ORIGINAL REPORT
Patients with Persistent Mild Psoriasis after Treatment with Ustekinumab Achieved Greater Improvements in Skin Clearance and Patient-reported Outcomes after Switching to Guselkumab in the Phase 3 NAVIGATE Trial
Enzo ERRICHETTI1, Peter WOLF2, Saakshi KHATTRI3, Patricia GORECKI4, Megan MILLER5, Jingzhi JIANG5, Chenglong HAN6 and Brian KIRBY7
1University Hospital “Santa Maria della Misericordia”, Udine, Italy, 2Department of Dermatology, Medical University of Graz, Graz, Austria, 3Mount Sinai Doctors, New York, NY, USA, 4Janssen-Cilag Ltd, High Wycombe, UK, 5Janssen Research and Development, LLC, Spring House, PA, USA, 6Janssen Global Services, LLC, Malvern, PA, USA and 7St. Vincent’s University Hospital and Charles Institute of Dermatology, University College Dublin, Ireland
Mild psoriasis may be burdensome; if symptoms are inadequately controlled, switching therapy may be warranted. In the Phase 3 NAVIGATE trial, patients with moderate-to-severe plaque psoriasis received ustekinumab for 16 weeks. Patients with inadequate response (Investigator’s Global Assessment [IGA] ≥ 2) were randomized to switch to guselkumab or continue ustekinumab. This post-hoc analysis evaluated the patient subgroup with residual mild psoriasis (IGA = 2) after initial ustekinumab therapy. Outcomes assessed included the Psoriasis Area and Severity Index (PASI), Dermatology Life Quality Index (DLQI), and Psoriasis Symptoms and Signs Diary (PSSD). Initially, 871 patients received ustekinumab. At Week 16, 161 randomized patients had residual mild psoriasis (IGA = 2). Among guselkumab- vs ustekinumab-treated patients at Week 28, 59.0% vs 27.7% achieved PASI 90, and 50.0% vs 21.0% achieved DLQI 0/1. Mean changes from baseline in PSSD score were –44 vs –28 and –50 vs –32, respectively, with thresholds of –40 considered clinically meaningful. Mean changes in PSSD itch score were –4.6 vs –2.9, with reductions ≥ 4.0 considered clinically meaningful. Treatment differences were maintained/increased through Week 52. Among patients with residual mild psoriasis after 16 weeks of ustekinumab, those switching to guselkumab had greater improvements in skin clearance, health-related quality of life, and patient-reported symptoms and signs than those continuing ustekinumab.
Key words: psoriasis; biologic therapy; patient-reported outcome measures; quality of life; guselkumab; ustekinumab.
SIGNIFICANCE
Little is known about outcomes of patients with residual psoriasis after switching biologic therapies. Given that mild psoriasis may involve substantial disease burden, this post-hoc analysis of the NAVIGATE trial examined patients with residual mild psoriasis after 16 weeks of treatment with ustekinumab who were randomized at Week 16 to remain on ustekinumab or switch to guselkumab through Week 52. Patients with residual mild psoriasis who switched to guselkumab achieved greater improvements in psoriasis disease activity, skin-related quality of life, and symptoms and signs of psoriasis than those who remained on ustekinumab through to Week 52.
Citation: Acta Derm Venereol 2024; 104: adv41053. DOI: https://doi.org/10.2340/actadv.v104.41053.
Copyright: © 2024 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Jun 24, 2024; Accepted: Aug 14, 2024; Published: Sep 5, 2024
Corr: Enzo Errichetti, University Hospital “Santa Maria della Misericordia”, Piazzale Santa Maria della Misericordia 15, IT-33100 Udine, Italy. Email: enzoerri@yahoo.it
Competing interests and funding: EE has worked as a consultant for AbbVie, Amgen, and Janssen. PW has carried out clinical trials for and/or has received honoraria as a consultant and/or speaker from AbbVie, Almirall, Amgen, Boehringer Ingelheim, Celgene, Eli Lilly, Janssen, LEO, Merck Sharp & Dohme, Novartis, Pfizer, Sandoz, and UCB. SK has received support for research from Bristol Myers Squibb, Celgene, LEO, Pfizer, and Takeda; as a speaker from AbbVie, Arcutis, Bristol Myers Squibb, Eli Lilly, Janssen, LEO, Pfizer, Regeneron, Sanofi, UCB; and as a consultant for AbbVie, Eli Lilly, Janssen, Regeneron, Sanofi, and UCB. PG was an employee of Janssen-Cilag Ltd of Johnson & Johnson at the time of this research; MG and JJ are employees of Janssen Research & Development, LLC of Johnson & Johnson; CH is an employee of Janssen Global Services of Johnson & Johnson; employees own stock/stock options in Johnson & Johnson, of which Janssen is a subsidiary. BK has received research support from/was a principal investigator (clinical trials) for AbbVie, Almirall, Janssen, Merck Sharpe & Dohme, Moonlake, Novartis, Pfizer, and UCB; been a consultant for AbbVie, Almirall, Celgene, Janssen, MC2 Therapeutics, Merck Sharpe & Dohme, Moonlake, Novartis, Pfizer, UCB, and Union; received honoraria from AbbVie, Almirall, Celgene, Janssen, Lilly, MC2 therapeutics, Moonlake, Novartis, Pfizer, Union, and UCB; and been on scientific advisory boards for AbbVie, Almirall, Celgene, GlaxoSmithKline, Janssen, Lilly, MC2 Therapeutics, Moonlake, Novartis, Pfizer, and UCB.
