ORIGINAL REPORT
Secukinumab Reduces Psoriasis-associated Pruritus and Regenerates the Cutaneous Nerve Architecture: Results from PSORITUS a Double-blind, Placebo-controlled, Randomized Withdrawal Phase IIIb Study
Lina RENKHOLD1,2, Manuel P. PEREIRA3,4, Karin LOSER5, Dieter METZE1, Daniel BAEUMER6, Nima MELZER6, Maximilian REINHARDT7, Athanasios TSIANAKAS8, Thomas LUGER1, Christian MESS9, Ruth BECKER1,2, Clara HAMBÜCHEN1,2, Konstantin AGELOPOULOS1,2 and Sonja STÄNDER1,2
1Department of Dermatology, University Hospital Münster, Münster, Germany, 2Center for Chronic Pruritus, University Hospital Münster, Münster, Germany, 3Institute of Allergology, Charité – Universitätsmedizin Berlin, corporate member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Berlin, Germany, 4Fraunhofer Institute for Translational Medicine and Pharmacology ITMP, Allergology and Immunology, Berlin, Germany, 5Institute of Immunology, University of Oldenburg, Oldenburg, Germany, 6Novartis Pharma GmbH, Nuremberg, Germany, 7Novartis Pharma AG, Basel, Switzerland, 8Fachklinik Bad Bentheim, Department of Dermatology, Bad Bentheim, Germany, and 9Department of Dermatology and Venereology, University Medical Center Hamburg-Eppendorf, Hamburg, Germany
The occurrence of pruritus in psoriasis was previously underestimated but is a significant burden. Secukinumab (SEC), a monoclonal anti-interleukin-17A antibody, efficiently controls signs of psoriasis, but the effect on pruritus and cutaneous neuroanatomy remained unknown. The primary objective of this study (NCT02362789) was to evaluate the superiority of SEC treatment vs placebo on pruritus intensity (visual analogue scale; VAS). Furthermore, the treatment-dependent course of pruritus in association with absolute Psoriasis Area Severity Index (PASI) score, as well as cutaneous histopathology and neuroanatomy, was assessed. Open-label SEC 300 mg s.c. was administered regularly until week 16. Patients who reached a ≥ 98% PASI reduction (PASI ≥ 98) were randomized to receive either placebo or SEC up to week 32. Punch biopsies were collected from lesional psoriatic (baseline, weeks 16 and 32) and non-lesional (baseline) skin for histopathological and neuroanatomical analyses. VAS scores improved significantly after open-label SEC treatment but relapsed upon placebo (29.92 ± 33.8) compared with SEC (12.30 ± 22.6; p = 0.036). After SEC-dependent improvement in PASI, histopathology, marker expression and neuroanatomy, relapse was observed with treatment discontinuation in all parameters except neuroanatomy. SEC was superior to placebo by efficiently controlling reduced pruritus intensity, clinically normalizing skin lesions, and reversing histopathological abnormalities. The neuroanatomy recovered upon SEC and remained stable even after withdrawal.
SIGNIFICANCE
Pruritus is a previously underestimated burden in psoriasis. Secukinumab has shown promising results in the treatment of psoriasis, but the long-lasting effect on pruritus and the associated neuroanatomy is unclear. Pruritus intensities, psoriasis-associated marker expression, and nerve fibre architecture improved during secukinumab treatment in this study. After randomized withdrawal, pruritus intensity, Psoriasis Area Severity Index score, histopathological characteristics, and marker expression relapsed upon placebo compared with secukinumab, except for neuroanatomy. For the first time, secukinumab was shown to improve pruritus intensity in line with cutaneous nerve architecture. After discontinuation of the drug, the neuroanatomy remained stable, even while the pruritus began to relapse.
Key words: neuroanatomy; pruritus; psoriasis; therapy.
Citation: Acta Derm Venereol 2024; 104: adv40737. DOI https://doi.org/10.2340/actadv.v104.40737.
Copyright: © 2024 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: May 10, 2024; Accepted after revision: Oct 21, 2024; Published: Nov 20, 2024
Corr: Sonja Ständer; Department of Dermatology and Center for Chronic Pruritus, University Hospital Münster, Von-Esmarch-Str. 58, DE-48149 Münster, Germany. E-mail: sonja.staender@ukmuenster.de
Competing interests and funding: SST was a speaker and/or consultant and/or investigator and/or has received research funding from Abbvie, Almirall, Beiersdorf, BMS, Clexio, Eli Lilly, FomF, Galderma, German Research Foundation (DFG), Integrity CE, Kiniksa, Leo Pharma, L’Oréal, MEDahead, Moroscience, NACCME, Novartis, Omnicuris, P.G. Unna Academy, Pfizer, Sanofi, TouchIME, UCB, Vifor, and WebMD. MPP is an investigator for Allakos, Celldex Therapeutics, Incyte, Sanofi, and Trevi Therapeutics; and has received consultant and/or speaker honoraria and/or travel fees from AbbVie, Beiersdorf, Eli Lilly, GA2LEN, Galderma, Menlo Therapeutics, Novartis, P.G. Unna Academy, Sanofi, and Trevi Therapeutics. KL was a speaker and/or consultant and/or investigator and/or has received research funding from Amgen, Biogen, Dr. Wolff Arzneimittel, Estée Lauder, the German Research Foundation (DFG), Janssen, Kiniksa, Leo Pharma, Novartis, and TEVA. DB was an employee of Novartis Pharma GmbH Germany. NM is an employee of Novartis Pharma GmbH Germany. MR is an employee of Novartis Pharma AG Switzerland. All other authors have no conflicts of interest to declare.
