ORIGINAL REPORT
Complete Blood Collection-based Systemic Inflammation Biomarkers as a Severity Biomarker in Alopecia Areata: A Cross-sectional Study
Sihan DENG1,2#, Jundong HUANG1#, Min LI1#, Jia JIAN1 and Wei SHI1*
1Department of Dermatology, Xiangya Hospital, Central South University, Hu Nan Key Laboratory of Aging Biology, Changsha, China and 2Hospital for Skin Diseases, Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College, Nanjing, China
#These authors have contributed equally to this work and share first authorship.
Previous studies have suggested that alopecia areata (AA) is an organ-specific disease characterized by loss of immune privilege of hair follicles. However, an increasing body of research indicates that it not only affects the skin but may also be accompanied by systemic inflammatory reactions. Therefore, searching for simple and easily available biomarkers to describe the underlying systemic inflammation in AA patients is of great clinical significance. Complete blood collection-based systemic inflammation biomarkers have been shown to be associated with the severity and prognosis of various skin and autoimmune diseases. They involve multiple cell lineages and can reveal different pathways of immune-inflammatory responses. The aim of this study was to investigate the level of complete blood collection-based systemic inflammation biomarkers in patients with AA, and to analyse their relationship with the disease severity. A total of 302 AA patients and 296 healthy controls were included in this study and the neutrophil/lymphocyte ratio (NLR), platelet/lymphocyte ratio (PLR), systemic immune inflammation index (SII), and white blood cell/lymphocyte ratio (WLR) were calculated. The differences in these indicators between the 2 groups were compared, and the relationship between NLR, PLR, SII, WLR, and the risk of severe AA were analysed. AA patients had higher NLR, SII, and WLR compared with healthy controls (p = 0.004, 0.002, and 0.002 respectively). PLR and SII were higher in the severe AA group compared with the mild-to-moderate AA patients (p = 0.005 and 0.011 respectively). The risk of severe AA increased with the increasing of PLR, SII, NLR, and WLR (p for trend was 0.001, 0.006, 0.022, and 0.021, respectively). The levels of systemic inflammation biomarkers in AA patients are higher than in healthy people. NLR, PLR, SII, and WLR are risk factors for severe AA, suggesting a close association between systemic inflammation and disease occurrence in AA patients.
SIGNIFICANCE
Alopecia areata is an autoimmune skin disease. While complete blood collection-based systemic inflammation biomarkers have been shown to be associated with the severity and prognosis of various skin and autoimmune diseases, research on their relationship with alopecia areata is limited. This study compared these inflammatory mark-ers between alopecia areata patients and healthy individuals, revealinwg higher levels of certain inflammatory indicators in alopecia areata patients, suggesting a close association between systemic inflammation and the onset of the disease. Our results also suggest that these systemic inflammatory biomarkers are risk factors for severe alopecia areata, and have the potential to serve as early and easily obtained prognostic markers in patients with alopecia areata.
Key words: alopecia areata; complete blood count; platelet to lymphocyte ratio; systemic immune inflammatory index.
Citation: Acta Derm Venereol 2024; 104: adv40971. DOI: https://doi.org/10.2340/actadv.v104.40971.
Copyright: 2024 © The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Jun 10, 2024. Accepted after revision: Sep 22, 2024. Published: Oct 10, 2024
*Corr: Wei Shi, Department of Dermatology, Xiangya Hospital, Central South University, Hu Nan Key Laboratory of Aging Biology, Changsha, China, CN 410005. E-mail: shiwei@csu.edu.cn
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Alopecia areata (AA) is a chronic, inflammatory hair loss disease affecting 0.1% to 0.2% of the general population (1). Treatment approaches are typically based on the disease severity, and systemic drugs are usually reserved for moderate-to-severe cases where topical options have not proved effective (2). With the emergence of effective small-molecule drugs targeting the JAK-STAT pathway, when and whether to initiate targeted systemic therapies in AA patients becomes a question (3).