This work was supported by Janssen Research & Development, LLC.
INTRODUCTION
Treatment of plaque psoriasis has improved considerably in recent years, making high levels of skin clearance an achievable goal (1–4). Patients who do not achieve clear skin or minimal disease activity, despite treatment, are likely to experience persistent morbidity from psoriasis and be dissatisfied with their treatment (1, 5–8). Patients with psoriasis treated with topical, nonbiologic systemic, or biologic therapies often have residual mild psoriasis that causes persistent symptoms, such as itch and pain, and has a negative impact on their health-related quality of life (HRQoL); many of these patients experience a lack or loss of therapeutic response (5–9). Switching to an alternative treatment, especially one with a different mechanism of action, may improve outcomes (4, 10).
In the Phase 3 NAVIGATE clinical trial of patients with moderate-to-severe plaque psoriasis (11), approximately one-third of patients had residual psoriasis that was mild, moderate, or severe (based on Investigator’s Global Assessment [IGA]) after 16 weeks of treatment with ustekinumab, a fully human monoclonal antibody that targets the p40 subunit of interleukin (IL)-12 and IL-23 (12). These patients were randomized to either continue ustekinumab or switch to guselkumab, a fully human monoclonal antibody that targets the p19 subunit of IL-23 (13). Ustekinumab-inadequate responders who switched to guselkumab achieved significantly lower disease activity, better HRQoL, and fewer symptoms and signs of psoriasis compared with those who continued treatment with ustekinumab (11).
However, there is a lack of information regarding outcomes after a treatment switch in patients with residual psoriasis of mild severity following biological therapy. Here we report post hoc analyses of patients with residual psoriasis of mild severity after initial treatment with ustekinumab in the NAVIGATE clinical trial (11), comparing outcomes after a subsequent switch to guselkumab with those after continued treatment with ustekinumab.
MATERIALS AND METHODS
Patients and trial design
Patient recruitment criteria and the design of the NAVIGATE trial have been published previously (11). Briefly, patients ≥ 18 years of age with a diagnosis of moderate-to-severe plaque psoriasis for ≥ 6 months, a Psoriasis Area and Severity Index (PASI) ≥ 12, an IGA ≥ 3, body surface area involvement ≥ 10%, and who were candidates for phototherapy or systemic treatment for psoriasis were enrolled. Exclusion criteria included severe, progressive, and uncontrolled illnesses, malignancy (except for nonmelanoma skin cancer and cervical cancer in situ) within 5 years of screening, current infections including active tuberculosis, and prior use of guselkumab or ustekinumab. Limitations were imposed on the use of specific biologic, systemic, and phototherapeutic treatments prior to administration of study drug.
NAVIGATE was a Phase 3, randomized, double-blind clinical trial conducted between October 2014 and May 2016 that used an enrichment design (14]). All patients participated in a 16-week open-label treatment period, during which they received ustekinumab (dosed according to bodyweight [45 mg for patients ≤ 100 kg or 90 mg for patients > 100 kg]) at Weeks 0 and 4. At Week 16, response to ustekinumab was assessed. Inadequate response was defined as an IGA score of 2 (mild), 3 (moderate), or 4 (severe) psoriasis (15). Patients with an inadequate response to ustekinumab at Week 16 (IGA ≥ 2) were randomized (1:1) to receive guselkumab 100 mg at Weeks 16, 20, and every 8 weeks thereafter through Week 44 or to continue receiving ustekinumab at Weeks 16, 28, and 40. Patients with a Week 16 IGA score of 0 or 1 continued treatment with ustekinumab at Weeks 16, 28, and 40.
The protocol was approved by the investigational review board (IRB)/ethics committee (EC) at each site. Central IRBs/ECs included Sterling IRB (USA), Bellberry Ltd (Australia), IRB Services (Canada), North West – Liverpool East Research EC (UK), Komisja Bioetyczna (Poland), and the Independent Interdisciplinary Committee for Ethics Expertise of Clinical Trials (Russia); several different regional IRBs/ECs approved the protocol at sites in Germany, Korea, Spain, and Taiwan. All patients gave written informed consent before any study-related procedures were performed. The trial was registered with EudraCT (2014-000721-20) and clinicaltrials.gov (NCT02203032).
Assessments
In this post hoc analysis of patients with residual mild psoriasis (IGA = 2) at Week 16, clinical efficacy was evaluated based on PASI responses (16). PASI 90 and PASI 100 responses, respectively, represent achievement of ≥ 90% or 100% improvement from baseline. Efficacy evaluations were performed at baseline, every 4 weeks until Week 44, and at Week 52.
