QUIZ SECTION
Multiple Indolent Purplish Nodules and Plaques of the Extremities in an 85-year-old Man: A Quiz
Giulia COSCARELLA1,2*, Giorgia MERLINI3 and Mario Alessandri BONETTI4
1Dermatologia, Dipartimento Universitario di Medicina e Chirurgia Traslazionale, Università Cattolica del Sacro Cuore, IT-00168 Rome, 2Dermatologia, Dipartimento di Scienze Mediche e Chirurgiche, Fondazione Policlinico, Universitario A. Gemelli IRCCS, Rome, 3Pathology Unit, IRCCS Ospedale San Raffaele, Milan, and 4Department of Plastic Surgery, University of Milan, Milan, Italy. *E-mail: giuliacoscarella@gmail.com
Citation: Acta Derm Venereol 2024; 104: adv40664. DOI: https://doi.org/10.2340/actadv.v104.40664.
Copyright: © 2024 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Published: Sep 5, 2024
An 85-year-old male was examined for indolent red-purplish nodules and plaques, some of them ulcerated, located on the left arm and on the right lower limb (Fig. 1). The lesions first presented nearly a month before and they were asymptomatic but fast growing. No systemic symptoms were reported. Medical history included arterial hypertension, under treatment with ACE inhibitors, and benign prostatic hyperplasia. Physical examination showed right inguinal palpable and painless lymphadenopathy. Laboratory tests, including blood count, liver and kidney function, inflammatory markers, and serum protein electrophoresis, were within normal limits except for a mild increase in C-reactive protein levels (CRP).
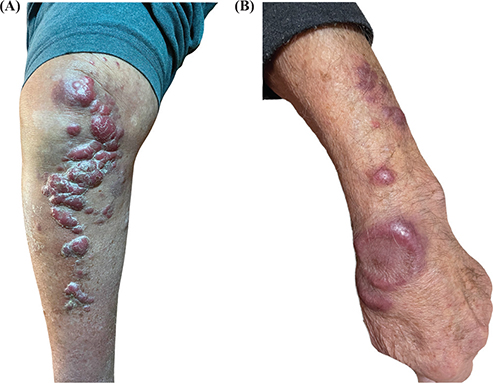
Fig. 1. (A) Indolent red-purplish nodules and plaques on the right lower limb. (B) Indolent red-purplish nodules and plaques on the left arm.
Positron emission tomography/computed tomography demonstrated one uptaking right inguinal lymph node of 1.9 cm in diameter. An incisional skin biopsy of the lesions in the lower extremities was performed and showed atypical lymphocytes CD20+ predominantly infiltrating dermis and subcutaneous tissue, while no epidermotropism was observed. In addition, positivity of Bcl2 and Bcl6 was shown in B-cells.
What is your diagnosis?
Differential diagnosis 1: Primary cutaneous diffuse large B-cell lymphoma (PC-DLBCL)
Differential diagnosis 2: Kaposi sarcoma
Differential diagnosis 3: Non-tuberculous mycobacterial infection
Differential diagnosis 4: Primary cutaneous follicular helper T-cell lymphoma
See next page for answer.
ANSWERS TO QUIZ
Indolent Multiple Purplish Nodules and Plaques of the Extremities: A Commentary
Diagnosis: Primary cutaneous diffuse large B-cell lymphoma
Primary cutaneous diffuse large B-cell lymphoma (PCD-LBCL) is an aggressive subtype of cutaneous B-cell lymphoma that typically occurs at the lower extremities (1). Clinical presentation may include macules, solitary or multiple nodules, or papules, which may ulcerate or coalesce to form plaques with infiltrated borders, covering even large areas (2). Tumour growth is usually rapid and involves either the lower or upper extremity with mono- or bilateral distribution. However, the simultaneous involvement of multiple body regions is rare. PCDLBCL at initial stage usually presents without clinical signs of extracutaneous dissemination.
There are no pathognomonic diagnostic clues allowing the clinical diagnosis of PCDLBCL, thus histological examination is mandatory. PCLBCL is characterized by a dense dermal infiltrate with a diffuse and/or nodular pattern composed of > 80% large tumour cells corresponding to centroblasts and/or immunoblasts, with numerous mitoses and a proliferative index > 39% (3). No epidermotropism or lymphocyte infiltration is generally observed (4). Immunohistochemistry demonstrates BCL2 amplification in PCLBCL (Fig. 2).
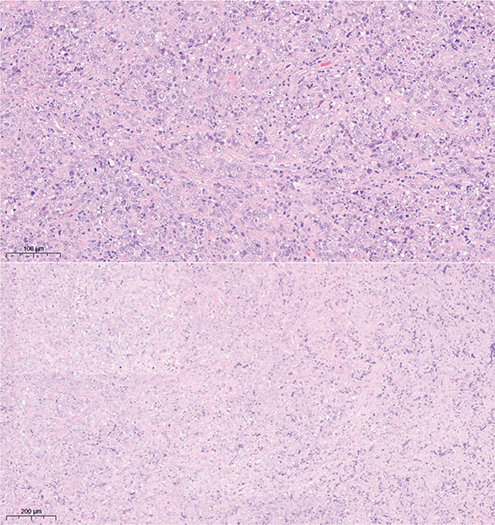
Fig. 2. Histopathologic representation of primary cutaneous diffuse large B-cell lymphoma.
