SHORT COMMUNICATION
Somatic Variants of KRT1/KRT10 Identified by Next-generation Sequencing in Patients with Epidermal Nevi
Shuya SUN#, Ran MO#, Zhiming CHEN, Yong YANG and Ruiyu XIANG*
Genetic Skin Disease Center, Jiangsu Key Laboratory of Molecular Biology for Skin Diseases and STIs, Hospital for Skin Diseases, Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College, Nanjing 210042, China.
*E-mail: ryxiang@pumcderm.cams.cn
#These authors contributed equally to this work and shared the first authorship.
Citation: Acta Derm Venereol 2024; 104: adv40958. DOI https://doi.org/10.2340/actadv.v104.40958.
Copyright: © 2024 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Jun 6, 2024; Accepted after revision: Sep 18, 2024; Published: Oct 22, 2024
Competing interests and funding: The authors have no conflicts of interest to declare.
This work was supported by grants from the CAMS Innovation Fund for Medical Sciences (CIFMS) (2021-I2M-1-018).
INTRODUCTION
Epidermal nevus (EN) is a benign hamartomatous skin lesion typically manifesting within the first year of life, characterized by localized verrucous epidermal thickening following Blaschko’s lines (1, 2). EN is considered a result of genetic mosaicism mainly caused by somatic variants in keratin genes (1). However, detecting these variants poses a challenge due to their low frequency in peripheral blood, necessitating the use of more precise methods beyond universal next-generation sequencing (NGS).
Here, we describe 3 patients diagnosed with ENs resulting from low-frequency somatic variants in KRT1 or KRT10, including 2 unreported variants. Written informed consents were obtained. The research was approved by the Ethics Committee of the Institute of Dermatology of the Chinese Academy of Medical Sciences and Peking Union Medical College (2019-Clinic-005).
CASE REPORTS
All the patients exhibited classic clinical manifestations of EN, characterized by asymmetrical hyperkeratotic plaques along Blaschko’s lines. Patient 1, a 4-year-old female, presented with narrow-band lesions extensively distributed on the trunk, buttocks, and flexural aspects of the limbs. Patient 2, a 41-year-old male, exhibited broad-band lesions predominantly on the buttocks, abdomen, and groin, accompanied by widespread erythema, hyper-keratotic patches, and desquamation. Patient 3, a 33-month-old male child (Fig. 1A), displayed lesions in a narrow-band pattern scattered on the trunk and limbs. None of them had a related family history or other associated systemic symptoms.
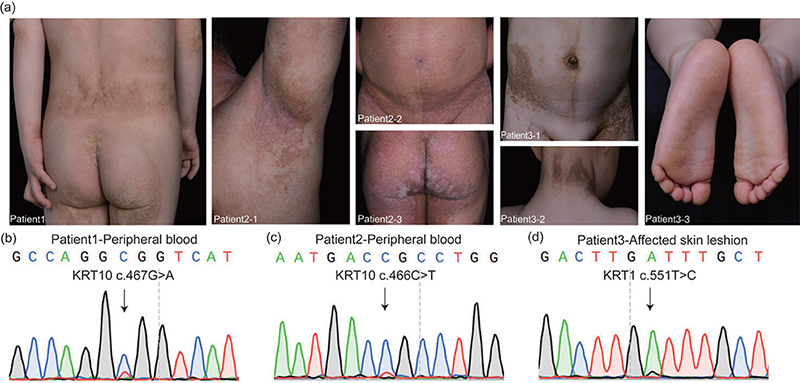
Fig. 1. Patients’ clinical and genetic features. (A) Patient 1: Verrucous hyperkeratotic plaques on the trunk, buttocks, and flexural aspects of the limbs; Patient 2: Hyperkeratotic plaques covering the buttocks, abdomen, and groin, accompanied by widespread erythema, hyperkeratotic patches, and desquamation; Patient 3: Scattered hyperkeratotic plaques along Blaschko’s lines, especially on the trunk and limbs. (B) A KRT10 c.467G>A somatic mosaic variant was detected from Patient 1’s peripheral blood. (C) A KRT10 c.466C>T somatic mosaic variant was detected from Patient 2’s peripheral blood. (D) A KRT1 c.551T>C somatic mosaic variant was detected from Patient 3’s affected skin tissue.
To ascertain the genetic aetiology, we first isolated the patients’ DNA from peripheral blood to perform the Skin NGS panel (MyGenostics, Beijing, China), which is the custom exome sequencing panel containing 723 genodermatosis-targeted genes. Subsequent polymerase chain reaction (PCR)–NGS (10,000×) was accomplished for further verification of the variant ratio.
RESULTS
Patient 1’s result showed a pathogenic mosaic variant of KRT10 c.467G > A (p.A156H) with a variant ratio of 23.6784% (8618/36,396). This is an unreported pathogenic missense variant with allele frequency of 0.000008238 (ExAC database), predicted to be deleterious (SIFT), probably damaging (PolyPhen) and disease-causing (MutationTaster). Patient 2’s result revealed a mosaic variant of KRT10 c.466C > T (p.R156C) with a variant ratio of 13% (1190/9236), which is a reported pathogenic variant of EN and epidermolytic hyperkeratosis (2, 3). However, no genetic variant was discovered in Patient 3’s peripheral blood DNA. Therefore, we obtained a biopsy specimen of his affected skin. A heterozygous KRT1 c.551T > C (p.I184T) variant was detected with a variant ratio of 18% (26,186/142,033) in DNA extracted from his affected skin tissue. This variant was not found in the ExAC database, and was predicted to be deleterious (SIFT), probably damaging (PolyPhen) and disease-causing (MutationTaster). Sanger sequencing confirmed all the genomic variants in the 3 patients (Fig. 1B–D).