Patient-reported outcome measures (PROMs) included the Dermatology Life Quality Index (DLQI) and the Psoriasis Symptoms and Signs Diary (PSSD). The DLQI (scale 0–30) includes 6 domains assessing the effects of psoriasis on HRQoL (17). The PSSD measures patient-reported severity of psoriasis symptoms (itch, pain, stinging, burning, and skin tightness) and observable signs (dryness, cracking, scaling, shedding or flaking, redness, and bleeding) over the previous 7 days using 0–10 numerical rating scales (18, 19). The combined total PSSD Symptoms score and the combined total PSSD Signs score range from 0–100. For both the DLQI and PSSD, higher scores indicate greater disease severity. PROMs were assessed at baseline and Weeks 16, 28, 32, 36, 40, and 52.
Statistical analysis
Percentages, with 95% confidence intervals (CI), are presented for categorical variables. Descriptive statistics, such as mean and standard error, are presented for continuous variables. The value 0 was assigned to changes from baseline for treatment failure (i.e., discontinuation of study treatment due to lack of efficacy or an adverse event of worsening of psoriasis, or initiation of a protocol-prohibited medication/therapy), and last observation carried forward was applied for remaining missing data. Non-responder imputation was applied after treatment failure or missing data for binary endpoints. For PSSD, least-squares mean differences (95% CIs) between guselkumab and ustekinumab were calculated using a mixed model for repeated measures, with treatment, visit, baseline weight (≤ 100 kg or > 100 kg), baseline PSSD score, and interaction of treatment group and visit as covariates.
RESULTS
Patient demographics and disease characteristics
As previously described, in the NAVIGATE trial (11), 871 patients were treated with open-label ustekinumab. After 16 weeks of treatment with ustekinumab, 268 patients (30.8%) had residual psoriasis (IGA ≥ 2). Of these, 161 (60.1%) had residual psoriasis of mild severity (IGA = 2) and represent the focus of the post hoc analyses reported here. Baseline characteristics were generally comparable for patients randomized to switch to guselkumab (n = 78) or to continue ustekinumab (n = 83) (Table I). However, patients randomized to guselkumab had a longer disease duration (18.6 vs 15.2 years), and a lower proportion had bodyweight > 100 kg (21.8% vs 26.5%).
| Cohort | All patients | Patients not randomized at Week 16 (IGA = 0 or 1) | Patients randomized at Week 16 | |||
| Patients with PsO disease activity of IGA ≥2 at Week 16 | Subset of patients with mild PsO (IGA = 2) at Week 16 | |||||
| Treatment up to Week 16 | UST | UST | UST | UST | UST | UST |
| Treatment from Week 16 forward | GUS or UST | UST | GUS | UST | GUS | UST |
| Patients, n | 871 | 585 | 135 | 133 | 78 | 83 |
| Age, years, mean (SD) | 43.1 (13.2) | 42.9 (13.1) | 44.2 (13.4) | 43.0 (13.7) | 44.5 (13.5) | 42.5 (13.6) |
| Male sex, n (%) | 566 (65.0) | 372 (63.6) | 95 (70.4) | 88 (66.2) | 55 (70.5) | 54 (65.1) |
| Weight, kg | 88.3 (22.0) | 86.8 (20.6) | 90.3 (22.2) | 91.3 (25.8) | 87.0 (20.9) | 89.8 (23.5) |
| ≤ 100 kg, n (%) | 640 (73.5) | 436 (74.5) | 98 (72.6) | 96 (72.2) | 61 (78.2) | 61 (73.5) |
| > 100 kg, n (%) | 231 (26.5) | 149 (25.5) | 37 (27.4) | 37 (27.8) | 17 (21.8) | 22 (26.5) |
| Disease duration, years, mean (SD) | 16.8 (12.2) | 16.7 (12.3) | 18.2 (12.7) | 15.6 (10.9) | 18.6 (12.7) | 15.2 (10.3) |
| Psoriatic arthritis, n (%) | 128 (14.7) | 77 (13.2) | 28 (20.7) | 21 (15.8) | 13 (16.7) | 10 (12.0) |
| IGA (0–4), n (%) | ||||||
| Mild (2), mean (SD) | 1 (0.1) | 0 | 0 | 0 | 0 | 0 |
| Moderate (3), mean (SD) | 694 (79.7) | 477 (81.5) | 103 (76.3) | 100 (75.2) | 63 (80.8) | 67 (80.7) |
| Severe (4), mean (SD) | 176 (20.2) | 108 (18.5) | 32 (23.7) | 33 (24.8) | 15 (19.2) | 16 (19.3) |
| PASI score (0–72), mean (SD) | 21.6 (9.2) | 21.1 (9.2) | 22.6 (9.3) | 22.8 (9.4) | 22.2 (9.2) | 21.9 (8.9) |
| DLQI (0–30), mean (SD) | 14.5 (7.2) | 14.2 (7.1) | 15.5 (7.9) | 14.4 (6.7) | 16.5 (7.6) | 14.3 (7.0) |
| PSSD, n | 866 | 584 | 133 | 132 | 76 | 82 |
| PSSD symptoms score (0–100), mean (SD) | 50.6 (24.7) | 48.7 (24.0) | 55.7 (25.5) | 52.9 (25.6) | 57.2 (26.5) | 53.2 (26.0) |
| PSSD sign scores (0–100), mean (SD) | 60.7 (20.4) | 58.8 (20.1) | 64.9 (20.3) | 63.7 (20.8) | 65.7 (20.4) | 63.7 (21.2) |
| DLQI: Dermatology Life Quality Index; GUS: guselkumab; IGA: Investigator’s Global Assessment; PASI: Psoriasis Area and Severity Index; PsO: psoriasis; PSSD: Psoriasis Symptoms and Signs Diary; UST: ustekinumab; SD: standard deviation. | ||||||
Achievement of PASI 90 and PASI 100 responses
After randomization at Week 16, greater proportions of patients with residual psoriasis of mild severity achieved PASI 90 and PASI 100 responses in the guselkumab group than in the ustekinumab group (Fig. 1A). At Week 24, PASI 90 response rates were 47.4% with guselkumab and 31.3% with ustekinumab; PASI 100 response rates were 10.3% and 7.2%, respectively. Greater responses for the guselkumab group were maintained through the final assessment at Week 52 than for the ustekinumab group (PASI 90: 59.0% vs 26.5%; PASI 100: 21.8% vs 9.6%, respectively, Fig. 1A).