The study was funded by Novartis Pharma GmbH Germany and supported by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) – FOR 5211 SOMACROSS and FOR 2690 PruSearch. Open access publication was funded by the Open Access Publication Fund of the University of Münster.
INTRODUCTION
For a long time, pruritus in psoriasis was underestimated, but presents a significant burden in up to 90% of patients (1, 2). The symptom is mainly located within lesions and of moderate intensity. However, pruritus can contribute to the development of mental comorbidities including anxiety, feelings of stigmatization, and depression (3–5). Consequently, improvement of pruritus with anti-psoriatic treatment leads to an improvement in the quality of life of patients (6, 7). The pathogenesis of pruritus in psoriasis is not well understood. It is assumed that an interaction of inflammatory Th1/Th17/Th22 mediators and cutaneous sensory nerves contributes to the development of the itch signal and to its chronicity (8–11). Additionally, interaction of sensory nerves and macrophages initiated by reactive oxygen species and subsequent release of neurotransmitters like substance P (SP), or calcitonin gene-related peptide (CGRP), was shown to mediate psoriasis-related cutaneous inflammation in a murine psoriasis model (12). Considering this broad involvement of cutaneous sensory nerve fibres in psoriasis, previous studies on the cutaneous neuroanatomy show conflicting data, with both reduced and enhanced epidermal nerve fibre numbers being reported in human psoriatic skin, possibly due to methodological discrepancies (13–16). In other pruritic conditions of inflammatory and neuropathic origin a reduction of intraepidermal nerve fibres was found (17, 18), but longitudinal studies on neuroanatomical alterations in psoriasis patients as well as on the relationship between pruritus and cutaneous neuroanatomy under treatment are still lacking. In addition, it is unclear whether pruritus recurs after normalization of the cutaneous neuroanatomy.
General disease control with secukinumab (SEC), the first approved human monoclonal IL17A antibody for psoriasis treatment, is already linked to pruritus relief (19, 20). Additionally, there is evidence that IL17A (overexpressed in psoriatic skin [21]) may have a neuromodulatory effect, either through direct influence on nerve fibres or secondarily through its pro-inflammatory properties (22). This study was designed to assess the impact of SEC treatment and withdrawal on the course of pruritus intensity in association with the neuroanatomy in psoriasis patients.
MATERIALS AND METHODS
Study design and patient population
PSORITUS (Secukinumab study in PSOriasis exploring pruRITUS) was a phase IIIb multicenter trial (NCT02362789) including both an open-label (OL) run-in phase (weeks 1–16) and a subsequent randomized placebo-controlled withdrawal (RW) phase (weeks 16–32) with monthly injections of SEC 300mg s.c. or placebo up to week 32, respectively (Fig. S1A).
Patients were adults with moderate to severe plaque psoriasis (Psoriasis Area Severity Index [PASI] > 10) and moderate to severe pruritus intensity of ≥ 30 on a 100-point visual analogue scale (VAS). Key exclusion criteria are described in Appendix S1.
All patients received OL SEC at baseline, weeks 1, 2, 3, and 4 and then every 4 weeks until week 16. Patients who did not reach a ≥ 98% reduction in the PASI score (PASI ≥ 98) discontinued the study after the OL phase. This cut-off ensures an excellent response and extensive skin clearance of patients without losing those who do not achieve a 100% PASI reduction. Patients (PASI ≥ 98 reduction) were randomized 1:1 until week 32 to either 4-weekly placebo or SEC, with patients and investigators blinded to study treatment (Fig. S1B). Safety data of SEC are shown in Table SI.
Primary objective: Evaluation of superiority of SEC vs placebo on pruritus intensity (worst itch within 24 h [WI-VAS-24h]) at week 32.
Exploratory objectives: Assessment of treatment-dependent course of pruritus in association with absolute PASI, histopathology and cutaneous neuroanatomy in lesional and non-lesional skin before, during and after treatment.
PSORITUS was performed in accordance with the Guidelines for Good Clinical Practice, with applicable local regulations (including European Directive 2001/20/EC), and with ethical principles laid down in the Declaration of Helsinki. Written informed consent was obtained from all participants.
Biopsies and histological analyses
Punch biopsies (4–6 mm diameter) were collected from lesional psoriatic plaques (LS) and non-lesional (NL) skin preferentially at the trunk (alternatively at extremities) in local anaesthesia at baseline (n = 130) and from LS skin at weeks 16 (n = 80) and 32 (n = 57) (Fig. S1a). Skin samples were frozen in OCT (optimal cutting temperature compound) medium for histopathology and immunohistochemical staining. Haematoxylin/eosin as well as periodic acid-Schiff-stained paraffin sections were analysed regarding histopathological changes. Immuno-peroxidase staining was performed on paraffin sections with CK16 and S100A7 antibodies. Biopsies were scored semi-quantitatively by 2 investigators (SST, DM) blinded to treatment groups.