Recent studies have shown that AA, which was previously thought to be a condition limited to the hair follicles, is associated with systemic inflammation (4–6). Patients with AA have shown a dysregulation in systemic cytokines, including Th1, Th2, and Th17. The severity of the disease has been found to be directly correlated with elevated levels of cytokines such as IL-2, TNF, IL-12, IL-17, and IL-17E in the serum (5). Bain et al. (6) found that the levels of type 17 cytokines IL-17A, IL-17F, IL-21, and IL-23 were increased in patients with AA, and the levels of type 2 cytokines IL-33, IL-31, and IL-17E(IL-25) were also significantly increased. Glickman et al. (7) discovered an imbalance in the expression of multiple cytokines in serum samples from patients with AA. They also sequenced 350 proteins from serum samples of patients with moderate to severe AA and found that the expression of Th1/Th2 and cardiovascular/atherosclerosis-related proteins in patients with moderate and severe AA was increased and correlated with the disease severity (4). Additionally, recent epidemiological studies suggest that patients with AA are at a higher risk of developing diseases associated with systemic inflammation, such as hyperlipidaemia, diabetes mellitus, and metabolic syndrome, compared with control patients (8, 9). Consequently, it is reasonable to speculate that timely initiation of systemic and targeted therapy may be necessary for AA patients with an underlying systemic inflammatory response. However, there is currently a lack of research on inflammatory biomarkers of AA. As such, the search for a convenient, inexpensive, and rapid evaluation indicator to evaluate the level of systemic inflammation in patients with AA is an urgent task in clinical practice.
In the past decade, complete blood collection-based systemic inflammation biomarkers have been widely used, which are deemed to be critical indicators of systemic inflammation and are directly associated with disease severity and outcome measures in patients affected by inflammatory conditions (10–12). Complete blood collection-based systemic inflammation biomarkers include neutrophil/lymphocyte ratio (NLR), platelet/lymphocyte ratio (PLR), systemic immune inflammation index (SII), white blood cell to lymphocyte ratio (WLR), etc., involving multiple cell lines, thus reflecting different pathways of immune inflammation response. Importantly, these indicators are easily obtainable during clinical practice and cause minimal harm to patients, which makes them a crucial factor to consider. However, there are only a few studies investigating blood-based systemic inflammation biomarkers in patients with AA, and such studies were limited by small sample sizes and selected study populations (13, 14).
This study focuses on the evaluation of haematological markers of inflammation derived from complete blood collection in AA.
METHODS
Study design and participants
This study retrospectively investigated clinical and laboratory data of 302 patients with AA who had visited the Department of Dermatology, Xiangya Hospital, Central South University from February 2021 to October 2023. All patients were diagnosed based on clinical manifestation or dermoscopy findings of AA. Patients were excluded if they had received any systemic treatment within 3 months before receiving complete blood collection. Patients with severe kidney and liver disease, metastatic tumours, autoimmune disease, infectious diseases, or those who had recently had surgery were also excluded. Moreover, a sex–age-matched healthy control group was included at the same time, who came from the physical examination centre of the same hospital. All included controls had no previously known cardiovascular, metabolic, inflammatory, or neoplastic diseases. Due to the retrospective nature of the study and the use of anonymized data, the local Institutional Review Board approved the study with a waiver of documented informed consent (approval number: 202312242).
Data collection
Demographic, clinical, and laboratory data were obtained from electronic medical records. The severity of AA was routinely assessed by the validated Severity of Alopecia Tool (SALT) score. The following parameters were extracted: white blood cell count (WBC), absolute neutrophil count (N), absolute lymphocyte count (L), and platelet count (P). To maximize clinical utility, we selected 4 indicators as they are easy to calculate in clinical practice and most widely used in various research. SII was calculated by the formula: N × P/L. By using the absolute blood count values, we also calculated the NLR, PLR, and WLR.
