ORIGINAL REPORT
Tildrakizumab Treatment for Psoriasis in Real-world Practice: An Analysis from the Swiss Registry (SDNTT)
Julia-Tatjana MAUL1,2, Melike AK1, Sara E. CERMINARA3, Simona STEINMANN1, Elisabeth V. GOESSINGER3, Anna DARZINA4, Iker OYANGUREN MONFERRER4, Raphael MICHEROLI5, Georgios KOKOLAKIS6, Elisabeth ROIDER3, Felix OESTEREICH7, Eva MATEU8, Martina BURLANDO9, Alexander A. NAVARINI3, Thomas KÜNDIG1,2 and Lara Valeska MAUL1,2
1Department of Dermatology, University Hospital Zurich, Zurich, 2Faculty of Medicine, University of Zürich, Zürich, 3Department of Dermatology, University Hospital Basel, Basel, Switzerland, 4Swiss4ward, Alicante, Spain, 5Department of Rheumatology, University Hospital Zurich, University of Zurich, Zurich, Switzerland, 6Psoriasis Research and Treatment Centre, Department of Dermatology, Venereology and Allergology, Charité-Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Berlin, Germany, 7Almirall AG, Wallisellen, Switzerland, 8TFS HealthScience, Barcelona, Spain, and 9Section of Dermatology, Department of Health Sciences (DISSAL), IRCCS San Martino University Hospital, Genoa, Italy
Real-world data on the effectiveness and safety of tildrakizumab, an interleukin 23p19 inhibitor, in Switzerland is limited. The objectives of this analysis were to assess the effectiveness and safety of tildrakizumab in patients with moderate-to-severe plaque psoriasis in Switzerland. Twenty-eight adults from the Swiss Dermatology Network for Targeted Therapies registry (SDNTT), who were on tildrakizumab treatment and had at least 3 months’ follow-up, were enrolled in this prospective, multicentre study. No missing data imputation was performed. The median Psoriasis Area and Severity Index (PASI) decreased from 9.5 at baseline to 2.1 and 0.3 (both p < 0.001) after 3 and 18 months, respectively, of tildrakizumab treatment. After 3 months, 76.9%/30.8% patients reached an absolute PASI < 3/ < 1. These rates increased to 85.7%/57.1% after 18 months of treatment. The proportions of patients achieving PASI 90/100 responses were 47.8%/30.4% at month 6 and 42.9%/14.3% at month 18. A significant improvement in quality of life up to 18 months of follow-up was observed as measured by the Dermatology Life Quality Index. There were no treatment discontinuations due to adverse events. This real-world registry provides robust evidence supporting the long-term effectiveness and favourable safety profile of tildrakizumab in treating patients with moderate-to-severe psoriasis.
SIGNIFICANCE
Based on data from patients participating in the Swiss Dermatology Network for Targeted Therapies registry, we assessed the long-term effectiveness and safety of tildrakizumab for the treatment of plaque psoriasis in clinical practice in Switzerland, a country with limited data available. After 3 months of treatment, tildrakizumab significantly improved both skin symptoms and quality of life of patients, maintaining these responses until month 18 and without safety concerns. Our study supports the long-term effectiveness and favourable safety profile of tildrakizumab for the treatment of moderate-to-severe plaque psoriasis.
Key words: psoriasis; real-world; registry; tildrakizumab.
Citation: Acta Derm Venereol 2024; 104: adv40946. DOI: https://doi.org/10.2340/actadv.v104.40946.
Copyright: © 2024 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Jun 5, 2024; Accepted after revision: Nov 5, 2024; Published: Nov 27, 2024
Corr: Dr Lara Valeska Maul, Department of Dermatology, University Hospital Zurich, Rämistrasse 100, CH-8091 Zurich, Switzerland. E-mail: lara.maul-duwendag@usz.ch
Competing interests and funding: J-TM has served as adviser and/or received speaking fees and/or participated in clinical trials sponsored by AbbVie, Almirall, Amgen, Bristol-Myers Squibb, Celgene, Eli Lilly, Incyte, Janssen, Leo Pharma, Merck Sharp & Dohme, Novartis, Pfizer, Pierre Fabre, Roche, Sanofi, and UCB. MA has no conflict of interest. SEC has no conflict of interest. SS has no conflict of interest. EG has no conflict of interest. AD has no conflict of interest. IOM has no conflict of interest. RM has no conflict of interest. GK has received travel grants or honoraria or has been a consultant member of advisory boards and speakers’ bureaux for one or more of the following: AbbVie, Actelion Pharmaceuticals, Almirall, Amgen, Basilea Pharmaceutica, Bayer Schering Pharma, Biogen Idec, Boehringer-Ingelheim, Celgene, Bristol-Myers Squibb, Hexal-Sandoz, Janssen-Cilag, Leo Pharma, Lilly, MSD Sharp & Dohme, Novartis, Pfizer, Sanofi, Takeda, and UCB. ER is a shareholder and founder of Maximon AG and its holding ventures, receives funding from the Goldschmidt Jacobson Foundation and the Swiss National Science Foundation and has received consultant and/or speaking fees from Eli Lilly, Galderma and Incyte. FO is an employee of Almirall. EM is an employee of TFS HealthScience. MB has acted as a speaker and consultant for AbbVie, Amgen, Eli Lilly, Janssen, Novartis, and UCB Pharma. AAN declares being a consultant and adviser and/or receiving speaking fees and/or grants and/or served as an investigator in clinical trials for AbbVie, Almirall, Amgen, Biomed, BMS, Boehringer Ingelheim, Celgene, Eli Lilly, Galderma, GSK, Leo Pharma, Janssen-Cilag, MSD, Novartis, Pfizer, Pierre Fabre Pharma, Regeneron, Sandoz, Sanofi, and UCB. TK has intermittent, project-focused consulting and/or advisory relationships with Leo Pharma, Janssen-Cilag, Eli Lilly, Pierre Fabre, Sanofi Genzyme, AbbVie, Biomed AG, Novartis, Almirall, Bristol-Myers Squibb, Galderma, L’Oréal/LaRoche-Posay, Merck-Sharp & Dohme, Zur Rose AG, Allergy Therapeutics AG, Derma2go AG, Oncobit AG, EVAX AG, Saiba Biotechnology AG, Saiba Animal Health AG, AltiBio Corp, Encoded Corp, Mabylon AG, MannKind Corp, and XBiotech Corp. LVM has served as adviser and/or received speaking fees and/or participated in clinical trials sponsored by Almirall, Amgen, Bristol-Myers Squibb, Eli Lilly, Incyte, MSD, Novartis, Pierre Fabre, Roche, and Sanofi.