Fig. 1. PASI and DLQI outcomes among patients with residual mild psoriasis (IGA = 2) at Week 16 after initial treatment with ustekinumab: (A) proportion (95% CI) of patients achieving PASI 90 or PASI 100 responses; (B) proportion (95% CI) of patients with a DLQI of 0 or 1. †Week of randomization. ‡Patients with baseline (Week 0) DLQI > 1. CI: confidence interval; DLQI: Dermatology Life Quality Index; IGA: Investigator’s Global Assessment; PASI: Psoriasis Area and Severity Index.
Achievement of DLQI of 0 or 1
Greater proportions of patients with residual psoriasis of mild severity receiving guselkumab achieved a DLQI of 0 or 1, indicating minimal or no effect of psoriasis on HRQoL, than those receiving ustekinumab (Fig 1B). At Week 28, 50.0% of patients in the guselkumab group vs 21.0% in the ustekinumab group achieved a DLQI of 0 or 1, and differences favouring guselkumab were maintained through to Week 52 (Fig. 1B).
Symptoms and signs of psoriasis
After 16 weeks of treatment with ustekinumab, mean improvements from baseline (Week 0) in the combined PSSD Symptoms score and combined PSSD Signs score among patients with residual mild psoriasis ranged from 33.9 to 38.4 points. After randomization, patients who switched to guselkumab showed further improvement. In contrast, PSSD Symptoms and Signs scores remained stable or worsened among those who continued ustekinumab treatment (Fig. 2). At Week 28, the differences (95% CI) between the guselkumab and ustekinumab groups in change from baseline in PSSD Symptoms and Signs scores were 15.7 (9.0, 22.3) and 17.1 (10.8, 23.3), respectively, in favour of guselkumab. These differences were maintained through Week 52. Furthermore, in guselkumab-treated patients, mean improvements in combined PSSD Symptoms and Signs scores exceeded clinically meaningful thresholds (≥ 40 for both) (20) at all timepoints assessed; these thresholds were generally not met for ustekinumab-treated patients (Fig. 2).

Fig. 2. Mean standard error (SE) change from baseline (Week 0) in Psoriasis Symptoms and Signs Diary (PSSD) combined symptoms or combined signs scores. *n = 80 at Week 16. †Week of randomization. ‡Armstrong et al., 2019 (20). Δ = least-squares mean treatment difference between guselkumab and ustekinumab; CI: confidence interval.
In addition, greater proportions of guselkumab-treated patients became symptom-free and/or sign-free (PSSD = 0) compared with ustekinumab-treated patients (Fig. S1). At Week 40, the proportions of patients with complete resolution of PSSD symptoms and signs for the guselkumab group were 25.3% and 14.5%, respectively, compared with 9.8% and 3.7% for the ustekinumab group. Differences between treatment groups were maintained through the final assessments at Week 52.
At Week 32, mean improvements from baseline for all individual PSSD item scores were greater with guselkumab than with ustekinumab treatment (Table II). Furthermore, mean improvements from baseline with guselkumab treatment exceeded clinically meaningful thresholds for each individual item; with ustekinumab treatment, only the PSSD Sign score for dryness reached the clinically meaningful threshold. These treatment effects were maintained through Week 52.
