgen, Galderma, Johnson Johnson, LEO, Novartis, and Sanofi. RMS has received honoraria for lectures from Almirall, Beiersdorf, Galderma, and Pierre Fabre. He is vice-president of the EURO-PDT Society and a member of the German S3 Guideline Committee on Actinic Keratosis and Squamous Cell Carcinoma. LRB, YG, NB-S, ES, SRW, and HCW have no conflicts of interest to declare.
REFERENCES
- Lomas A, Leonardi-Bee J, Bath-Hextall F. A systematic review of worldwide incidence of nonmelanoma skin cancer. Br J Dermatol 2012; 166: 1069–1080. https://doi.org/10.1111/j.1365-2133.2012.10830.x
- Philipp-Dormston WG, Müller K, Novak B, Strömer K, Termeer C, Hammann U, et al. Patient-reported health outcomes in patients with non-melanoma skin cancer and actinic keratosis: results from a large-scale observational study analysing effects of diagnoses and disease progression. J Eur Acad Dermatol Venereol 2018; 32: 1138–1146. https://doi.org/10.1111/jdv.14703
- Krebs in Deutschland für 2017/2018. 13. Ausgabe. Robert Koch-Institut (Hrsg) und die Gesellschaft der epidemiologischen Krebsregister in Deutschland e.V. (Hrsg). Berlin, 2021.
- Katalinic A, Kunze U, Schäfer T. Epidemiology of cutaneous melanoma and non-melanoma skin cancer in Schleswig-Holstein, Germany: incidence, clinical subtypes, tumour stages and localization (epidemiology of skin cancer). Br J Dermatol 2003; 149: 1200–1206. https://doi.org/10.1111/j.1365-2133.2003.05554.x
- Holm AS, Nissen CV, Wulf HC. Basal cell carcinoma is as common as the sum of all other cancers: implications for treatment capacity. Acta Derm Venereol 2016; 96: 505–509. https://doi.org/10.2340/00015555-2282
- Horn LR, Wansing H. Negation. In: Zalta EN, Nodelman U, editors. The Stanford Encyclopedia of Philosophy (Winter 2022 Edition). The Metaphysics Research Lab, Philosophy Department, Stanford University, Stanford, CA.
- Ackrill J. Aristotle’s Categories and De Interpretatione. Oxford: Clarendon Press, 1963. https://doi.org/10.1093/actrade/9780198720867.book.1
- Plato. The Sophist, B. Jowett, trans. New York: Random House, 1937.
- National Healthcare System. Skin-cancer-non-melanoma. [Cited 8 Mar 2024] Available from: https://www.nhsinform.scot/illnesses-and-conditions/cancer/cancer-types-in-adults/skin-cancer-non-melanoma/#about-non-melanoma-skin-cancer.
- Amaral T, Garbe C. Non-melanoma skin cancer: new and future synthetic drug treatments. Expert Opin Pharmacother 2017; 18: 689–699. https://doi.org/10.1080/14656566.2017.1316372
- Cancer Council Australia Keratinocyte Cancers Guideline Working Party. Clinical practice guidelines for keratinocyte cancer. Sydney: Cancer Council Australia. [cited 2023 Oct 25]. Available from: https://wiki.cancer.org.au/australia/Guidelines:Keratinocyte_carcinoma.
- Gupta G, Dirschka T. Squamous cell carcinoma and its precursors. In: Griffiths C, Barker J, Bleiker T, Chalmers R, Creamer D, editors. Rook’s Textbook of Dermatology. 9th ed. Hoboken, NJ: Wiley-Blackwell, 2016.