Statistical analysis
Continuous variables were expressed as mean and standard deviation (SD) or median and interquartile range (IQR) according to data distribution, while categorical variables were presented as percentages. For comparisons, Student’s t-test or the Mann–Whitney U test was performed, depending on the normality of the data distribution. The χ2 test was used for categorical variables. Trend analysis of binary logistic regression was utilized to model the relationship between inflammatory markers and severe AA (defined as SALT score ≥ 50). Biomarkers (NLR, PLR, SII, and WLR) were categorized into quartiles, with the lowest quartile as the reference group, then the median of each group was introduced into the logistic regression model as a continuous variable. The confounding factors of age, gender, and BMI were adjusted in Model 2. 95% confidence interval (CI) and p for the trend were calculated for the odds ratio (OR) for severe AA. If the p for trend < 0.05, it indicates the presence of a linear trend between the variables. Restricted cubic spline analysis adjusted for sex, age, and BMI was used to further explore the potential nonlinear relationship between inflammatory biomarkers and the risk of severe AA with 3 knots at the 10th, 60th, and 90th percentiles. Differences were considered statistically significant at p < 0.05, and all p-values were based on 2-sided tests. The SPSS (version IBM SPSS Statistics 26.0; IBM Corp, Armonk, NY, USA) software and R (version 4.3.2; R Foundation for Statistical Computing, Vienna, Austria) were used for statistical calculations.
RESULTS
Demographic and clinical characteristics
A total of 598 patients were included in this study, including 302 patients with AA and 296 healthy controls. The median age of the AA patients was 28.5 (IQR 18.0–40.0), and the ratio of males to females was 1:1.32. There was no statistical difference in gender and age between the AA group and the control group (Table I).
The median disease duration of patients with AA is 16 months, and moderate to severe AA patients (S3–S5) account for 39.07% of cases. Patchy hair loss is the predominant type (84.77%). Among all patients, 37.75% have eyebrow involvement, 21.19% have eyelash involvement, 15.56% have nail involvement, and approximately one-tenth of patients have a family history of AA (Table II).
Comparison of inflammation markers between alopecia areata patients and healthy control
As indicated in Table III, the median white blood cell count and neutrophil count in patients with AA were higher than those in healthy controls (p < 0.001). The median lymphocyte count and platelet count in patients with AA were not significantly different from those in healthy controls. The median NLR, SII, and WLR in the AA group were significantly higher than those in the healthy control group (p = 0.004, 0.002 and 0.002, respectively).
Comparison of inflammatory markers between patients with different severity of alopecia areata
To investigate the relationship between inflammatory markers and the severity of AA, we categorized patients with AA into a severe AA group (n = 118) and mild and moderate AA groups (n = 184). It was found that the median PLR and SII in severe AA group was higher than that of the mild and moderate AA group (p = 0.005 and 0.011 respectively). There were no statistically significant differences in absolute white blood cell count, platelet count, neutrophil count, and lymphocyte count between the 2 groups. In addition, compared with the mild to moderate AA group, the age of patients with severe AA was younger, and the proportion of women was larger (54.24%) (Table IV).
Associations of inflammation markers with the risk of severe alopecia areata
The impact of PLR, SII, NLR, and WLR indicators on the risk of severe AA is presented in Table V. Model 1 represents the crude model without adjusting for confounding factors, while Model 2 represents the model adjusted for age, gender, and BMI. After adjusting for confounders of sex, age, and BMI, the risk of severe AA in the highest quartile of PLR, SII, NLR, and WLR was 2.77 times (95% CI 1.40–5.49) and 2.58 times (95% CI 1.31–5.10), 2.90 times (95% CI 1.40–6.03) and 2.87 (95% CI 1.40–5.90) than that in the lowest quartile, respectively. We performed a restricted cubic spline analysis to understand the nonlinear relationship between the indicators and the risk of severe AA adjusting for sex, age and BMI, and the nonlinear p-values of each indicator were all < 0.05, indicating that there is no non-linear relationships between PLR, SII, NLR, WLR levels and the risk of severe AA (Fig. 1).Moreover, after adjustment for age, gender, and BMI, the p for the trend suggested a linear trend between PLR, SII, NLR, and WLR and the risk of severe AA (p for trend < 0.05). Therefore, the risk of severe AA increased with the increase of PLR, SII, NLR, and WLR.