Cutaneous neuroanatomy
Intraepidermal nerve fibre density (IENFD) was analysed by assessing the number of PGP9.5-positive nerve fibres crossing the basement membrane per mm epidermis. Samples were processed according to the validated and previously reported protocol (23) (Appendix S1). Absolute intraepidermal nerve fibre length (IENFL) was determined generating 3 z-stacks (26 individual images, 20 µm range) per patient per time point. The open-source software DeconvolutionLab2 (24) was used to deconvolve the image stacks into tagged image file format (TIFF) files for further analysis (see Fig. S6A). Morphometric evaluation of epidermal nerve fibres was performed using the software NeuroM/Blue Brain Project (25) (see Fig. S6B). Epidermis height was assessed by determining the distance between basement membrane and stratum corneum. For the longitudinal observations only, localization-matched biopsies were used.
Statistical analyses
The study sample size was calculated based on previous data from the FIXTURE Study (CAIN457A2303) (26) as described in the Appendix.
The primary analysis method was testing differences between the placebo and the SEC group for significance using a t-test. Missing values of VAS or PASI were imputed with the median value of the entire group at the corresponding timepoint.
Non-parametric tests were used for data without normal distribution. Paired samples were compared by Wilcoxon’s rank sum test; data of independent groups were tested with the Kruskal–Wallis test or Mann–Whitney test, as appropriate. Correlations were calculated with Spearman’s correlation coefficient test. All calculations were performed using SPSS 27 software (IBM Corp, Armonk, NY, USA) and two-sided p-values of p < 0.05 were considered statistically significant.
RESULTS
Patient population
In total, 146 patients with psoriasis vulgaris were screened, 130 of whom entered the OL run-in phase receiving SEC (16 weeks). The OL phase was completed by 128 patients (98.5%). Fifty of 130 subjects failed run-in, discontinued treatment, and were not re-randomized to the RW phase (48 failed to reach PASI ≥ 98; 1 discontinuation due to adverse events [AE]; 1 death). Eighty (61.5%) out of 130 SEC-treated subjects achieved extensive skin clearance (PASI ≥ 98) and qualified for the subsequent RW phase (weeks 16–32). These subjects were randomized to receive either SEC (n = 42) or placebo (n = 38) (Fig. S1B). A higher proportion of patients discontinued in the placebo group 12/38 (31.6%) as compared with the SEC group 4/42 (9.5%), the major reason for which was lack of efficacy (6 placebo- and 2 SEC-treated patients).
Baseline characteristics (previously published for the initial 130 patients [7]) were balanced between RW SEC- and placebo-treatment groups (Table I). Baseline PASI was 23.4 ± 10.5 for SEC-treated and 24.2 ± 12.4 for placebo-treated patients, with the majority in both groups (> 90%) having an Investigator’s Global Assessment (IGA) modified 2011 score 3/4, indicative of moderate to severe disease. Average of baseline WI-VAS-24h was 74.8 ± 18.0 for the SEC group and 76.1 ± 20.1 for placebo. Safety of SEC in PSORITUS was consistent with previous phase III clinical trials and no new or unexpected safety signals emerged (Table SI). There was 1 death that resulted from rupture of a pre-existing infra-renal aortic aneurysm after the first 4 doses of SEC and was considered unrelated to study treatment. One patient had an AE leading to discontinuation of study treatment and 7 patients had non-fatal serious AEs.
Pruritus and skin lesions improve with secukinumab
This analysis was performed based on 33 SEC- and 24 placebo-treated patients with complete data sets available. In the OL phase, baseline pruritus intensity (WI-VAS-24h; mean ± SD) of 74.39 ± 19.2 rapidly reduced and reached significance after 1 week of treatment (60.04 ± 27.5; p < 0.001). Pruritus intensity continued to improve up to week 16 with a mean WI-VAS-24h of 6.47 ± 13.0 (p < 0.001; Fig. S2A). At week 32, the primary endpoint was met with significantly lower pruritus intensity in SEC-treated patients than in the placebo group (12.30 ± 22.6 vs 29.92 ± 33.8; p = 0.036; Fig. 1A). By week 16, rates of PASI 75/90/100 response were 92.0%, 77.9%, and 33.6%, in line with previous phase III studies (26) (Fig. S2C). Low absolute PASI scores achieved during the OL phase (Fig. S2B) were maintained with SEC up to week 32 with a mean of 1.28 ± 2.2 compared with placebo (4.07 ± 4.3; p = 0.008; Fig. 1B). It is noteworthy that, despite the relapse in the placebo group in terms of both pruritus intensity and PASI scores, levels at week 32 were lower compared with baseline.
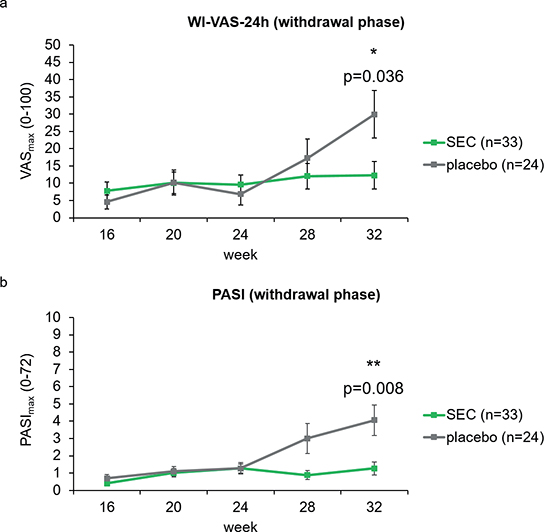
Fig. 1. Pruritus intensity and disease activity following secukinumab treatment (randomized withdrawal phase). (A) Assessment of clinical parameters during the RW phase including worst pruritus intensity (WI-VAS-24h score, placebo v SEC: p = 0.036, and (B) absolute PASI score (placebo versus SEC: p = 0.008. Data are shown as mean (SE). PASI: Psoriasis Area Severity Index, RW: randomized withdrawal, SE: standard error, SEC: secukinumab, WI-VAS-24h: worst itch of the previous 24 h assessed using a visual analogue scale (0–100mm). Statistics: t-test *p < 0.05, **p < 0.01.