The SDNTT registry is supported by AbbVie, Almirall, Bristol Myers Squibb, Janssen, Lilly, and UCB. This publication was funded by Almirall AG, Wallisellen, Switzerland.
INTRODUCTION
Psoriasis is a common chronic inflammatory skin disease associated with multiple comorbidities, such as psoriatic arthritis, cardiometabolic diseases, or depression, with a significant impact on patients’ quality of life (QoL) (1). In recent years, the interleukin (IL)-23/Th17 cell pathway has been identified as a therapeutic target in immune-driven diseases (2). For this reason, current therapeutic strategies that disrupt IL-23 or IL-17 cytokine signalling have become the gold standard in the treatment of moderate-to-severe psoriasis (3).
Interleukin-23 is a heterodimeric cytokine composed of 2 subunits: a p40 subunit shared with IL-12 and a unique p19 subunit. The most recent biologic agents targeting the p19 subunit of the IL-23 cytokine (guselkumab, risankizumab, and tildrakizumab) have demonstrated high levels of efficacy and favourable safety profiles for the treatment of moderate-to-severe psoriasis (4–7). Tildrakizumab is a humanized, immunoglobin G1κ monoclonal antibody that specifically binds to the IL-23 p19 subunit. The randomized, double-blind, placebo-controlled reSURFACE 1 and reSURFACE 2 trials demonstrated the long-term efficacy and safety of tildrakizumab for the treatment of adults with moderate-to-severe plaque psoriasis for up to 5 years (8–10).
Real-life studies have confirmed that tildrakizumab is an effective treatment for moderate-to-severe psoriasis, with a reassuring safety profile over 100 weeks (11–13). However, real-world data on the effectiveness and safety of tildrakizumab are limited and no data from Switzerland are available. So far, only real-world results on the use of tildrakizumab in Switzerland combined with data from an Italian cohort have been published (14). This study aims to examine the long-term effectiveness and safety of tildrakizumab for the treatment of plaque psoriasis in clinical practice in Switzerland, based on data from the Swiss Dermatology Network for Targeted Therapies (SDNTT) registry.
MATERIALS AND METHODS
Patient selection
Male or female subjects aged ≥ 18 years with plaque psoriasis participating in the SDNTT registry (ClinicalTrials.gov Identifier: NCT01706692) (15–21) from 2 sites in Switzerland (University Hospital Basel and University Hospital Zürich) who initiated treatment with tildrakizumab as approved for plaque-type psoriasis at registry entry as first-line or subsequent therapy or during treatment in the registry and who had at least 3 months’ follow-up were included. Written informed consent was obtained from all patients prior to inclusion in the registry and ethical approval was provided by all participating hospitals.
Data collection
The SDNTT registry collects data on the effectiveness, the quality of life, treatment satisfaction, comorbidities, and the safety of modern psoriasis therapies under everyday conditions from 8 study sites in Switzerland. Adult patients starting conventional systemic or biologic treatment are observed for up to 20 years after enrolment and regardless of subsequent therapy. Study data are collected at baseline, at 3 months, at 6 months, and thereafter at 6-month intervals, using case report forms for both patients and physicians.
This analysis includes the patients’ baseline demographic data (sex, age, age at psoriasis diagnosis, bodyweight, body mass index, presence of comorbidities), the treatment effectiveness, which was assessed using the Psoriasis Area and Severity Index (PASI) response rates, Body Surface Area (BSA) affected, and static Physician Global Assessment (sPGA). Furthermore, the effect on quality of life (QoL) was measured using the Dermatology Life Quality Index (DLQI), and all reported adverse events (AEs) were analysed to evaluate the safety (22).
Outcomes
The effectiveness analysis included (a) the proportion of patients reaching absolute PASI scores < 5, < 3, and < 1, (b) relative PASI 75, 90, and 100 response rates (i.e., patients achieving ≥ 75%, ≥ 90%, and 100% improvement from baseline PASI) at each visit, and (c) the evolution of PASI, BSA, and sPGA outcomes. Analogously, the QoL was assessed by analysing absolute DLQI scores and proportions of patients with a DLQI ≤ 5, ≤ 3, and 0/1 at respective study visits. The safety profile was based on the analysis of collected adverse events (AEs).
Statistical analysis
All baseline characteristics, as well as AEs, were analysed using standard descriptive statistics, including absolute and relative frequencies for categorical variables, and mean, standard deviation, median, minimum, and maximum for continuous variables based on observed cases.
For all effectiveness outcomes, the non-parametric Wilcoxon rank-sum test with continuity correction, considering the non-normality of the data confirmed by the Lilliefors test (Kolmogorov–Smirnov), was used to test for statistically significant changes in PASI, BSA, sPGA, or DLQI scores between follow-up and baseline visits. P-values of < 0.05 were deemed statistically significant.