| Factor | Model 1* | Model 2** | ||
| OR (95%CI) | p-value | OR (95%CI) | p-value | |
| PLR | ||||
| Q1 (< 95.70) | Reference | Reference | ||
| Q2 (95.70–115.99) | 1.25 (0.63–2.49) | 0.520 | 1.16 (0.58–2.33) | 0.680 |
| Q3 (115.99–141.84) | 1.66 (0.85–3.26) | 0.142 | 1.66 (0.84–3.29) | 0.147 |
| Q4 (> 141.84) | 2.61 (1.33–5.11) | 0.005 | 2.77 (1.40–5.49) | 0.004 |
| P for trend | 0.003 | 0.001 | ||
| SII | ||||
| Q1 (< 305.30) | Reference | Reference | ||
| Q2 (305.30–416.54) | 1.40 (0.71–2.74) | 0.333 | 1.36 (0.69–2.69) | 0.379 |
| Q3 (416.54–575.63) | 1.25 (0.63–2.46) | 0.526 | 1.33 (0.67–2.66) | 0.421 |
| Q4 (> 575.63) | 2.45 (1.26–4.78) | 0.009 | 2.58 (1.31–5.10) | 0.006 |
| P for trend | 0.009 | 0.006 | ||
| NLR | ||||
| Q1 (< 1.22) | Reference | Reference | ||
| Q2 (1.22–1.65) | 2.31 (1.17–4.57) | 0.015 | 2.67 (1.32–5.40) | 0.006 |
| Q3 (1.65–2.25) | 1.67 (0.84–3.33) | 0.148 | 2.07 (1.01–4.27) | 0.048 |
| Q4 (> 2.25) | 2.17 (1.09–4.32) | 0.027 | 2.90 (1.40–6.03) | 0.004 |
| P for trend | 0.100 | 0.022 | ||
| WLR | ||||
| Q1 (< 2.46) | Reference | Reference | ||
| Q2 (2.46–3.00) | 2.25 (1.16–4.39) | 0.017 | 2.61 (1.30–5.21) | 0.007 |
| Q3 (3.00–3.59) | 1.51 (0.75–3.04) | 0.244 | 1.83 (0.89–3.76) | 0.103 |
| Q4 (> 3.59) | 2.17 (1.10–4.28) | 0.025 | 2.87 (1.40–5.90) | 0.004 |
| P for trend | 0.090 | 0.021 | ||
| IQR: interquartile range; OR: odds ratio; CI: confidence intervals; NLR: neutrophil to lymphocyte ratio; PLR: platelet to lymphocyte ratio; SII: systemic immune inflammatory response index; WLR: white blood cell to lymphocyte ratio. | ||||
| *Model 1 is the unadjusted model. **Model 2 adjusted for age, sex, and BMI values. | ||||
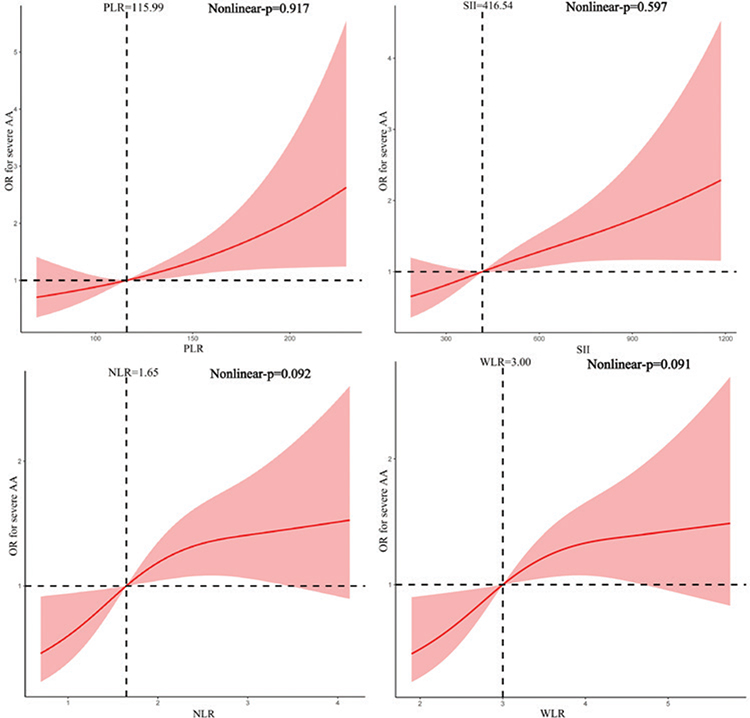
Fig. 1. Restricted cubic spline plots. Relationship between platelet to lymphocyte ratio (PLR) and risk of severe alopecia areata (AA); relationship between systemic immune inflammatory response index (SII) and risk of severe AA; relationship between neutrophil to lymphocyte ratio (NLR) and risk of severe AA; relationship between white blood cell to lymphocyte ratio (WLR) and risk of severe AA. Adjusted by age, sex, and body mass index values.