| Week | Mean improvementa from Week 0 (SE) | Clinically meaningful improvementb | ||
| Guselkumab (n = 76) | Ustekinumab (n = 82) | |||
| Symptoms | ||||
| Itch | 32 | 5.1 (0.3) | 3.7 (0.3) | ≥ 4 |
| 52 | 4.7 (0.4) | 2.9 (0.4) | ||
| Pain | 32 | 5.1 (0.3) | 3.5 (0.4) | ≥ 4 |
| 52 | 4.6 (0.4) | 2.8 (0.4) | ||
| Stinging | 32 | 3.8 (0.4) | 2.3 (0.4) | ≥ 3 |
| 52 | 3.3 (0.4) | 1.5 (0.4) | ||
| Burning | 32 | 4.4 (0.4) | 3.3 (0.4) | ≥ 4 |
| 52 | 4.1 (0.4) | 2.7 (0.4) | ||
| Skin tightness | 32 | 5.1 (0.3) | 3.7 (0.3) | ≥ 4 |
| 52 | 4.7 (0.3) | 2.9 (0.4) | ||
| Signs | ||||
| Dryness | 32 | 5.2 (0.3) | 4.1 (0.3) | ≥ 4 |
| 52 | 4.9 (0.3) | 3.3 (0.3) | ||
| Cracking | 32 | 5.0 (0.3) | 3.7 (0.4) | ≥ 4 |
| 52 | 4.6 (0.4) | 3.0 (0.4) | ||
| Scaling | 32 | 5.5 (0.3) | 4.2 (0.3) | ≥ 5 |
| 52 | 5.3 (0.4) | 3.4 (0.4) | ||
| Shedding or flaking | 32 | 6.0 (0.3) | 4.8 (0.3) | ≥ 5 |
| 52 | 5.8 (0.3) | 3.7 (0.4) | ||
| Redness | 32 | 6.0 (0.3) | 4.3 (0.3) | ≥ 5 |
| 52 | 5.8 (0.3) | 3.3 (0.3) | ||
| Bleeding | 32 | 3.6 (0.3) | 2.4 (0.3) | ≥ 3 |
| 52 | 3.4 (0.3) | 1.9 (0.3) | ||
| aImprovement = reduction from baseline in PSSD score. bClinically meaningful reductions from baseline (Armstrong, 2019).20 PSSD: Psoriasis Symptoms and Signs Diary; SE: standard error. | ||||
For the PSSD symptom of itch, mean improvements from baseline at Weeks 28–52 were greater with guselkumab compared with ustekinumab; only the guselkumab group achieved mean improvements above the clinically meaningful threshold of ≥ 4.0 (Fig. 3). A treatment difference (95% CI) of 1.7 (0.9, 2.4) was observed as early as 12 weeks after randomization.

Fig. 3. Mean standard error (SE) change from baseline in Psoriasis Symptoms and Signs Diary (PSSD) itch symptom score. *n = 80 at Week 16. †Week of randomization. ‡Armstrong et al., 2019 (20). Δ = least-squares mean treatment difference between guselkumab and ustekinumab; CI: confidence interval.
Complete resolution of each of the individual symptoms and signs of psoriasis (individual PSSD score = 0) at Week 52 was observed in a greater proportion of patients receiving guselkumab than ustekinumab (Fig. 4). Higher levels of response with guselkumab were seen as early as Week 32 (16 weeks after randomization) (Fig. S2).
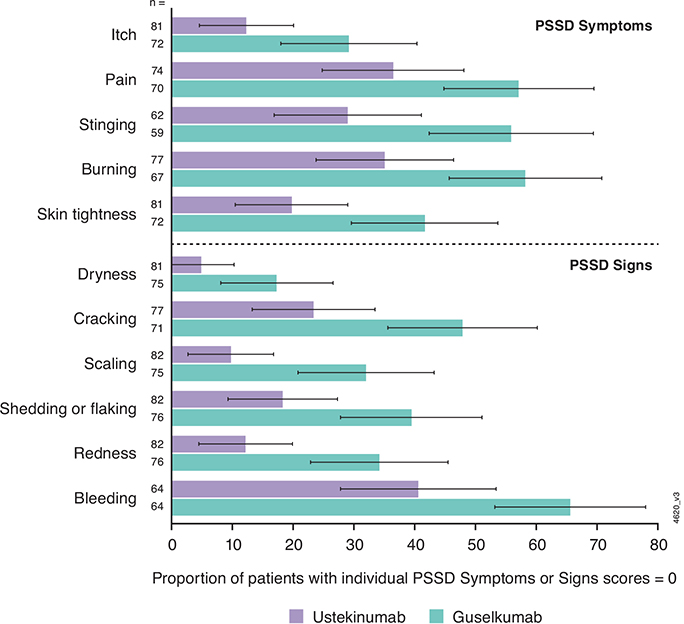
Fig. 4. Proportions (95% confidence interval) of patients who achieved absence of individual Psoriasis Symptoms and Signs Diary (PSSD) symptoms or signs of psoriasis (PSSD = 0) at Week 52.
Finally, when focusing the PSSD analysis on patients with high levels of skin clearance (PASI 90 or PASI 100), mean improvement from baseline for most PSSD items was greater with guselkumab than with ustekinumab treatment at Week 40; these differences were maintained through to the final assessments at Week 52 (Table SI). As expected among these high responders, all mean improvements from baseline for individual PSSD symptoms and signs were clinically meaningful in the guselkumab group; most mean improvements were also clinically meaningful in the ustekinumab group.