No imputation of missing data was performed. Recorded comorbidities and AEs were classified according to system organ classes and preferred terms from the Medical Dictionary for Regulatory Activities.
RESULTS
Demographics and disease characteristics at baseline
As per the cut-off date (1 July 2023), a total of 28 patients had started treatment with tildrakizumab either at the University Hospital Basel or University Hospital Zürich and have been included in this analysis. Table I presents the baseline data of the patients included in the present analysis. Hypertension was found to be one of the most frequent comorbidities (17.9%), while 25% of patients were smokers (Table I).
| Factor | n | n (%) | Mean (SD) | Median (min–max) |
| Gender* (male) | 28 | 14 (50.0) | ||
| Age (years) | 28 | 47.4 (15.4) | 46.5 (18.5-81.5) | |
| Age at diagnosis (years) | 20 | 30.1 (13.9) | 27.5 (8.0-56.0) | |
| Weight (kg) | 28 | 75.0 (12.0) | 75.0 (55.0-100.0) | |
| BMI (kg/m2) | 28 | 25.9 (4.5) | 25.1 (20.2-38.1) | |
| < 25 | 28 | 14 (50.0) | ||
| 25–29 | 28 | 4 (14.3) | ||
| ≥ 30 | 28 | 10 (35.7) | ||
| PASI score | 27 | 9.3 (5.8) | 9.5 (0.0-29.4) | |
| BSA affected (%) | 27 | 13.1 (9.7) | 10.5 (0.0-40.0) | |
| sPGA | 28 | 2.1 (1.0) | 2.0 (0.0-4.0) | |
| DLQI | 23 | 11.7 (7.4) | 13.0 (0.0-27.0) | |
| Comorbidities** (yes) | 28 | 20 (71.4) | ||
| Social circumstances | ||||
| Tobacco user | 28 | 7 (25.0) | ||
| Ex-tobacco user | 28 | 5 (17.9) | ||
| Hepatobiliary disorders | ||||
| Hepatitis | 28 | 4 (14.3) | ||
| Hepatic steatosis | 28 | 3 (10.7) | ||
| Hepatic cirrhosis | 28 | 2 (7.1) | ||
| Hepatomegaly | 28 | 1 (3.6) | ||
| Vascular disorders | ||||
| Hypertension | 28 | 5 (17.9) | ||
| Peripheral arterial occlusive disease | 28 | 3 (10.7) | ||
| Peripheral venous disease | 28 | 1 (3.6) | ||
| Musculoskeletal and connective tissue disorders | ||||
| Osteoarthritis | 28 | 2 (7.1) | ||
| Metatarsalgia | 28 | 1 (3.6) | ||
| Periarthritis | 28 | 1 (3.6) | ||
| Psoriatic arthropathy | 28 | 1 (3.6) | ||
| Spondylitis | 28 | 1 (3.6) | ||
| Metabolism and nutrition disorders | ||||
| Type 2 diabetes mellitus | 28 | 2 (7.1) | ||
| Hyperuricaemia | 28 | 1 (3.6) | ||
| Iron deficiency | 28 | 1 (3.6) | ||
| Vitamin D deficiency | 28 | 1 (3.6) | ||
| Psychiatric disorders | ||||
| Alcohol abuse | 28 | 2 (7.1) | ||
| Depression | 28 | 2 (7.1) | ||
| Adjustment disorder | 28 | 1 (3.6) | ||
| Respiratory, thoracic, and mediastinal disorders | ||||
| Rhinitis allergic | 28 | 3 (10.7) | ||
| Asthma | 28 | 1 (3.6) | ||
| Sleep apnoea syndrome | 28 | 1 (3.6) | ||
| Nervous system disorders | ||||
| Drug withdrawal convulsions | 28 | 1 (3.6) | ||
| Migraine | 28 | 1 (3.6) | ||
| Parkinson’s disease | 28 | 1 (3.6) | ||
| Polyneuropathy | 28 | 1 (3.6) | ||
| Blood and lymphatic system disorders | ||||
| Bicytopenia | 28 | 1 (3.6) | ||
| Hypersplenism | 28 | 1 (3.6) | ||
| Thrombocytopenia | 28 | 1 (3.6) | ||
| Cardiac disorders | ||||
| Cardiac failure | 28 | 1 (3.6) | ||
| Cardiomyopathy | 28 | 1 (3.6) | ||
| Coronary artery disease | 28 | 1 (3.6) | ||
| Neoplasms benign, malignant, and unspecified (including cysts and polyps) | ||||
| Clear cell renal cell carcinoma | 28 | 1 (3.6) | ||
| Myeloproliferative neoplasm | 28 | 1 (3.6) | ||
| Uterine leiomyoma | 28 | 1 (3.6) | ||
| Skin and subcutaneous tissue disorders | ||||
| Dermatitis atopic | 28 | 1 (3.6) | ||
| Granuloma annulare | 28 | 1 (3.6) | ||
| Congenital, familial, and genetic disorders | ||||
| Factor V Leiden mutation | 28 | 1 (3.6) | ||
| Endocrine disorders | ||||
| Hypothyroidism | 28 | 1 (3.6) | ||
| Eye disorders | ||||
| Neovascular age-related macular degeneration | 28 | 1 (3.6) | ||
| Gastrointestinal disorders | ||||
| Dysphagia | 28 | 1 (3.6) | ||
| General disorders and administration site conditions | ||||
| Pain | 28 | 1 (3.6) | ||
| Reproductive system and breast disorders | ||||
| Uterine polyp | 28 | 1 (3.6) | ||
| Surgical and medical procedures | ||||
| Hysterectomy | 28 | 1 (3.6) | ||
| *Age at the start of tildrakizumab treatment; **by system organ class and preferred term. Patients may have more than one comorbidity. | ||||
| BMI: body mass index; BSA: body surface area; max: maximum; min: minimum; DLQI: Dermatology Life Quality Index; PASI: Psoriasis Area and Severity Index; SD: standard deviation; sPGA: static Physician Global Assessment. | ||||
Effectiveness
At baseline, a median absolute PASI score of 9.5 was reported. Upon treatment initiation with tildrakizumab, this decreased significantly to 2.1 at month three, 0.9 at month 12, and 0.6 at month 18 (p < 0.001, for all time points) (Fig. 1A). Correspondingly, the number of patients achieving absolute and relative PASI improvements increased. Overall, 92.3%, 76.9%, and 30.8% of patients achieved PASI < 5, PASI < 3, and PASI < 1 at month 3. This increased to 94.7%, 94.7%, and 57.9% at month 12, and 92.9%, 85.7%, and 57.1%, at month 18, respectively (Fig. 1B). At month 6, 69.6% of patients achieved PASI 75, 47.8% a PASI 90, and 30.4% a PASI 100. At month 12, the rates were 79.0%, 47.4% and 10.5%, and after 18 months of tildrakizumab treatment, 71.4%, 43.0%, and 14.3% achieved PASI 75, PASI 90, and PASI 100, respectively (Fig. 1C).