The course of pruritus intensity paralleled the course of absolute PASI scores in the RW phase and is supported by increasing correlations in the SEC as well as the placebo group (Table SII).
Histopathological changes normalize with secukinumab
Psoriasis-related histopathological changes were proportionally categorized into absent, weakly present, present, and strongly present (Fig. S3). LS skin showed typical psoriatic features with hyperkeratosis, hyperplasia, dilated blood vessels, neutrophils in the horny layer and papillary oedema as well as weakly present erythrocyte extravasation compared with NL skin. All biopsies showed progressive normalization of assessed disease-specific pathologic changes upon OL SEC treatment. After treatment withdrawal with placebo, recurrence of psoriasis was associated with a reversion of previous psoriasis-related histomorphological transformations at week 32 compared with week 16 (Fig. S3B, C, E, F). In the placebo group (week 32) blood vessels dilated again (0 [0;1.8]) vs the SEC group (0 [0;0]; p < 0.01), neutrophils recurred to be present in the horny layer (placebo 0 [0;1.8] vs SEC 0 [0;0]; p = 0.005) and erythrocytes extravasated (placebo 0 [0;1.0] vs SEC 0 [0;0]; p = 0.028). Recurrence of hyperkeratosis and hyperplasia was also observed with placebo, but without significantly differing from the SEC group (Fig. S3A, D). The course of treatment-dependent histopathological changes in psoriatic skin lesions is visualized by representative haematoxylin/eosin staining (Fig. S4).
Cutaneous expression of psoriasis-associated markers normalizes with secukinumab
To further sustain our histopathological findings, we analysed cutaneous expression of disease-related markers including a semi-quantitative rating (median [interquartile range]) of histochemical staining from 0 to 5 (gradually from negative to strongly positive). At baseline, investigated markers CK16 and S100A7, 2 epidermal barrier proteins impaired in psoriasis, showed significantly increased expression levels in LS compared with NL skin (Fig. S5). CK16 showed SEC-associated decline of expression levels in LS skin until week 16. At week 32, expression in the placebo group (1.0 [0.6;2.0]) is significantly increased compared with the SEC group (CK16: 0.0 [0.0;0.4], p = 0.004). Equal improvements in S100A7 expression were observed upon OL SEC treatment. Placebo led to increased S100A7 expression (week 32: 3.5 [0.6;4.4]), whereas low expression was maintained with SEC (0.5 [0.0;1.4]; p = 0.03).
A moderate positive correlation was found between pruritus intensity at baseline and both CK16 (r = 0.402, p = 0.029, n = 19) and S100A7 (r = 0.426, p = 0.027, n = 18) expression of LS skin. At week 16, pruritus intensity correlated only with CK16 expression (r = 0.705, p < 0.001, n = 19). CK16 expression of the SEC group correlated significantly with PASI scores (r = 0.720, p = 0.006, n = 12) at week 32.
Cutaneous neuroanatomical changes recover upon secukinumab treatment
Cutaneous neuroanatomy was analysed by determining IENFD and IENFL (Table II). Only patients with every biopsy taken from the same areas were evaluated (n = 47). Furthermore, IENFD of all time points was normalized to NL skin at baseline. IENFD in LS skin at baseline was significantly reduced compared with treated LS skin at week 16 and, irrespective of treatment, at week 32 (Fig. 2A).
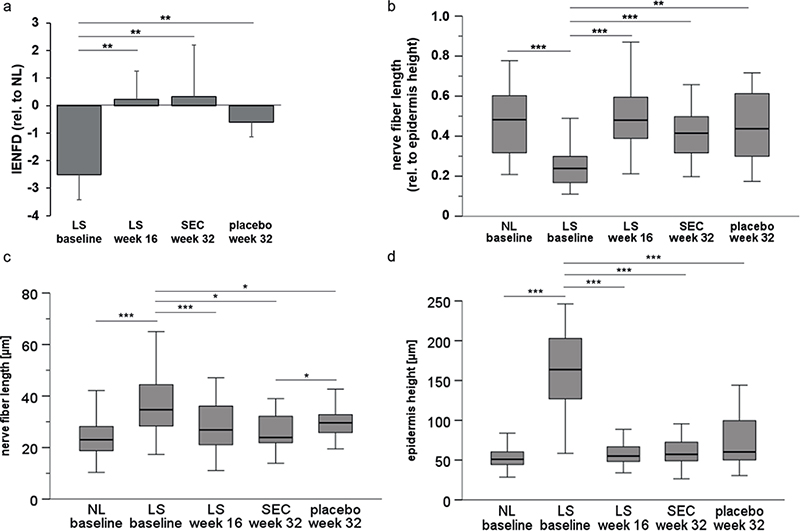
Fig. 2. Intraepidermal nerve fibre density and length recover upon secukinumab treatment. (A) IENFD of LS skin at baseline (n = 47), week 16 (n = 47) and 32 (SEC: n = 29; placebo: n = 18) normalized to NL skin at baseline. IENFD in LS skin at baseline is significantly decreased and recovers upon SEC treatment until week 16 (OL phase, p = 0.004) and remains stable during RW phase (until week 32, p = 0.023). (B) IENFL relative to the epidermal height. LS skin at baseline differing significantly (p < 0.001) from NL skin (baseline; n = 47) and LS skin after secukinumab treatment at week 16 (n = 47) and 32 (SEC: n = 29; placebo: n = 18). (C) Absolute IENFL in µm at every time point (n = 47; SEC: n = 29; placebo: n = 18). (D) Epidermis height in µm at every time point (n = 47; SEC: n = 29; placebo: n = 18). IENFD: intraepidermal nerve fibre density, IENFL: intraepidermal nerve fibre length, LS: lesional skin, NL: non-lesional skin, OL: open-label, RW: randomized withdrawal phase, SEC: secukinumab. Statistics: Wilcoxon test *p < 0.05, **p < 0.01, ***p < 0.001.