DISCUSSION
The Phase 3 NAVIGATE trial examined clinical outcomes among patients with moderate-to-severe plaque psoriasis who had an inadequate response (IGA ≥ 2) after 16 weeks of treatment with ustekinumab and were randomized to either switch to guselkumab or continue treatment with ustekinumab (11). We report outcomes for the subgroup of patients with residual psoriasis of mild severity (IGA = 2) after initial treatment with ustekinumab who were then randomized based on their inadequate response. Compared with continuing treatment with ustekinumab, switching to guselkumab resulted in higher PASI 90 and PASI 100 response rates, greater proportions of patients achieving minimal or no effect of psoriasis on HRQoL (DLQI of 0 or 1), and greater relief from psoriasis symptoms and signs (assessed with the PSSD).
Studies have shown that mild psoriasis can be associated with substantial disease burden and negative effects on HRQoL (1, 5–9). PROMs capture individual patient experiences of disease burden, which are not necessarily reflected by efficacy measures such as the PASI and IGA (20, 21). For this reason, dermatologists recognize the importance of PROMs in psoriasis treatment decisions (22). One PROM used to evaluate the disease burden of plaque psoriasis is the PSSD (18), which was developed using patient interviews, published reports, and guidance from the US Food and Drug Administration (23). This instrument demonstrated strong psychometric properties in the NAVIGATE trial, including significant positive correlations with PASI, IGA, and DLQI (19).
In this analysis, changes from baseline in PSSD Symptoms and Signs scores were greater with guselkumab than ustekinumab after randomization. Similarly, improvements in individual PSSD item scores (symptoms: itch, pain, stinging, burning, and skin tightness; and signs: dryness, cracking, scaling, shedding or flaking, redness, and bleeding) were greater with guselkumab treatment than with ustekinumab. The changes from baseline in PSSD (both combined and individual scores) with guselkumab all exceeded established thresholds for clinically meaningful improvement (19), whereas these thresholds were generally not met with ustekinumab treatment.
Comparable trends were observed for the proportions of patients who achieved complete resolution of combined PSSD Symptoms and/or combined PSSD Signs (symptom-free and/or sign-free status) as well as complete resolution of individual PSSD items; PSSD scores of 0 were more frequently observed among patients treated with guselkumab compared with ustekinumab. Among the most common psoriasis symptoms, itch can be especially troubling and difficult to control (1, 6, 8, 20, 24–26). Greater improvement in PSSD itch score with guselkumab vs ustekinumab was observed as early as 12 weeks after randomization and was maintained up to the final assessment. Furthermore, in the guselkumab group, the change from baseline in PSSD itch score was clinically meaningful.
To our knowledge, this is the first report comparing outcomes for patients experiencing an inadequate response to biologic treatment with residual psoriasis of exclusively mild severity (IGA = 2) who either switched to a different biologic therapy or continued with their initial regimen. Most of the patients included in this analysis had not achieved PASI 90 at the time of randomization at Week 16, supporting the hypothesis that PASI 90 and PASI 100 responses could be used as sensitive measures of treatment differences in patients who switched to guselkumab vs continued with ustekinumab.
Limitations
Limitations of the analyses include their post hoc nature, the relatively small numbers of patients, and the inability to evaluate statistical significance for the observed differences. Baseline characteristics were generally similar for patients randomized to switch to guselkumab vs continue ustekinumab; however, patients in the guselkumab group had a longer mean psoriasis disease duration (18.6 vs 15.2 years) and were less likely to have a bodyweight greater than 100 kg (21.8% vs 26.5%); these differences are likely a result of the relatively small sample size. Notably, ustekinumab dosing and statistical analysis of treatment differences were both pre-specified to correct for variations in bodyweight, because bodyweight is known to influence ustekinumab efficacy (27). In contrast, guselkumab dosing is not based on bodyweight, and the treatment effects of guselkumab are more consistent across bodyweight quartiles compared with other biologics (28, 29).
We did not perform additional safety analyses in this subset of patients from NAVIGATE with residual psoriasis of mild severity after induction therapy with ustekinumab. However, as previously reported, both guselkumab and ustekinumab were well tolerated in the overall NAVIGATE study population (11), and both guselkumab (30) and ustekinumab (31) have well-established safety profiles based on robust clinical development programmes and post-marketing studies in psoriasis.
Conclusion
The results reported here demonstrate that patients with residual psoriasis of even mild severity (IGA = 2) after 16 weeks of treatment with ustekinumab can benefit from a switch to guselkumab, as did the full non-responder group in the NAVIGATE trial, which also included patients with psoriasis of greater severity (IGA ≥ 2) (11). Among patients with IGA = 2 after 16 weeks of ustekinumab treatment, greater proportions of those who switched to guselkumab achieved PASI 90 and PASI 100 responses, improvement in skin-related HRQoL, and reduction of psoriasis symptoms and signs compared with those who continued ustekinumab treatment.
ACKNOWLEDGEMENTS
Medical writing support was provided by Elizabeth Rosenberg, PhD, of Kelly Science and Clinical, and Cherie Koch, PhD, of Janssen Scientific Affairs, under the direction of the authors in accordance with Good Publication Practice guidelines (Ann Intern Med 2022; 175: 1298–304).