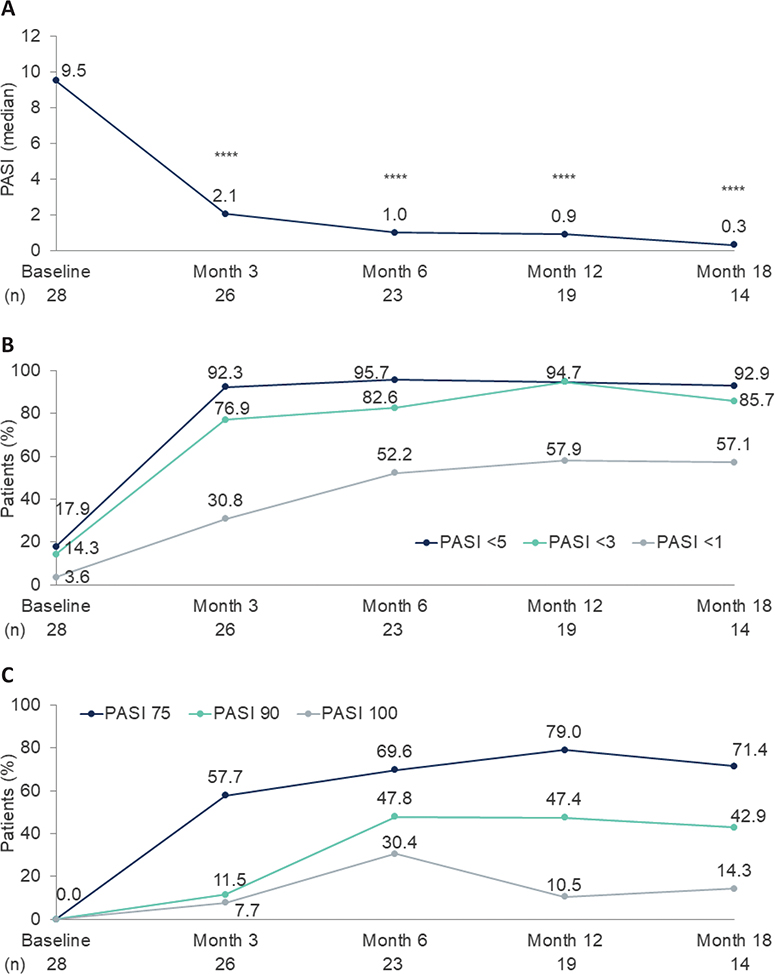
Fig. 1. (A) Absolute Psoriasis Area and Severity Index (PASI), (B) PASI < 5, < 3 and < 1 responses, and (C) PASI 75, 90, and 100 responses over time. ****p < 0.0001; Wilcoxon signed-rank test comparing baseline to follow-up.
In line with the PASI improvements, both the BSA and sPGA scores demonstrated significant improvements. The median affected BSA of patients at baseline was 10.5%. A significant reduction to 1.5% at month 3, 0.6% at month 12, and 0.5% at month 18 (p < 0.0001, in all 3 cases) was observed (Fig. 2A). Lastly, the median sPGA at baseline was 2.0. This median decreased significantly to 1.0 at month 3 (p < 0.0001), a reduction that was maintained until month 18 (Fig. 2B).
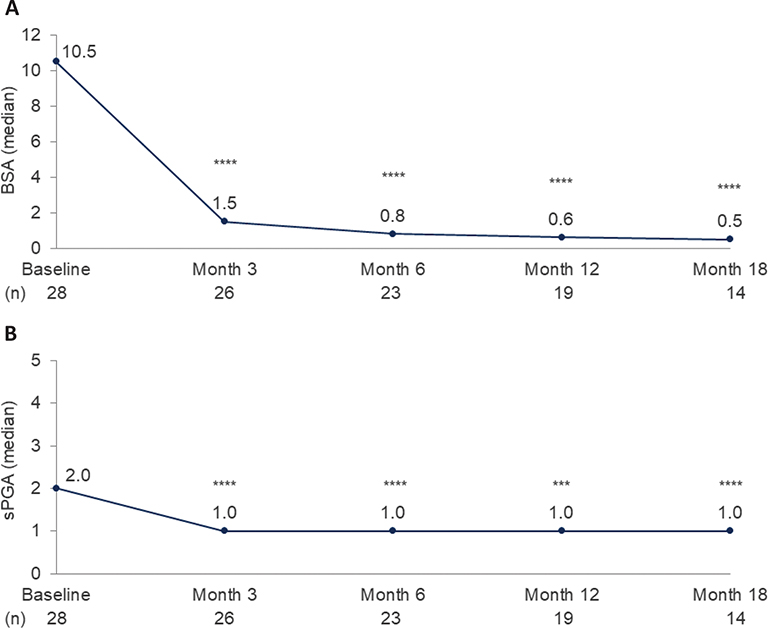
Fig. 2. (A) Body surface area (BSA) and (B) static Physician Global Assessment (sPGA) scores over time. ***p < 0.001, ****p < 0.0001; Wilcoxon signed-rank test.