ENs are regarded as benign skin mosaicism disorders affecting the epidermis and skin appendages, and can occasionally involve other organ systems, including skeletal, neurological, and ophthalmological systems, which is termed EN syndrome (4, 5). ENs may also appear with malignant tumours of skin or other systems (6). Thus, a complete assessment of affected patients is essential, and more accurate detection techniques are needed for genetic counselling (7). For EN patients with fertility aspirations, sperm genetic testing and pre-implantation genetic testing could be used to reduce the potential genetic risks to their offspring (8).
DISCUSSION
To date, 9 articles have reported cases of EN caused by somatic variants of keratin genes, mainly KRT1, KRT2, and KRT10. Genetic testing methods have gradually improved (1, 2, 9, 10). Initially, genomic DNA from skin lesions was detected through PCR (2). Subsequent advancements, such as whole-exome sequencing, have enabled testing of lower-ratio somatic heterozygous variants in affected skin tissues (9). The application of NGS facilitated discovery of somatic variants from not only the patient’s affected skin but also peripheral blood. Diociaiuti et al. (10) detected a KRT2 c.556A > G somatic variant in a patient with EN through NGS using a customized ichthyosis gene panel through both blood (estimated variant ratio of 1.5%) and affected skin (variant ratio of 25%). On the above basis, we initially combined high-depth skin panel sequencing with high-depth sequencing of pathogenic sites.
We have herein reported 3 cases of EN due to somatic mosaicism variants of KRT1 or KRT10. Two previously unreported variants were found: KRT10 c.467G > A (p.A156H) and KRT1 c.551T > C (p.I184T). Our detection method accurately identified the mosaic proportions in both blood and tissue samples.
In general, mosaicism involving multiple organ systems (both the skin and the blood system are affected) tends to occur in the early stages of embryonic development, while mosaicism confined to a single organ or tissue is the result of somatic variants that occur later in embryonic development (11). To optimize efficiency, we suggest blood sampling for patients with extensive lesions and tissue sampling for those with partial lesions. This approach is crucial for ensuring precise diagnosis, minimizing the risk of misdiagnosis, and should be integrated into clinical practice.
ACKNOWLEDGEMENTS
IRB approval status: The research was approved by the Ethics Committee of the Institute of Dermatology of the Chinese Academy of Medical Sciences and Peking Union Medical College (2019-Clinic-005).
REFERENCES
- Paller AS, Syder AJ, Chan YM, Yu QC, Hutton E, Tadini G, et al. Genetic and clinical mosaicism in a type of epidermal nevus. N Engl J Med 1994; 331: 1408–1415. https://doi.org/10.1056/NEJM199411243312103
- Samuelov L, Sarig O, Gat A, Halachmi S, Shalev S, Sprecher E. Extensive lentigo simplex, linear epidermolytic naevus and epidermolytic naevus comedonicus caused by a somatic mutation in KRT10. Br J Dermatol 2015; 173: 293–296. https://doi.org/10.1111/bjd.13616
- Haruna K, Suga Y, Mizuno Y, Hasegawa T, Kourou K, Matsuba S, et al. R156C mutation of keratin 10 causes mild form of epidermolytic hyperkeratosis. J Dermatol 2007; 34: 545–548. https://doi.org/10.1111/j.1346-8138.2007.00328.x
- Livingstone E, Hillen U, Hafner C, Piel S, Groesser L, Schadendorf D, et al. Segmentally arranged seborrhoeic keratoses with impending atypia and squamous cell carcinoma in an elderly woman. Br J Dermatol 2015; 172: 1642–1625. https://doi.org/10.1111/bjd.13562
- Morren M-A, Fodstad H, Brems H, Bedoni N, Guenova E, Jacot-Guillarmod M, et al. Mosaic RASopathies concept: different skin lesions, same systemic manifestations? J Med Genet 2024; 61: 411–419. https://doi.org/10.1136/jmg-2023-109306
- Hafner C, Toll A, Real FX. HRAS mutation mosaicism causing urothelial cancer and epidermal nevus. N Engl J Med 2011; 365: 1940–1942. https://doi.org/10.1056/NEJMc1109381
- Kono M, Suga Y, Akashi T, Ito Y, Takeichi T, Muro Y, et al. A child with epidermolytic ichthyosis from a parent with epidermolytic nevus: risk evaluation of transmission from mosaic to germline. J Invest Dermatol 2017; 137: 2024–2026. https://doi.org/10.1016/j.jid.2017.04.036
- Breuss MW, Yang X, Gleeson JG. Sperm mosaicism: implications for genomic diversity and disease. Trends Genet 2021; 37: 890–902. https://doi.org/10.1016/j.tig.2021.05.007
- Mohamad J, Samuelov L, Assaf S, Vodo D, Sarig O, Sprecher E. Epidermolytic epidermal nevus caused by a somatic mutation in KRT2. Pediatr Dermatol 2021; 38: 538–540. https://doi.org/10.1111/pde.14529
- Diociaiuti A, Castiglia D, Corbeddu M, Rotunno R, Rossi S, Pisaneschi E, et al. First case of KRT2 epidermolytic nevus and novel clinical and genetic findings in 26 Italian patients with keratinopathic ichthyoses. Int J Mol Sci 2020; 21: 7707. https://doi.org/10.3390/ijms21207707
- Waldvogel SM, Posey JE, Goodell MA. Human embryonic genetic mosaicism and its effects on development and disease. Nat Rev Genet 2024; 25: 698–714. https://doi.org/10.1038/s41576-024-00715-z