DISCUSSION
To characterize the underlying systemic inflammatory state in AA, we compared the difference in several complete blood collection-based systemic inflammation biomarkers between AA patients and healthy controls. Our cross-sectional study indicated that AA patients had higher NLR, SII, and WLR compared with the healthy control group. Interestingly, we discovered positive correlations between inflammatory indicators and the disease severity measures in the expected direction, with increasing PLR, SII, NLR, and WLR linked with increased risk of severe AA. These systemic inflammation biomarkers are risk factors for severe AA, suggesting a close association between systemic inflammation and disease occurrence in patients with AA. Our research fills important knowledge gaps in the literature and provides a reference for subsequent clinical applications and related research.
Different from previous studies (13, 14), our study found significant differences in the complete blood collection between the AA population and the control group. Several factors may explain this discrepancy. First, compared with our study all other studies had small sample sizes (range: n = 105–135), which could yield false-negative outcomes. Also, the included population was heterogeneous in terms of severity: our study included patients with varying degrees of severity of alopecia areata, while the previous cohort studies included a sizeable number of mild AA patients (87/105), whose systemic inflammatory response may not differ much from that of the healthy population (14), and another study did not report any measure of disease severity of the included participants (13). In addition, the conflicting results may be attributed partially to ethnic and racial factors. Although it may not be feasible to directly compare our results with those of İslamoğlu et al. (14) and Dere et al. (13), it appears that the healthy controls included in our study exhibited relatively lower levels of inflammation than AA patients.
Neutrophils and lymphocytes are the main cell types mediating inflammation and immune response, which may help understand systemic inflammatory responses by measuring their total count. Although CD8+ T lymphocytes play a key role in the pathogenesis of AA (15), the deficiency of regulatory T cells is also an important contributing factor to the recovery and maintenance of AA, which may be the reason why lymphocytes actively participate in the pathogenesis of AA but the overall number is not significantly different from that of healthy controls (16, 17). Consistent with previous studies (14), we found increased numbers of neutrophils in patients with AA, supporting the view that innate immunity, represented by neutrophils, may be involved in the pathogenesis of AA. Recent studies have revealed that neutrophils, which also play roles in chronic inflammatory conditions and adaptive immune responses, are more pleiotropic than previously thought (18, 19). However, the exact mechanism by which neutrophils are elevated in AA patients is unclear in this study. More research is needed to further explore the role of neutrophils in the pathophysiology of AA.
Previous studies have clearly shown that systemic inflammatory scores, including NLR, PLR, WLR, and SII, reflect the activity of various inflammatory diseases and are considered to be independent prognostic indicators (20–23). For the first time, our findings indicate that the levels of NLR, SII, and WLR in patients with AA are elevated, suggesting the possibility of sub-clinical systemic inflammation, especially in severe cases. In addition, for patients with elevated inflammatory markers, a novel treatment paradigm is needed that focuses on reducing systemic inflammation.