Absolute IENFL [µm] was significantly increased in LS skin at baseline compared with NL skin and LS skin after both OL and RW phase (Fig. 2C). Epidermis height showed analogous alterations such as the IENFL (Fig. 2D).
To eliminate potential bias due to epidermal hyperplasia, we additionally analysed the IENFL relative to the epidermal height, resulting in significantly decreased IENFL in LS skin at baseline (0.24 [0.17;0.30]) compared with NL skin (0.48 [0.32;0.61]; p < 0.001). Relative IENFL increased in LS skin with SEC treatment (0.48 [0.39;0.60]; p < 0.001) and was maintained irrespective of treatment withdrawal (SEC: 0.42 [0.31;0.50], p < 0.001; placebo: 0.44 [0.28;0.61], p = 0.003; Fig. 2B).
Considering pruritus, a weak negative correlation at baseline was observed in LS skin between WI-VAS-24h and IENFD (r = -0.207, p = 0.039) and relative IENFL (r = –0.320, p = 0.039), respectively. Further negative correlations were found between IENFD after the OL phase at week 16 and both PASI at baseline (r = –0.289, p = 0.004) and week 16 (r = –0.286, p = 0.01).
DISCUSSION
In this phase IIIb randomized, double-blind, placebo-controlled trial (NCT02362789) the therapeutic effect of SEC on pruritus intensity in accordance with cutaneous neuroanatomy in psoriasis patients was successfully demonstrated. SEC was the first approved “first line label” biologic targeting IL17A (27) in psoriasis showing great efficacy. Today, other suitable alternatives such as ixekizumab (targeting IL17A) or brodalumab (targeting IL17A receptor) are also available (28). Patients receiving SEC showed, as expected, a significant reduction in itch intensity and PASI scores. In the withdrawal phase, both pruritus and PASI remain stable for 8 weeks and recur from week 12 onwards in the placebo arm, while SEC continues to control pruritus and PASI over the entire period. At the primary endpoint (week 32), SEC-treated patients showed significant superiority regarding pruritus intensity compared with the placebo group. This shows a stable effect of SEC on pruritus intensity and PASI, which even lasted for several weeks after discontinuation of therapy.
Psoriasis-related histopathological alterations in lesional skin recovered upon SEC therapy in line with clinical healing of lesions. After SEC discontinuation (placebo-group), the histopathological characteristics worsened paralleled to PASI scores and pruritus intensity, underlining that psoriatic inflammation might induce and maintain pruritic sensations. In this context, it has been shown previously that expression of well-known psoriasis markers such as IL23 correlates with pruritus intensity (11). To fortify further the relevance of histopathological changes, we analysed the expression of the psoriasis-associated markers CK16(29) and S100A7(30) by immunohistochemical staining. CK16 is associated with epidermal barrier integrity and showed histologically increased expression in psoriatic lesional skin reinforcing previous reports (31, 32). Expression of CK16 normalized due to SEC treatment consistent with a previous study (33) and may be related to improvement of skin lesions. S100A7 was already shown to suppress extracellular matrix production (34) and was found to be upregulated in psoriatic lesional skin in line with Nattkemper et al. 2018 (16) but also normalized with SEC treatment. The expression of both CK16 and S100A7 in lesional skin at baseline correlated moderately with the maximum pruritus intensity at baseline and additionally we observed a strong correlation of CK16 expression and pruritus intensity after OL SEC treatment. Therefore, there may be a relation of assessed markers and pruritus that has so far not been sufficiently investigated. Furthermore, both analysed markers showed increased expression levels in the placebo group compared with the SEC group (week 32) in accordance with worsening of pruritus intensity, PASI, and histopathological characteristics, highlighting the potential interplay between the assessed parameters.