Quality of life
The quality of life of patients was assessed using the DLQI. At baseline patients reported a median DLQI of 13.0. Upon treatment initiation, the DLQI significantly decreased at each timepoint and a median DLQI of 1.0 was reported at month 6 (p < 0.0001), 0.0 at month 12 (p < 0.001), and 0.5 at month 18 (p < 0.0001), respectively (Fig. 3A). Similarly, the number of patients achieving absolute DLQI values of ≤ 5, ≤ 3, and 0/1 increased over time. At month 6, 60.9%, 56.5%, and 26.1% of patients had a DLQI ≤ 5, ≤ 3, and 0/1, respectively. The DLQI 0/1 response increased to 36.8% of patients at month 12, which was maintained until month 18, where 71.4% achieved a DLQI ≤ 3 and 35.7% a DLQI 0/1 (Fig. 3B).
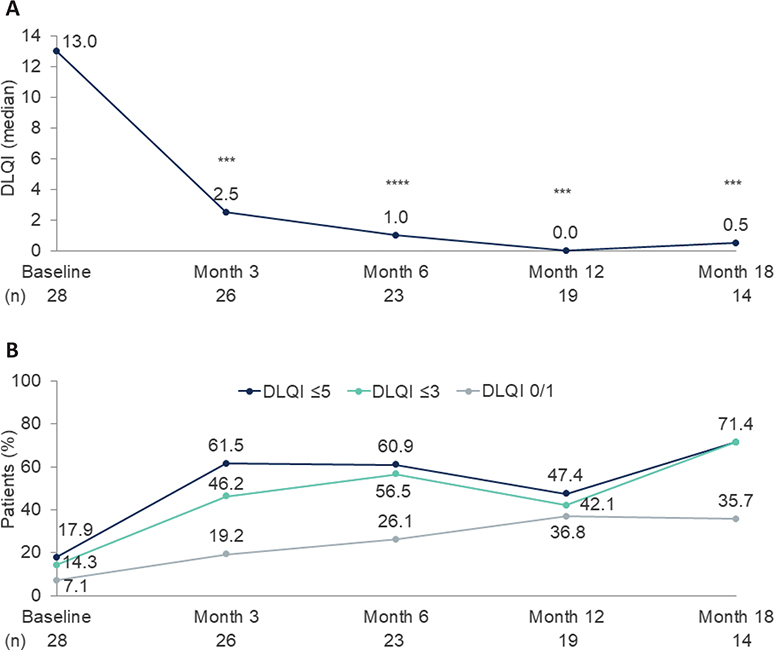
Fig. 3. (A) Dermatology Life Quality Index (DLQI) score and (B) proportions of patients with DLQI ≤ 5, ≤ 3, and 0/1 over time. ***p < 0.001, ****p < 0.0001; Wilcoxon signed-rank test.
Safety
The safety analysis included a follow-up time of 34.5 patient-years with a total of 17 AEs reported. No AEs led to treatment discontinuation. One serious AE (acute biventricular heart failure) was recorded that was assessed as not related to the treatment. Adverse events by system organ class and preferred term are listed in Table II. The most frequent AE was hypertension (n = 2). Three patients reported gastrointestinal disorders and 3 reported nervous system disorders. Two patients reported infections (1 case of folliculitis and 1 case of an upper respiratory tract infection). One patient had a cardiac disorder (1 case of acute cardiac failure).
DISCUSSION
The present study is based on real-world data collected in the SDNTT registry at 2 hospital centres in Switzerland to assess the effectiveness, safety, and impact on QoL of tildrakizumab in the management of psoriasis. In line with previous results from Switzerland, this analysis showed high PASI response rates and a fast and lasting QoL improvement with tildrakizumab in a real-world setting (14).
Compared with the reSURFACE 1 and reSURFACE 2 clinical trials (8, 23), our cohort had lower baseline PASI, BSA, and sPGA scores, which was due to the stricter inclusion/exclusion criteria of the phase 3 trials as well as switches from other therapies (24), and a lower bodyweight that could be explained by the inclusion of a higher percentage of women in the current study. In addition, in the real-world setting, conventional systemic therapies are required prior to initiation of biologics and washout periods are uncommon, further facilitating lower absolute PASI values at baseline. Psoriasis is associated with an increased risk of several comorbidities, also known as the comorbidome, that may influence its progression and vice versa (25, 26). Examples of relevant comorbidities linked to psoriasis include cardiovascular, metabolic, or mental health diseases, as well as psoriatic arthritis (25, 26), which were well represented in our cohort (with 18% of patients reporting hypertension, 7% diabetes, 7% depression, and 3.6% psoriatic arthritis) and with frequencies in agreement with that of previous real-world studies (27, 28). Surprisingly, but in line with the lower bodyweight, hypertension was less frequent in this cohort than in the phase 3 reSURFACE trials (about 30%) (8).