The morphology and distribution of skin lesions sometimes provide crucial information guiding physicians towards the diagnosis, even though various conditions may share similar clinical presentations. PCDLBCL presents similarities to Kaposi sarcoma (KS). KS is an angioproliferative disorder generally presenting as violaceous papules or plaques and ulcerated nodules, predominantly localized at the lower extremities (5). KS is characterized by the proliferation of oddly shaped endothelial cells, which may occur in the elderly (6).
In our patient, the age and the presence as well as the site of the purplish nodules could have suggested KS. Dermoscopy constitutes a useful diagnostic tool to identify typical dermoscopic features related to KS, such as the rainbow pattern or the presence of serpentine vessels (5).
Another potential consideration for the differential diagnosis is the primary cutaneous follicular T-cell lymphoma (PCTL), which is characterized by numerous red, infiltrated, and non-ulcerated papules, plaques, and nodules, mainly appearing on the chest, extremities, or in the head and neck region (7). The classic histology of PCTL includes a dense dermal presence of CD3+ T and CD20+ B cells, which do not penetrate the epidermis (7). Immunohistochemistry can help in confirming PCTL by demonstrating BCL6 and CD10 expression (7).
An additional alternative in the spectrum of differential diagnosis could be a non-tuberculous mycobacteriosis (NTM), which is an opportunistic cutaneous infection caused by pathogens different from Mycobacterium tuberculosis or Mycobacterium leprae. NTMs may have a variable clinical presentation mainly including erythematous papular-nodular lesions, often complicated by ulceration. Among all species, Mycobacterium marinum infection may lead to the outbreak of violaceous nodular lesions localized at the extremities due to the contact with aquatic environments (8). Systemic manifestations such as pulmonary disease, lymphadenopathy, and disseminated disease usually occur along with skin and soft tissue disease. Fever, night sweats, weight loss, and hepatosplenomegaly are the most frequent systemic manifestations. Culture of skin specimens is the primary diagnostic examination, despite its low specificity (8).
In our patient, on the basis of histological diagnosis of PCDLBCL, systemic chemotherapy was started. Skin lesions on both upper and lower extremities regressed after the first cycle of R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) and systemic therapy was consequently interrupted. At 3-month follow up, lesions recurred and a second cycle of R-CHOP was carried out.
Treatment strategies for PCDLBCL vary based on the patient’s age, the International Prognostic Index (IPI), and the feasibility of intensified dosing approaches. In patients aged 60 to 80 years, the standard of care is typically represented by 8 cycles of chemotherapy combining a CHOP regimen with rituximab. For patients who are 80 years and older, it is advisable to opt for an attenuated CHOP regimen (9).
REFERENCES
- Willemze R, Cerroni L, Kempf W, Berti E, Facchetti F, Swerdlow SH, et al. The 2018 update of the WHO-EORTC classification for primary cutaneous lymphomas. Blood 2019; 133: 1703–1714. https://doi.org/10.1182/blood-2018-11-881268
- Lara-Endara J, Montalvo N, Redroban L, Mushtaq A. Primary cutaneous diffuse large B-cell lymphoma, leg type mimicking subcutaneous panniculitis-like T-cell lymphoma in a COVID-19 setting: case report and review of literature. Dermatol Online J 2021; 27(12). DOI: 10.5070/D3271256703. https://doi.org/10.5070/D3271256703
- Swerdlow SH, Campo E, Pileri SA, Harris NL, Stein H, Siebert R, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood 2016; 127: 2375–2390. https://doi.org/10.1182/blood-2016-01-643569
- Cretella P, Peluso AL, Picariello C, Cozzolino I, Triggiani M, Puzziello A, et al. Immunohistochemical algorithms and gene expression profiling in primary cutaneous B-cell lymphoma. Pathol Res Pract 2022; 231: 153804. https://doi.org/10.1016/j.prp.2022.153804
- Pileri A, Orioni G, Zengarini C, Grandi V, Piraccini BM, Gaspari V. Violaceous lesions on the leg: what else apart from Kaposi sarcoma? Differential diagnosis with a narrative review of the literature. Dermato 2023; 3: 56–68. https://doi.org/10.3390/dermato3010005
- Micali G, Nasca MR, De Pasquale R, Innocenzi D. Primary classic Kaposi’s sarcoma of the penis: report of a case and review. J Eur Acad Dermatol Venereol 2003; 17: 320–323. https://doi.org/10.1046/j.1468-3083.2003.00747.x
- Battistella M, Beylot-Barry M, Bachelez H, Rivet J, Vergier B, Bagot M. Primary cutaneous follicular helper T-cell lymphoma: a new subtype of cutaneous T-cell lymphoma reported in a series of 5 cases. Arch Dermatol 2012; 148: 832–839. https://doi.org/10.1001/archdermatol.2011.3269
- Nogueira LB, Garcia CN, Costa MSCD, Moraes MB, Kurizky PS, Gomes CM. Non-tuberculous cutaneous mycobacterioses. An Bras Dermatol 2021; 96: 527–538. https://doi.org/10.1016/j.abd.2021.04.005
- Sokol L, Naghashpour M, Glass LF. Primary cutaneous B-cell lymphomas: recent advances in diagnosis and management. Cancer Control 2012; 19: 236–244. https://doi.org/10.1177/107327481201900308