IRB approval status: The study was conducted in accordance with ethical principles that have their origin in the Declaration of Helsinki and are consistent with Good Clinical Practice. All study protocols were approved by an institutional review board or ethics committee. All participants provided written informed consent.
REFERENCES
- Korman NJ, Malatestinic W, Goldblum OM, Murage MJ, Renda L, Lin C-Y, et al. Assessment of the benefit of achieving complete versus almost complete skin clearance in psoriasis: a patient’s perspective. J Dermatolog Treat 2022; 33: 733–739. https://doi.org/10.1080/09546634.2020.1772454
- Puig L, Thom H, Mollon P, Tian H, Ramakrishna GS. Clear or almost clear skin improves the quality of life in patients with moderate-to-severe psoriasis: a systematic review and meta-analysis. J Eur Acad Dermatol Venereol 2017; 31: 213–220. https://doi.org/10.1111/jdv.14007
- Fairchild AO, Reed SD, Johnson FR, Anglin G, Wolka AM, Noel RA. What is clearance worth? Patients’ stated risk tolerance for psoriasis treatments. J Dermatolog Treat 2017; 28: 709–715. https://doi.org/10.1080/09546634.2017.1329499
- Carretero G, Puig L, Carrascosa JM, Ferrándiz L, Ruiz-Villaverde R, de la Cueva P, et al. Redefining the therapeutic objective in psoriatic patients candidates for biological therapy. J Dermatolog Treat 2018; 29: 334–346. https://doi.org/10.1080/09546634.2017.1395794
- Armstrong AW, Robertson AD, Wu J, Schupp C, Lebwohl MG. Undertreatment, treatment trends, and treatment dissatisfaction among patients with psoriasis and psoriatic arthritis in the United States: findings from the National Psoriasis Foundation surveys, 2003–2011. JAMA Dermatol 2013; 149: 1180–1185. https://doi.org/10.1001/jamadermatol.2013.5264
- Lebwohl M, Langley RG, Paul C, Puig L, Reich K. van de Kerkhof P, et al. Evolution of patient perceptions of psoriatic disease: results from the Understanding Psoriatic Disease Leveraging Insights for Treatment (UPLIFT) survey. Dermatol Ther (Heidelb) 2022; 12: 61–78. https://doi.org/10.1007/s13555-021-00635-4
- Gupta S, Garbarini S, Nazareth T, Khilfeh I, Costantino H, Kaplan D. Characterizing outcomes and unmet needs among patients in the United States with mild-to-moderate plaque psoriasis using prescription topicals. Dermatol Ther (Heidelb) 2021; 11: 2057–2075. https://doi.org/10.1007/s13555-021-00620-x
- Korman NJ, Zhao Y, Pike J, Roberts J, Sullivan E. Increased severity of itching, pain, and scaling in psoriasis patients is associated with increased disease severity, reduced quality of life, and reduced work productivity. Dermatol Online J 2015; 21: 13030/qt1x16v3dg. https://doi.org/10.5070/D32110028943
- Strober B, Greenberg JD, Karki C, Mason M, Guo N, Hur P, et al. Impact of psoriasis severity on patient-reported clinical symptoms, health-related quality of life and work productivity among US patients: real-world data from the Corrona Psoriasis Registry. BMJ Open 2019; 9: e027535. https://doi.org/10.1136/bmjopen-2018-027535
- Menter A, Strober BE, Kaplan DH, Kivelevitch D, Prater EF, Stoff B, et al. Joint AAD-NPF guidelines of care for the management and treatment of psoriasis with biologics. J Am Acad Dermatol 2019; 80: 1029–1072. https://doi.org/10.1016/j.jaad.2018.11.057
- Langley RG, Tsai T-F, Flavin S, Song M, Randazzo B, Wasfi Y, et al. Efficacy and safety of guselkumab in patients with psoriasis who have an inadequate response to ustekinumab: results of the randomized, double-blind, phase III NAVIGATE trial. Br J Dermatol 2018; 178: 114–123. https://doi.org/10.1111/bjd.15750
- Stelara. (ustekinumab) [package insert]. Horsham, PA: Janssen Pharmaceutical Companies; 2022.
- Tremfya. (guselkumab) [package insert]. Horsham, PA: Janssen Pharmaceutical Companies; 2020.
- United States Department of Health and Human Services FaDA. Enrichment strategies for clinical trials to support approval of human drugs and biological products. U.S. Department of Health and Human Services, 2019. Available from: https://www.fda.gov/media/121320/download (last accessed May 24, 2024).