In recent years, therapies have become more effective and, consequently, more ambitious treatment goals can be achieved and are being pursued. In addition, the focus has shifted from relative endpoints to an absolute outcome (e.g., PASI < 3) (4, 5, 29–32). Overall, our study showed a significant improvement in PASI, BSA, and sPGA outcomes after 3 months of treatment with tildrakizumab, with approximately 80% of patients reaching an absolute PASI < 3. This response increased through 1 year of follow-up, with 95% of patients achieving a PASI < 3 at month 12, a higher percentage than observed in the pooled analyses of reSURFACE trials (82.0% and 85.3% among patients responding to tildrakizumab 100 and 200 mg, defined as PASI 75 response at week 28, respectively) (9). Similar effects (i.e., increased effectiveness compared with the efficacy observed in pivotal trials) have been reported not only in other real-world studies of tildrakizumab (24, 27) but also in real-world studies of guselkumab and risankizumab (33, 34). Al-though IL-23 inhibitors bind the IL-23 p19 subunit, each of them binds an epitope with a unique size, which may influence short- and long-term clinical efficacy in vitro (35). This is why real-world psoriasis data that account for patient complexity are so important.
Recent advances in biologic therapies for moderate-to-severe plaque psoriasis have facilitated the achievement of more ambitious endpoints such as PASI 90 or PASI 100 responses or absolute PASI scores of < 3 or < 1 in most patients. When comparing the relative PASI results obtained in this study with the phase 3 trials (baseline PASI of 9 vs 20, respectively), the observed PASI 90 and PASI 100 response rates at month 12 (47.4%/10.5%) were lower than those observed in the reSURFACE 1 and 2 trials (73.2%/34.4% and 75.6%/45.2% among patients responding to tildrakizumab 100 and 200 mg, respectively) (9). However, the absolute PASI response rates (i.e., PASI < 3 and PASI < 1) were higher compared with the reSURFACE trials. One contributing factor to this effect is certainly the relatively low baseline PASI observed in this cohort, highlighting the relevance of absolute PASI reporting for real-world effectiveness results (36).
In line with this, our study observed higher rates of patients obtaining a PASI of < 3 and lower frequencies of PASI 90 responses at 12 months, when comparing PASI outcomes not only with phase 3 trials but also with other real-world investigations (11, 12, 14). These studies encompassed patients with moderate-to-severe plaque psoriasis treated with tildrakizumab in routine clinical settings. For example, the percentage of patients with PASI < 3 and PASI 90 responses at month 12 was 74.6% and 57.7%, respectively, in the non-interventional TILOT study (11). However, the baseline PASI and BSA scores of the patients included in these studies were also higher than those of our cohort. Notably, patients in our study had a baseline PASI < 10 but a baseline DLQI of 13, indicating that, despite effective symptom management in clinical practice, patients’ QoL remained impaired.
There are few data on the long-term effects of tildrakizumab on patients’ health-related QoL (HRQoL) in a real-world setting (11, 14). Although a high level of response for the HRQoL outcome was observed in our cohort, with 40% of patients achieving a DLQI of 0 or 1 at month 12, other real-world studies have found higher response rates. In the non-interventional TILOT study, the percentage of patients with a DLQI 0/1 was 48% at week 52 (11).
To date, most real-world evidence studies report a maximum follow-up period of 12 months (11, 12, 14). Here, we present data on the effectiveness of tildrakizumab over 18 months in a real-world setting. It is noteworthy that 86% of patients in this cohort maintained a PASI < 3 response at month 18. These results are consistent with the 100-week data recently presented in the TILOT study, which showed that 84% of patients achieved an absolute PASI < 3 after 100 weeks (13), further supporting the long-term effectiveness of tildrakizumab.
In terms of safety, few AEs were reported, and no patient discontinued the study drug due to an AE in this cohort. Tildrakizumab may increase the risk of infection. Adverse cardiovascular events and malignancies are also AEs of special interest among IL-23p19 inhibitors (6). At the time of this analysis, only 2 patients had reported infectious AEs and 1 patient had suffered a cardiac disorder. No malignancies were reported.
Limitations
Nonetheless, this study has several limitations. These include the small sample size and selection bias associated with real-world studies. In addition, only the 100 mg prefilled syringe of tildrakizumab was available during the study as the 200 mg prefilled syringe was not yet commercialized in Switzerland (the recommended dose is 100 mg, but a dose of 200 mg may be considered in patients with high disease burden or weighing more than 90 kg) (37).
Conclusion
This analysis of the effectiveness, safety, and impact on QoL of tildrakizumab for the treatment of psoriasis from the SDNTT registry demonstrated that, after 3 months of treatment, tildrakizumab significantly improved patients’ skin symptoms and HRQoL, maintaining these responses until month 18. No new safety findings were recorded throughout the follow-up period. In conclusion, real-world data from the SDNTT registry support the long-term effectiveness and favourable safety profile of tildrakizumab for the treatment of patients with moderate-to-severe plaque psoriasis. Overall, the results from Switzerland are consistent with those of real-world studies supporting the effectiveness and safety of long-term use of IL-23p19 inhibitors.
ACKNOWLEDGEMENTS
The authors would like to thank all the patients who contributed to the registries, without whom this research would not be possible. They particularly acknowledge the substantial contribution of the coordinating team, and the enthusiastic collaboration of all the dermatologists and nurses who provided data.
Data availability statement
Datasets generated during and/or analysed during this study are available from the corresponding author upon reasonable request.