In consideration of cutaneous neuroanatomy in psoriatic skin lesions, decreased IENFD and reduced IENFL relative to the epidermal height was found at baseline as compared with non-lesional skin. The finding of rarefication of intraepidermal nerve fibres in psoriatic skin is consistent with previous observations in psoriasis (13, 14, 16) and in other pruritic inflammatory conditions such as atopic dermatitis or chronic nodular prurigo (17, 18). However, other studies in psoriasis showed higher IENFD in psoriatic skin. This discrepancy may be explained by different IENFD assessment methodology analysing the number of intraepidermal nerve fibre fragments per mm2 epidermis (15) instead of the number of nerve fibres crossing the dermal–epidermal junction. Another explanation might be the analysis of different examined localizations (35) that seem to influence the density (Fig. S6C). Increased absolute IENFL at baseline is in line with a previous reported finding (36). Additionally, increased epidermal height in psoriatic lesions (vs non-lesional skin) may possibly indicate a hyperplasia-associated elongation of nerve fibres. However, due to increased thickness of the skin, a lower innervation depth was achieved in lesional skin, which was reflected in a reduced relative IENFL.
SEC treatment led to a recovery of IENFD and relative IENFL, which remained stable even in the placebo group after SEC discontinuation, in contrast to all other assessments in this study. Whether IL17A inhibition by SEC influences neuronal regeneration directly or indirectly through the general healing process, as previously shown in chronic prurigo patients (23), is not yet clear. The negative correlation between IENFD and relative IENFL in psoriatic skin and pruritus intensity at baseline as well as subsequent therapy-dependent parallel reduction of pruritus and recovery of IENFD/L indicate that neuroanatomical structure and its changes may contribute to pruritus. However, recurrence of pruritus along with the disease is thus not primarily due to a change in neuroanatomy. This study argues for a dominant role of inflammatory markers in the generation of pruritus in psoriasis supported by positive correlations between PASI and pruritus intensity (placebo group, RW phase). Changes in neuroanatomy seem to be secondary due to scratching or cutaneous inflammation. Thus, the function of cutaneous nerves under psoriatic condition might be more crucial for pruritus than the anatomy. Neuroimmune communication, a close interaction between nerve fibres and immune cells via their released factors such as inflammatory chemokines (e.g., chemokine [C-X-C motif] ligand 1; CXCL1), cytokines (e.g., tumour necrosis factor α, IL31, IL17A) or neuropeptides (e.g., CGRP, SP) and their respective receptors may contribute to the progression of psoriatic lesions and pruritus (37). Pro-inflammatory cytokines such as IL31 were already shown to influence neuronal function and outgrowth in other inflammatory skin diseases like atopic dermatitis (38). There are also indications that IL17A may act directly on nerves by influencing both growth and excitability (22), but also secondarily through activation of, e.g., CXCL1, which in turn facilitates pruritus (39).
We hypothesize that cutaneous neuroanatomy change is delayed to its epidermal environment, as we revealed a negative correlation of PASI scores in lesional skin at baseline and IENFD after the OL SEC treatment. This result indicates that patients with lower PASI scores at baseline showed a more profound regeneration of IENFD with SEC treatment. Therefore, it can be speculated that inflammation has a long-term effect on cutaneous neuroanatomy. Persistent, excessive inflammation can impair neuronal regeneration (40), so the extent of inflammation could impair or determine the course of neuroanatomical recovery even under psoriatic conditions.
Taken together, we demonstrated the potency of SEC treatment regarding improvement of pruritus and reversal of histopathological abnormalities. We showed for the first time a beneficial impact of SEC on altered neuroanatomy in psoriatic skin, which remained stable even after discontinuation of the drug, while pruritus began to worsen along with recurrence of the disease. Exact molecular relationships between IL17A inhibition, pruritus, and epidermal neuroanatomy under psoriatic inflammation should be further elucidated in future investigations.
ACKNOWLEDGEMENTS
IRB approval status: IRB approval was obtained from the Ethics Commission Westfalian Lippe Münster (No. 2014-S61-f-A). The independent ethics committee or institutional review board at each study site approved the study protocol, informed consent forms, and recruitment materials before patient enrolment. The studies were conducted in accordance with the International Conference for Harmonisation guidelines, applicable regulations, and the Declaration of Helsinki. Written informed consent was obtained from all participants.
