ORIGINAL REPORT
Is the Use of the Extended (Meth)acrylate Series – Nails Justified? Characterization of Nail Acrylate Allergy in a Tertiary Medical Centre
Joel DASCALU1, Sophia POLANSKY1, Ziad KHAMAYSI1,2, Emily AVITAN-HERSH1,2 and Mariela J. NEVET1,2
1Department of Dermatology, Rambam Health Care Campus, Haifa, and 2The Ruth and Bruce Rappaport Faculty of Medicine, Technion – Israel Institute of Technology, Haifa, Israel
Abstract
Methacrylate allergy is a common cause of allergic contact dermatitis, and its incidence has surged over the past decade. Consequently, the primary sensitizing agent, 2-hydroxyethyl methacrylate, was recently added to the European Baseline Series of contact allergens. This study aimed to assess the added value of testing for allergens included in the (Meth)Acrylate Series – Nails, in addition to 2-hydroxyethyl methacrylate, as well as to characterize patients who may benefit from more extensive testing. A retrospective analysis of medical records of patch-tested patients was conducted between June 2013 and July 2022. Among the 3,828 patients who underwent patch testing, 396 were tested with the (Meth)Acrylate Series – Nails; 153 (38.6%) of those patients tested positive for at least 1 acrylate. The most common hapten was 2-hydroxyethyl methacrylate (85.6%), followed by hydroxypropyl methacrylate (85.0%) and ethylene glycol dimethacrylate (80.4%). In our study, 22/153 patients (14.4%) would have been missed if tested only for 2-hydroxyethyl methacrylate. The analysis showed that including hydroxypropyl methacrylate and ethylene glycol dimethacrylate improved detection rate to 98%, rendering the use of the entire tray unnecessary in most cases.
SIGNIFICANCE
Exposure to acrylate substances can trigger allergic rashes, often accompanied by cracks and intense itching. To establish a diagnosis, patients are advised to undergo a “patch test”, in which patches containing potential allergens are placed on the skin to observe allergic reactions. One substance, 2-hydroxyethyl methacrylate (2-HEMA), identified acrylate-induced allergic contact dermatitis in 85% of cases. 2-HEMA is included in the basic European Baseline tray. Testing of merely 2 other acrylic allergens identified 98% of nail-acrylate allergies in our study population. Routine implementation of this practice may minimize costs and patient discomfort, with few consequences on the patch test sensitivity.
Key words: 2-hydroxyethyl methacrylate; contact dermatitis; methacrylates.
Citation: Acta Derm Venereol 2024; 104: adv41079. DOI https://doi.org/10.2340/actadv.v104.41079.
Copyright: © 2024 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Jul 13, 2024; Accepted after revision: Oct 10, 2024; Published: Nov 12, 2024
Corr: Mariela Judith Nevet, Department of Dermatology, Rambam Health Care Campus, 2 Haalia Hashnia St., Haifa, Israel. E-mail: Y_nevet@rambam.health.gov.il.
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Acrylates and (meth)acrylates are esters or salts of acrylic acid and methacrylic acid, respectively. Monomeric acrylates and (meth)acrylates are unstable potent liquid allergens that polymerize either spontaneously at room temperature, with heat, or via UV radiation or visible light to form acrylic plastics. Acrylic polymers usually do not cause allergic contact dermatitis (ACD); nevertheless, their monomeric and dimeric forms are known contact sensitizers. Acrylates are used in various products, such as glues, coatings, inks, paints, dental prostheses, acrylic nails, mascara, and medical adhesives. The clinical presentation of allergic patients might involve dermatitis of the fingertips, hands, face – especially the eyelids – and the oral cavity (1–3).
The combination of the potent sensitization potential of acrylic monomers and their widespread exposure makes acrylates a significant aetiological factor in both occupational and non-occupational contact dermatitis. The incidence of ACD to acrylates has increased in the last decade, along with a transition towards exposure to acrylates among beauty industry consumers and employees (1, 4–6). For instance, it was estimated to comprise 2.3% of patch-tested patients across Europe during 2020–2021, showing a 3-fold rise in a timeframe of 6 years (2, 7).
Accordingly, (meth)acrylates were named contact allergen of the year by the American Contact Dermatitis Society in 2012 (8) and an acrylic compound, isobornyl acrylate, was allergen of the year for 2020 (9). Most prominently, nail acrylates have been found responsible for two-thirds of all acrylate allergies. Acrylic nails are also known as the leading cause of occupational acrylate allergy, and the risk of 2-hydroxyethyl methacrylate (2-HEMA) allergy was found to be 9 times higher among hairdressers and beauticians (2, 10). Diagnosis of acrylate ACD among beauticians has a considerable impact, with 20–50% observed to discontinue working in their profession (2, 11). Consequently, 2-HEMA was added to the European Baseline Series (EBS) of contact allergens in 2019 (12). While 2-HEMA is widely considered a reliable marker of acrylate ACD, the addition of a standardized extended acrylate series has been suggested to improve the diagnosis of acrylate allergy (1).
The potential added value of the nail acrylate series tray to acrylate ACD detection has not been established. Thus, we aimed to assess the additional benefit of testing with the (Meth)Acrylate Series – Nails (ANS; Chemotechnique Diagnostics, Vellinge, Sweden) and to identify individuals who require the addition of the extended nail acrylate series.
MATERIALS AND METHODS
This is a retrospective cohort study performed at the patch-test clinic of Rambam Medical Center, Haifa, Israel. We retrieved data from medical files of all patch-tested patients in our outpatient clinic between 1 June 2013 and 31 July 2022. A total of 3,828 patients were patch tested during this period. All procedures were approved by the Rambam Hospital Helsinki Ethics review board, protocol number 0630-21-RMB-D.