REFERENCES
- Griffiths CEM, Armstrong AW, Gudjonsson JE, Barker JNWN. Psoriasis. Lancet 2021; 397: 1301–1315. https://doi.org/10.1016/S0140-6736(20)32549-6
- Sharma A, Upadhyay DK, Gupta GD, Narang RK, Rai VK. IL-23/Th17 axis: a potential therapeutic target of psoriasis. Curr Drug Res Rev 2022; 14: 24–36. https://doi.org/10.2174/2589977513666210707114520
- Wu M, Dai C, Zeng F. Cellular mechanisms of psoriasis pathogenesis: a systemic review. Clin Cosmet Investig Dermatol 2023; 16: 2503–2515. https://doi.org/10.2147/CCID.S420850
- Nast A, Smith C, Spuls PI, Avila Valle G, Bata-Csörgö Z, Boonen H, et al. EuroGuiDerm guideline on the systemic treatment of psoriasis vulgaris – Part 1: treatment and monitoring recommendations. J Eur Acad Dermatol Venereol 2020; 34: 2461–2498. https://doi.org/10.1111/jdv.16915
- Nast A, Smith C, Spuls PI, Avila Valle G, Bata-Csörgö Z, Boonen H, et al. EuroGuiDerm guideline on the systemic treatment of psoriasis vulgaris – Part 2: specific clinical and comorbid situations. J Eur Acad Dermatol Venereol 2021; 35: 281–317. https://doi.org/10.1111/jdv.16926
- Blauvelt A, Chiricozzi A, Ehst BD, Lebwohl MG. Safety of IL-23 p19 inhibitors for the treatment of patients with moderate-to-severe plaque psoriasis: a narrative review. Adv Ther 2023; 40: 3410–3433. https://doi.org/10.1007/s12325-023-02568-0
- Xu S, Zhang X, Pan M, Shuai Z, Xu S, Pan F. Treatment of plaque psoriasis with IL-23p19 blockers: a systematic review and meta-analysis. Int Immunopharmacol 2019; 75: 105841. https://doi.org/10.1016/j.intimp.2019.105841
- Reich K, Papp KA, Blauvelt A, Tyring SK, Sinclair R, Thaçi D, et al. Tildrakizumab versus placebo or etanercept for chronic plaque psoriasis (reSURFACE 1 and reSURFACE 2): results from two randomised controlled, phase 3 trials. Lancet 2017; 390: 276–288. https://doi.org/10.1016/S0140-6736(17)31279-5
- Thaci D, Piaserico S, Warren RB, Gupta AK, Cantrell W, Draelos Z, et al. Five-year efficacy and safety of tildrakizumab in patients with moderate-to-severe psoriasis who respond at week 28: pooled analyses of two randomized phase III clinical trials (reSURFACE 1 and reSURFACE 2). Br J Dermatol 2021; 185: 323–334. https://doi.org/10.1111/bjd.19866
- Egeberg A, Jullien D, Gaarn Du Jardin K, Thaçi D. Five-year safety of tildrakizumab in patients with moderate-to-severe psoriasis from two phase 3 trials (reSURFACE 1 and reSURFACE 2): number needed to harm for occurrence of adverse events of special interest. J Dermatolog Treat 2023; 34: 2220447. https://doi.org/10.1080/09546634.2023.2220447
- Tsianakas A, Schwichtenberg U, Pierchalla P, Hinz T, Diemert S, Korge B. Real-world effectiveness and safety of tildrakizumab in long-term treatment of plaque psoriasis: results from the non-interventional, prospective, multicentre study TILOT. J Eur Acad Dermatol Venereol 2023; 37: 85–92. https://doi.org/10.1111/jdv.18572
- Ruggiero A, Fabbrocicni G, Cacciapuoti S, Potestio L, Gallo L, Megna M. Tildrakizumab for the treatment of moderate-to-severe psoriasis: results from 52 weeks real-life retrospective study. Clin Cosmet Investig Dermatol 2023; 16: 529–536. https://doi.org/10.2147/CCID.S402183
- Tsianakas A, Kirsch A, Petri M. Sustained efficacy and safety of tildrakizumab over 2 years in patients with moderate to severe plaque psoriasis in routine clinical practice: interim results in week 100 from the non-interventional, prospective, multicenter study TILOT. Presented at the 32 European Academy of Dermatology and Venereology (EADV) Congress, 11–14 October 2023, Berlin, Germany. Abstract 3110.
- Burlando M, Maul JT, Salvi I, Simic D, Cozzani E, Ak M, et al. Psoriasis patients’ characteristics associated with high PASI response to tildrakizumab: an international dual center study. Eur Rev Med Pharmacol Sci 2022; 26: 6772–6776.
- Maul JT, Augustin M, Sorbe C, Conrad C, Anzengruber F, Mrowietz U, et al. Association of sex and systemic therapy treatment outcomes in psoriasis: a two-country, multicentre, prospective, noninterventional registry study. Br J Dermatol 2021; 185: 1160–1168. https://doi.org/10.1111/bjd.20387
- Cazzaniga S, Anzengruber F, Augustin M, Boehncke WH, Borradori L, Conrad C, et al. Linkage between patients’ characteristics and prescribed systemic treatments for psoriasis: a semantic connectivity map analysis of the Swiss Dermatology Network for Targeted Therapies registry. J Eur Acad Dermatol Venereol 2019; 33: 2313–2318. https://doi.org/10.1111/jdv.15983
- Drach M, Papageorgiou K, Maul JT, Djamei V, Yawalkar N, Häusermann P, et al. Effectiveness of methotrexate in moderate to severe psoriasis patients: real-world registry data from the Swiss Dermatology Network for Targeted Therapies (SDNTT). Arch Dermatol Res 2019; 311: 753–760. https://doi.org/10.1007/s00403-019-01945-6
- Anzengruber F, Augustin M, Radtke MA, Thaci D, Yawalkar N, Streit M, et al. Smoking does not alter the therapy response to systemic anti-psoriatic therapies: a two-country, multi-centre, prospective, non-interventional study. Acta Derm Venereol 2019; 99: 871–877. https://doi.org/10.2340/00015555-3221