This study has several limitations that should be considered for the interpretation of the findings. First, though we made every effort to adjust for potential confounding in our analyses, data were unavailable to allow further adjustment for several risk factors of AA, including the duration of the current episode of alopecia and pull-test results reflecting disease activity. Second, the cross-sectional study design prevents us from establishing a cause-and-effect relationship. Third, although our dataset is based on an objective record of an electronic medical record system, there was the possibility of selection bias. Fourth, the traditional unspecific inflammatory parameters such as C-reactive protein, IL-6, and erythrocyte sedimentation rate were not included in the analysis. Finally, given the fact that patients with mild AA usually do not need to have a complete blood collection performed, selection bias is inevitable. This may represent a selection bias of patients with more severe disease, with an expected higher level of inflammation. Further prospective multicentre studies are needed to validate these results.
In conclusion, our results suggest that complete blood collection-based systemic inflammation biomarkers are associated with the development and severity of AA. These biomarkers offer clinically significant information and have the potential to serve as an early and easily accessible prognostic marker for AA patients. Further studies, particularly longitudinal assessments of pre- and post-treatment changes, are needed to confirm our findings and emphasize the potential of utilizing laboratory parameters for AA management.
ACKNOWLEDGEMENTS
Ethics statement: This study was conducted in accordance with ethical guidelines and regulations. Due to the retrospective nature of the study and the use of anonymized data, informed consent was waived by the institutional research ethics boards of Xiangya Hospital, Central South University (Changsha, China). The study protocol and data-handling procedures were approved by the institutional research ethics boards of Xiangya Hospital, Central South University (Changsha, China).
All data analysed in this study were anonymized and maintained in strict confidentiality. The use of patient data complied with relevant privacy regulations and ethical standards. No identifiable personal information was used or disclosed in the course of this research.
The waiver of informed consent does not compromise the rights, welfare, or privacy of the participants involved. The study results have been presented in an aggregated and de-identified manner to ensure the protection of participant confidentiality.
We acknowledge the importance of informed consent in research and offer assurance that all other ethical considerations and safeguards were strictly adhered to throughout the study.
REFERENCES
- Dhillon S. Tofacitinib: a review in rheumatoid arthritis. Drugs 2017; 77: 1987–2001. https://doi.org/10.1007/s40265-017-0835-9
- Alkhalifah A, Alsantali A, Wang E, McElwee KJ, Shapiro J. Alopecia areata update: part I. Clinical picture, histopathology, and pathogenesis. J Am Acad Dermatol 2010; 62: 177–188, quiz 189–190. https://doi.org/10.1016/j.jaad.2009.10.032
- Group ACSS, Moussa A, Bennett M, Wall D, Meah N, York K, et al. The Alopecia Areata Severity and Morbidity Index (ASAMI) study: results from a global expert consensus exercise on determinants of alopecia areata severity. JAMA Dermatol 2024; 160: 341–350. https://doi.org/10.1001/jamadermatol.2023.5869
- Glickman JW, Dubin C, Renert-Yuval Y, Dahabreh D, Kimmel GW, Auyeung K, et al. Cross-sectional study of blood biomarkers of patients with moderate to severe alopecia areata reveals systemic immune and cardiovascular biomarker dysregulation. J Am Acad Dermatol 2021; 84: 370–380. https://doi.org/10.1016/j.jaad.2020.04.138
- Waskiel-Burnat A, Osinska M, Salinska A, Blicharz L, Goldust M, Olszewska M, et al. The role of serum th1, th2, and th17 cytokines in patients with alopecia areata: clinical implications. Cells 2021; 10: 3397. https://doi.org/10.3390/cells10123397