REFERENCES
- Amatya B, Wennersten G, Nordlind K. Patients’ perspective of pruritus in chronic plaque psoriasis: a questionnaire-based study. J Eur Acad Dermatol Venereol 2008; 22: 822–826. https://doi.org/10.1111/J.1468-3083.2008.02591.X
- Yosipovitch G, Goon A, Wee J, Chan YH, Goh CL. The prevalence and clinical characteristics of pruritus among patients with extensive psoriasis. Br J Dermatol 2000; 143: 969–973. https://doi.org/10.1046/J.1365-2133.2000.03829.X
- Reich A, Hrehorow E, Szepietowski JC. Pruritus is an important factor negatively influencing the well-being of psoriatic patients. Acta Derm Venereol 2010; 90: 257–263. https://doi.org/10.2340/00015555-0851
- Hawro M, Sahin E, Steć M, Różewicka-Czabańska M, Raducha E, Garanyan L, et al. A comprehensive, tri-national, cross-sectional analysis of characteristics and impact of pruritus in psoriasis. J Eur Acad Dermatol Venereol 2022; 36: 2064–2075. https://doi.org/10.1111/JDV.18330
- Korman NJ, Zhao Y, Pike J, Roberts J, Sullivan E. Increased severity of itching, pain, and scaling in psoriasis patients is associated with increased disease severity, reduced quality of life, and reduced work productivity. Dermatol Online J 2015; 21. https://doi.org/10.5070/d32110028943
- Zhu B, Edson-Heredia E, Guo J, Maeda-Chubachi T, Shen W, Kimball AB. Itching is a significant problem and a mediator between disease severity and quality of life for patients with psoriasis: results from a randomized controlled trial. Br J Dermatol 2014; 171: 1215–1219. https://doi.org/10.1111/bjd.13065
- Ständer S, Steinke S, Augustin M, Metze D, Loser K, Baeumer D, et al. Quality of life in psoriasis vulgaris: use of the ItchyQoL questionnaire in a secukinumab phase iii trial in patients with psoriasis vulgaris. Acta Derm Venereol 2019; 99: 1085–1090. https://doi.org/10.2340/00015555-3275
- Agelopoulos K, Pereira MP, Wiegmann H, Ständer S. Cutaneous neuroimmune crosstalk in pruritus. Trends Mol Med 2022; 28: 452–462. https://doi.org/10.1016/J.MOLMED.2022.03.005
- Komiya E, Tominaga M, Kamata Y, Suga Y, Takamori K. Molecular and cellular mechanisms of itch in psoriasis. Int J Mol Sci 2020; 21: 1–25. https://doi.org/10.3390/IJMS21218406
- Ayasse MT, Buddenkotte J, Alam M, Steinhoff M. Role of neuroimmune circuits and pruritus in psoriasis. Exp Dermatol 2020; 29: 414–426. https://doi.org/10.1111/EXD.14071
- Nattkemper LA, Lipman ZM, Ingrasci G, Maldonado C, Garces JC, Loayza E, et al. Neuroimmune mediators of pruritus in Hispanic scalp psoriatic itch. Acta Derm Venereol 2023; 103: adv4463. https://doi.org/10.2340/actadv.v103.4463
- Kodji X, Arkless KL, Kee Z, Cleary SJ, Aubdool AA, Evans E, et al. Sensory nerves mediate spontaneous behaviors in addition to inflammation in a murine model of psoriasis. FASEB J 2019; 33: 1578–1594. https://doi.org/10.1096/FJ.201800395RR
- Johansson O, Han SW, Enhamre A. Altered cutaneous innervation in psoriatic skin as revealed by PGP 9.5 immunohistochemistry. Arch Dermatol Res 1991; 283: 519–523. https://doi.org/10.1007/BF00371926
- Tan Y, Ng WJ, Lee SZX, Lee BTK, Nattkemper LA, Yosipovitch G, et al. 3-dimensional optical clearing and imaging of pruritic atopic dermatitis and psoriasis skin reveals downregulation of epidermal innervation. J Invest Dermatol 2019; 139: 1201–1204. https://doi.org/10.1016/j.jid.2018.11.006
- Taneda K, Tominaga M, Negi O, Tengara S, Kamo A, Ogawa H, et al. Evaluation of epidermal nerve density and opioid receptor levels in psoriatic itch. Br J Dermatol 2011; 165: 277–284. https://doi.org/10.1111/J.1365-2133.2011.10347.X
- Nattkemper LA, Tey HL, Valdes-Rodriguez R, Lee H, Mollanazar NK, Albornoz C, et al. The genetics of chronic itch: gene expression in the skin of patients with atopic dermatitis and psoriasis with severe itch. J Invest Dermatol 2018; 138: 1311–1317. https://doi.org/10.1016/J.JID.2017.12.029
- Pogatzki-Zahn EM, Pereira MP, Cremer A, Zeidler C, Dreyer T, Riepe C, et al. Peripheral sensitization and loss of descending inhibition is a hallmark of chronic pruritus. J Invest Dermatol 2020; 140: 203–211.e4. https://doi.org/10.1016/J.JID.2019.05.029
- Renkhold L, Wiegmann H, Pfleiderer B, Süer A, Zeidler C, Pereira MP, et al. Scratching increases epidermal neuronal branching and alters psychophysical testing responses in atopic dermatitis and brachioradial pruritus. Front Mol Neurosci 2023; 16: 1260345. https://doi.org/10.3389/fnmol.2023.1260345
- Feldman SR, Green L, Kimball AB, Siu K, Zhao Y, Herrera V, et al. Secukinumab improves scalp pain, itching, scaling and quality of life in patients with moderate-to-severe scalp psoriasis. J Dermatolog Treat 2017; 28: 716–721. https://doi.org/10.1080/09546634.2017.1329502