- Langley RGB, Feldman SR, Nyirady J, van de Kerkhof P, Papavassilis. The 5-point Investigator’s Global Assessment (IGA) Scale: a modified tool for evaluating plaque psoriasis severity in clinical trials. J Dermatolog Treat 2015; 26: 23–31. https://doi.org/10.3109/09546634.2013.865009
- Fredriksson T, Pettersson U. Severe psoriasis – oral therapy with a new retinoid. Dermatologica 1978; 157: 238–244. https://doi.org/10.1159/000250839
- Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI) – a simple practical measure for routine clinical use. Clin Exp Dermatol 1994; 19: 210–216. https://doi.org/10.1111/j.1365-2230.1994.tb01167.x
- Feldman SR, Mathias SD, Schenkel B, Colwell HH, McQuarrie K, Randazzo B, et al. Development of a patient-reported outcome questionnaire for use in adults with moderate-to-severe plaque psoriasis: the Psoriasis Symptoms and Signs Diary. J Dermatol and Dermatol Treat 2016; 20: 19–26. https://doi.org/10.1016/j.jdds.2015.07.004
- Armstrong A, Puig L, Langley R, Tsai TF, Song M, Wasfi Y, et al. Validation of psychometric properties and development of response criteria for the Psoriasis Symptoms and Signs Diary (PSSD): results from a phase 3 clinical trial. J Dermatolog Treat 2019; 30: 27–34. https://doi.org/10.1080/09546634.2017.1364694
- Pariser D, Schenkel B, Carter C, Farahi K, Brown TM, Ellis CN for the Psoriasis Patient Interview Study Group. A multicenter, non-interventional study to evaluate patient-reported experiences of living with psoriasis. J Dermatolog Treat 2016; 27: 19–26. https://doi.org/10.3109/09546634.2015.1044492
- van Ee I, Deprez E, Egeberg A, Augustin M, Conrad C, Corazza V, et al. Freedom from disease in psoriasis: a Delphi consensus definition by patients, nurses and physicians. J Eur Acad Dermatol Venereol 2022; 36: 403–412. https://doi.org/10.1111/jdv.17829
- Feldman SR, Regnier SA, Chirilov A, Hey F, Gilloteau I, Cella D. Patient-reported outcomes are important elements of psoriasis treatment decision making: a discrete choice experiment survey of dermatologists in the United States. J Am Acad Dermatol 2019; 80: 1650–1657. https://doi.org/10.1016/j.jaad.2019.01.039
- US Food and Drug Administration (FDA) guidance document for PRO Development USDoHaHSF, 2009. Available from: https://www.fda.gov/media/77832/download (last accessed May 24, 2024).
- Elewski B, Alexis AF, Lebwohl M, Stein Gold L, Pariser D, Del Rosso J, et al. Itch: an under-recognized problem in psoriasis. J Eur Acad Dermatol Venereol 2019; 33: 1465–1476. https://doi.org/10.1111/jdv.15450
- Miyagi T, Kanai Y, Murotani K, Okubo Y, Honma M, Kobayashi S, et al. Itch as a critical factor in impaired health-related quality of life in patients with plaque psoriasis achieving clear or almost-clear skin: analysis of the single-arm, open-label, multicenter, prospective ProLOGUE study. JAAD Int 2022; 8: 146–153. https://doi.org/10.1016/j.jdin.2022.06.013
- Pithadia DJ, Reynolds KA, Lee EB, Wu JJ. Psoriasis-associated itch: etiology, assessment, impact, and management. J Dermatolog Treat 2020; 31: 18–26. https://doi.org/10.1080/09546634.2019.1572865
- Lebwohl M, Yeilding N, Szapary P, Wang Y, Li S, Zhu Y, et al. Impact of weight on the efficacy and safety of ustekinumab in patients with moderate to severe psoriasis: rationale for dosing recommendations. J Am Acad Dermatol 2010; 63: 571–579. https://doi.org/10.1016/j.jaad.2009.11.012
- Blauvelt A, Armstrong AW, Langley RG, Gebauer K, Thaci D, Bagel J, et al. Efficacy of guselkumab versus secukinumab in subpopulations of patients with moderate-to-severe plaque psoriasis: results from the ECLIPSE study. J Dermatolog Treat 2022; 33: 2317–2324. https://doi.org/10.1080/09546634.2021.1959504
- Gordon KB, Blauvelt A, Foley P, Song M, Wasfi Y, Randazzo B, et al. Efficacy of guselkumab in subpopulations of patients with moderate-to-severe plaque psoriasis: a pooled analysis of the phase III VOYAGE 1 and VOYAGE 2 studies. Br J Dermatol 2018; 178: 132–139. https://doi.org/10.1111/bjd.16008
- Lebwohl MG, Merola JF, Rowland K, Miller M, Yang Y-W, Yu J, et al. Safety of guselkumab treatment for up to 5 years in patients with moderate-to-severe psoriasis: pooled analyses across seven clinical trials with greater than 8600 patient-years of exposure. Br J Dermatol 2023; 189: 42–52. https://doi.org/10.1093/bjd/ljad115
- Kimball AB, Papp KA, Wasfi Y, Chan D, Bissonnette R, Sofen H, et al. Long-term efficacy of ustekinumab in patients with moderate-to-severe psoriasis treated for up to 5 years in the PHOENIX 1 study. J Eur Acad Dermatol Venereol 2013; 27: 1535–1545. https://doi.org/10.1111/jdv.12046