- Bain KA, McDonald E, Moffat F, Tutino M, Castelino M, Barton A, et al. Alopecia areata is characterized by dysregulation in systemic type 17 and type 2 cytokines, which may contribute to disease-associated psychological morbidity. Br J Dermatol 2020; 182: 130–137. https://doi.org/10.1111/bjd.18008
- Glickman JW, Dubin C, Dahabreh D, Han J, Del Duca E, Estrada YD, et al. An integrated scalp and blood biomarker approach suggests the systemic nature of alopecia areata. Allergy 2021; 76: 3053–3065. https://doi.org/10.1111/all.14814
- Ly S, Manjaly P, Kamal K, Shields A, Wafae B, Afzal N, et al. Comorbid conditions associated with alopecia areata: a systematic review and meta-analysis. Am J Clin Dermatol 2023; 24: 875–893. https://doi.org/10.1007/s40257-023-00805-4
- Egeberg A, Anderson S, Edson-Heredia E, Burge R. Comorbidities of alopecia areata: a population-based cohort study. Clin Exp Dermatol 2021; 46: 651–656. https://doi.org/10.1111/ced.14507
- Hao X, Li D, Wu D, Zhang N. The relationship between hematological indices and autoimmune rheumatic diseases (ARDs), a meta-analysis. Sci Rep 2017; 7: 10833. https://doi.org/10.1038/s41598-017-11398-4
- Langley BO, Guedry SE, Goldenberg JZ, Hanes DA, Beardsley JA, Ryan JJ. Inflammatory bowel disease and neutrophil-lymphocyte ratio: a systematic scoping review. J Clin Med 2021; 10: 4219. https://doi.org/10.3390/jcm10184219
- Ma R, Cui L, Cai J, Yang N, Wang Y, Chen Q, et al. Association between systemic immune inflammation index, systemic inflammation response index and adult psoriasis: evidence from NHANES. Front Immunol 2024; 15: 1323174. https://doi.org/10.3389/fimmu.2024.1323174
- Dere G, Gundogdu M. Investigation of the relationship between alopecia areata and inflammatory blood parameters. J Cosmet Dermatol 2021; 20: 4048–4051. https://doi.org/10.1111/jocd.14048
- İslamoğlu ZGK, Demirbas A. Evaluation of complete blood cell and inflammatory parameters in patients with alopecia areata: their association with disease severity. J Cosmet Dermatol 2020; 19: 1239–1245. https://doi.org/10.1111/jocd.13131
- Takahashi R, Kinoshita-Ise M, Yamazaki Y, Fukuyama M, Ohyama M. Increase in CD8(+) effector memory T cells re-expressing CD45RA correlates with intractability of severe alopecia areata. J Invest Dermatol 2024; 144: 1654–1657.e7. https://doi.org/10.1016/j.jid.2024.01.006
- Xu W, Wan S, Xie B, Song X. Novel potential therapeutic targets of alopecia areata. Front Immunol 2023; 14: 1148359. https://doi.org/10.3389/fimmu.2023.1148359
- Hamed FN, Astrand A, Bertolini M, Rossi A, Maleki-Dizaji A, Messenger AG, et al. Alopecia areata patients show deficiency of FOXP3+CD39+ T regulatory cells and clonotypic restriction of Treg TCRbeta-chain, which highlights the immunopathological aspect of the disease. PLoS One 2019; 14: e0210308. https://doi.org/10.1371/journal.pone.0210308
- Kolaczkowska E, Kubes P. Neutrophil recruitment and function in health and inflammation. Nat Rev Immunol 2013; 13: 159–175. https://doi.org/10.1038/nri3399
- Deniset JF, Kubes P. Recent advances in understanding neutrophils. F1000Res 2016; 5: 2912. https://doi.org/10.12688/f1000research.9691.1
- Tarkowski B, Lawniczak J, Tomaszewska K, Kurowski M, Zalewska-Janowska A. Chronic urticaria treatment with omalizumab-verification of NLR, PLR, SIRI and SII as biomarkers and predictors of treatment efficacy. J Clin Med 2023; 12: 2639. https://doi.org/10.3390/jcm12072639
- Zhao X, Li J, Li X. Association between systemic immune-inflammation index and psoriasis: a population-based study. Front Immunol 2024; 15: 1305701. https://doi.org/10.3389/fimmu.2024.1305701
- Utlu Z. Evaluation of systemic immune and inflammatory biomarkers in hidradenitis suppurativa. Eur Rev Med Pharmacol Sci 2023; 27: 9267–9272.
- Andersen CSB, Kvist-Hansen A, Siewertsen M, Enevold C, Hansen PR, Kaur-Knudsen D, et al. Blood cell biomarkers of inflammation and cytokine levels as predictors of response to biologics in patients with psoriasis. Int J Mol Sci 2023; 24: 6111. https://doi.org/10.3390/ijms24076111