- Lacour JP, Paul C, Jazayeri S, Papanastasiou P, Xu C, Nyirady J, et al. Secukinumab administration by autoinjector maintains reduction of plaque psoriasis severity over 52 weeks: results of the randomized controlled JUNCTURE trial. J Eur Acad Dermatol Venereol 2017; 31: 847–856. https://doi.org/10.1111/JDV.14073
- Lowes MA, Kikuchi T, Fuentes-Duculan J, Cardinale I, Zaba LC, Haider AS, et al. Psoriasis vulgaris lesions contain discrete populations of Th1 and Th17 T cells. J Invest Dermatol 2008; 128: 1207–1211. https://doi.org/10.1038/sj.jid.5701213
- Moynes DM, Vanner SJ, Lomax AE. Participation of interleukin 17A in neuroimmune interactions. Brain Behav Immun 2014; 41: 1–9. https://doi.org/10.1016/j.bbi.2014.03.004
- Bobko S, Zeidler C, Osada N, Riepe C, Pfleiderer B, Pogatzki-Zahn E, et al. Intraepidermal nerve fibre density is decreased in lesional and inter-lesional prurigo nodularis and reconstitutes on healing of lesions. Acta Derm Venereol 2016; 96: 404–406. https://doi.org/10.2340/00015555-2232
- Sage D, Donati L, Soulez F, Fortun D, Schmit G, Seitz A, et al. DeconvolutionLab2: an open-source software for deconvolution microscopy. Methods 2017; 115: 28–41. https://doi.org/10.1016/J.YMETH.2016.12.015
- Markram H. The blue brain project. Nat Rev Neurosci 2006; 7: 153–160. https://doi.org/10.1038/NRN1848
- Langley RG, Elewski BE, Lebwohl M, Reich K, Griffiths CEM, Papp K, et al. Secukinumab in plaque psoriasis: results of two phase 3 trials. N Engl J Med 2014; 371: 326–338. https://doi.org/10.1056/NEJMOA1314258
- Frieder J, Kivelevitch D, Menter A. Secukinumab: a review of the anti-IL-17A biologic for the treatment of psoriasis. Ther Adv Chronic Dis 2018; 9: 5–21. https://doi.org/10.1177/2040622317738910
- Simopoulou T, Tsiogkas SG, Zafiriou E, Bogdanos DP. Secukinumab, ixekizumab, bimekizumab and brodalumab for psoriasis and psoriatic arthritis. Drugs Today (Barc) 2023; 59: 135–167. https://doi.org/10.1358/dot.2023.59.3.3419557
- Lessard JC, Piña-Paz S, Rotty JD, Hickerson RP, Kaspar RL, Balmain A, et al. Keratin 16 regulates innate immunity in response to epidermal barrier breach. Proc Natl Acad Sci U S A 2013; 110: 19537–19542. https://doi.org/10.1073/PNAS.1309576110
- Granata M, Skarmoutsou E, Mazzarino MC, D’Amico F. S100A7 in psoriasis: immunodetection and activation by CRISPR technology. Methods Mol Biol 2019; 1929: 729–738. https://doi.org/10.1007/978-1-4939-9030-6_45
- Werner B, Bresch M, Brenner FM, Lima HC. Comparative study of histopathological and immunohistochemical findings in skin biopsies from patients with psoriasis before and after treatment with acitretin. J Cutan Pathol 2008; 35: 302–310. https://doi.org/10.1111/J.1600-0560.2007.00800.X
- Fernandes AR, Martins-Gomes C, Santini A, Silva AM, Souto EB. Psoriasis vulgaris: pathophysiology of the disease and its classical treatment versus new drug delivery systems. In: Grumezescu AM, editor. Design of nanostructures for versatile therapeutic applications. Norwich, NY: William Andrew Publishing; 2018: p. 379–406. https://doi.org/10.1016/B978-0-12-813667-6.00009-7
- Blauvelt A, Pariser DM, Tyring S, Bagel J, Alexis AF, Soung J, et al. Psoriasis improvements and inflammatory biomarker normalization with secukinumab: the randomized ObePso-S study. J Dermatol Sci 2023; 109: 12–21. https://doi.org/10.1016/J.JDERMSCI.2023.01.003
- Gauglitz GG, Bureik D, Zwicker S, Ruzicka T, Wolf R. The antimicrobial peptides psoriasin (S100A7) and koebnerisin (S100A15) suppress extracellular matrix production and proliferation of human fibroblasts. Skin Pharmacol Physiol 2015; 28: 115–123. https://doi.org/10.1159/000363579
- Kim TW, Shim WH, Kim JM, Mun JH, Song M, Kim HS, et al. Clinical characteristics of pruritus in patients with scalp psoriasis and their relation with intraepidermal nerve fiber density. Ann Dermatol 2014; 26: 727–732. https://doi.org/10.5021/ad.2014.26.6.727
- Cui S, Xiao T, Wang Y, Lu H, Wang Y, Gao XH, et al. Morphological relationship between nerve fibers and Langerhans cells in the epidermis of psoriasis vulgaris and lichen simplex chronicus. J Dermatol Sci 2009; 56: 132–134. https://doi.org/10.1016/J.JDERMSCI.2009.07.009
- Choi JE, Di Nardo A. Skin neurogenic inflammation. Semin Immunopathol 2018; 40: 249–259. https://doi.org/10.1007/s00281-018-0675-z
- Nemmer JM, Kuchner M, Datsi A, Oláh P, Julia V, Raap U, et al. Interleukin-31 signaling bridges the gap between immune cells, the nervous system and epithelial tissues. Front Med (Lausanne) 2021; 8: 639097. https://doi.org/10.3389/fmed.2021.639097
- Oleszycka E, Kwiecien K, Kwiecinska P, Morytko A, Pocalun N, Camacho M, et al. Soluble mediators in the function of the epidermal-immune-neuro unit in the skin. Front Immunol 2022; 13: 1003970. https://doi.org/10.3389/fimmu.2022.1003970
- Gu D, Xia Y, Ding Z, Qian J, Gu X, Bai H, et al. Inflammation in the peripheral nervous system after injury. Biomedicines 2024; 12: 1256. https://doi.org/10.3390/biomedicines12061256