- Maul JT, Navarini AA, Sommer R, Anzengruber F, Sorbe C, Mrowietz U, et al. Gender and age significantly determine patient needs and treatment goals in psoriasis: a lesson for practice. J Eur Acad Dermatol Venereol 2019; 33: 700–708. https://doi.org/10.1111/jdv.15324
- Jungo P, Maul JT, Djamei V, von Felten S, Kolios AGA, Czernielewsk J, et al. Superiority in quality of life improvement of biologics over conventional systemic drugs in a Swiss Real-Life Psoriasis Registry. Dermatology 2016; 232: 655–663. https://doi.org/10.1159/000455042
- Maul JT, Djamei V, Kolios AGA, Meier B, Czernielewski J, Jungo P, et al. Efficacy and survival of systemic psoriasis treatments: an analysis of the Swiss Registry SDNTT. Dermatology 2016; 232: 640–647. https://doi.org/10.1159/000452740
- Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI): a simple practical measure for routine clinical use. Clin Exp Dermatol 1994; 19: 210–216. https://doi.org/10.1111/j.1365-2230.1994.tb01167.x
- Reich K, Warren RB, Iversen L, Puig L, Pau-Charles I, Igarashi A, et al. Long-term efficacy and safety of tildrakizumab for moderate-to-severe psoriasis: pooled analyses of two randomized phase III clinical trials (reSURFACE 1 and reSURFACE 2) through 148 weeks. Br J Dermatol 2020; 182: 605–617. https://doi.org/10.1111/bjd.18232
- Drerup KA, Seemann C, Gerdes S, Mrowietz U. effective and safe treatment of psoriatic disease with the anti-IL-23p19 biologic tildrakizumab: results of a real-world prospective cohort study in nonselected patients. Dermatology 2022; 238: 615–619. https://doi.org/10.1159/000519924
- Bu J, Ding R, Zhou L, Chen X, Shen E. Epidemiology of psoriasis and comorbid diseases: a narrative review. Front Immunol 2022; 13: 880201. https://doi.org/10.3389/fimmu.2022.880201
- Buja A, Miatton A, Cozzolino C, Brazzale AR, Lo Bue R, Mercuri SR, et al. The prevalent comorbidome at the onset of psoriasis diagnosis. Dermatol Ther (Heidelb) 2023; 13: 2093–2105. https://doi.org/10.1007/s13555-023-00986-0
- Costanzo A, Llamas-Velasco M, Fabbrocini G, Cuccia A, Rivera-Diaz R, Gaarn Du Jardin K, et al. Tildrakizumab improves high burden skin symptoms, impaired sleep and quality of life of moderate-to-severe plaque psoriasis patients in conditions close to clinical practice. J Eur Acad Dermatol Venereol 2023; 37: 2004–2015. https://doi.org/10.1111/jdv.19229
- Becher G, Conner S, Ingram JA, Stephen KE, McInnes AC, Heald AH, et al. A retrospective real-world study of the effectiveness and tolerability of tildrakizumab in UK adults with moderate-to-severe chronic plaque psoriasis. Dermatol Ther (Heidelb) 2022; 12: 2343–2354. https://doi.org/10.1007/s13555-022-00800-3
- Belinchón Romero I, Dauden E, Ferrándiz Foraster C, González-Cantero Á, Carrascosa Carrillo JM. Therapeutic goals and treatment response evaluation in moderate to severe psoriasis: an experts opinion document. Ann Med 2021; 53: 1727–1736. https://doi.org/10.1080/07853890.2021.1986637
- Amatore F, Villani AP, Tauber M, Viguier M, Guillot B, Psoriasis Research Group of the French Society of Dermatology (Groupe de Recherche sur le Psoriasis de la Société Française de Dermatologie). French guidelines on the use of systemic treatments for moderate-to-severe psoriasis in adults. J Eur Acad Dermatol Venereol 2019; 33: 464–483. https://doi.org/10.1111/jdv.15340
- Gisondi P, Talamonti M, Chiricozzi A, Piaserico S, Amerio P, Balato A, et al. Treat-to-target approach for the management of patients with moderate-to-severe plaque psoriasis: consensus recommendations. Dermatol Ther (Heidelb) 2021; 11: 235–252. https://doi.org/10.1007/s13555-020-00475-8
- Treatment Guidelines – International Psoriasis Council [Internet]. 2022 [cited 2023 Dec 12]. Available from: https://psoriasiscouncil.org/education/treatment-guidelines/
- Galluzzo M, Talamonti M, Bernardini N, Chiricozzi A, De Simone C, Bonifati C, et al. Real-world outcomes in patients with moderate-to-severe plaque psoriasis treated with guselkumab for up to 1 year. Expert Opin Biol Ther 2022; 22: 1585–1592. https://doi.org/10.1080/14712598.2022.2090835
- Mastorino L, Susca S, Megna M, Siliquini N, Quaglino P, Ortoncelli M, et al. Risankizumab shows high efficacy and maintenance in improvement of response until week 52. Dermatol Ther 2022; 35: e15378. https://doi.org/10.1111/dth.15378
- Daniele SG, Eldirany SA, Damiani G, Ho M, Bunick CG. Structural basis for p19 targeting by anti-il-23 biologics: correlations with short- and long-term efficacy in psoriasis. JID Innov 2024; 4: 100261. https://doi.org/10.1016/j.xjidi.2024.100261
- Strober B, Ferris L, Callis Duffin K, Janak JC, Sima AP, Eckmann T, et al. Real-world effectiveness of risankizumab in patients with moderate-to-severe psoriasis using the CorEvitas Psoriasis Registry. J Am Acad Dermatol 2024; 90: 82–90. https://doi.org/10.1016/j.jaad.2023.08.097
- Kokolakis G, Kreis G, Falqués M, Aparici M, Sondermann W. High tolerability, favorable safety, and subjects’ preference for a single 200 mg/2 mL tildrakizumab injection: a phase I, open-label, randomized crossover trial in healthy volunteers. Dermatol Ther (Heidelb) 2022; 12: 2135–2144. https://doi.org/10.1007/s13555-022-00789-9