Patients with suspected acrylate ACD were concomitantly tested with both the EBS and ANS, obtained from Chemotechnique Diagnostics. Since May 2019, our clinic has implemented the newer EBS edition, which includes 2-HEMA at a concentration of 2%. Nevertheless, when acrylate allergy was suspected, patients were also subjected to ANS testing. Our analysis included only those who were both tested with the latter series and exposed to acrylates through nail products. The allergens were stored and dispensed according to the manufacturer’s instructions. Allergens were transported in airtight tubes and prepared by specialist nurses immediately prior to application.
Patch tests were applied to the upper back with Finn Chambers on Scanpor tape. The patch tests were performed with 48 h occlusion and readings were taken on D2 and D4 for all tested series. The reactions were scored as: “−”, negative; “IR”, irritant reaction; “?”, doubtful; “+”, weak; “++”, strong; “+++”, extreme, according to the recommendations of the International Contact Dermatitis Research Group (13). A positive response was considered if a weak, strong, or extreme response was noted on D4. No reaction, IR, and doubtful reaction were all considered negative responses. The following data, according to the MOAHLFA index, were retrieved from the patients’ files: gender, occupational dermatitis, atopic dermatitis, distribution of the rash (hand, leg, or facial dermatitis) and age (14).
Statistical analysis
Data were statistically analysed with StatPlus statistical package software (StatPlus Pro 7, AnalystSoft Inc, Alexandria, VA, US)A. The Mann–Whitney U test was used to compare continuous variables and the χ2 test was employed to compare categorical variables. The confidence intervals (CIs) for proportions were set at 95% and values of p < 0.05 were considered to be significant.
RESULTS
Demographics and clinical data
A total of 3,828 patients were patch tested between June 2013 and July 2022. During the 9 years of the study, 396 (10.3%) patients were suspected of having nail acrylate allergy and were therefore tested with the extended ANS. Of these 396 subjects, 153 patients (38.6%), all of whom were female, exhibited positive reactions to acrylates. The incidence of nail acrylate allergy in our patch test population was 153/3,828 (4%). Among the acrylate-sensitive patients, hand dermatitis was most prominent, displayed in 141 (91.5%) patients. The face (25/153, 16%) was also a commonly affected site, with the eyelids (11/25, 44%) often being involved. Thirty-two (20.9%) patients had involvement of more than 1 anatomical location. The characteristics of patients who tested negative or positive for acrylates were compared and are illustrated in Table I. Notably, patients testing positive for acrylates had a shorter disease duration of 1 year and 4 months (± 1.74 years), compared with those testing negative, who had a duration of 3 years (± 4.09 years) (p < 0.001).
| Factor | ANS positive (%) | ANS negative (%) | p-value |
| Male | 0 | 0 | N/A |
| Occupational dermatitis | 58.2 | 9.9 | < 0.001 |
| Atopic dermatitis | 3.9 | 8.6 | 0.07 |
| Hand involvement | 91.5 | 38.3 | < 0.001 |
| Leg involvement | 3.9 | 10.7 | < 0.05 |
| Facial involvement | 14.4 | 47.7 | < 0.001 |
| Age > 40 years | 41.8 | 44.9 | 0.554 |
| Bold values are statistically significant (p < 0.05). ANS: (Meth)Acrylate Series – Nails; N/A: not applicable. | |||
Allergens
As predicted, 2-HEMA was the most prevalent allergen, found in 3.4% of all tested patients and 85.6% of acrylate-allergic patients who were tested with the ANS. The next most frequent allergens were hydroxypropyl methacrylate (HPMA) and ethylene glycol dimethacrylate (EGDMA), which were positive in 85.0% and 80.4% of acrylate-allergic subjects, respectively.
As previously indicated, since May 2019, our outpatient clinic has utilized the updated EBS edition which includes 2-HEMA. During this period, we tested 1,591 patients, 5.8% of whom (93/1591) exhibited a positive reaction to at least 1 of the acrylates, with the detection rate of 2-HEMA reaching 96.8%. In a parallel interval from February 2017 to April 2019, 3.9% (50/752) of all tested patients had acrylate ACD (p = NS), with a significantly lower detection rate of 2-HEMA (34.0%; p < 0.0001).
We aimed to characterize the patients who would have been missed if tested only for 2-HEMA. In our study, this group comprised 22 patients (14.4%). Among them 15 patients were beauticians and 7 consumers. The most common allergens in this group were HPMA (18/22), followed by EGDMA (16/22). Table II presents a comparison between the demographic and clinical characteristics of these 22 patients and patients who tested positive for 2-HEMA as part of the ANS. The results revealed that individuals over the age of 40 were more likely to have allergy to acrylates other than 2-HEMA (p < 0.05).
| Characteristic | 2-HEMA positive (n = 131) | Nail acrylate allergy other than 2-HEMA (n = 22) | p-value |
| Male (%) | 0 (0.0) | 0 (0.0) | n/a |
| Occupational (%) | 74 (56.5) | 15 (68.1) | 0.303 |
| Atopic dermatitis (%) | 3 (2.3) | 3 (13.7) | < 0.05 |
| Hand involvement (%) | 119 (90.8) | 21 (95.5) | 0.473 |
| Leg involvement (%) | 4 (3.5) | 1 (4.5) | 0.716 |
| Facial involvement (%) | 20 (15.3) | 2 (9.1) | 0.451 |
| Age > 40 years (%) | 29 (22.1) | 10 (45.5) | < 0.05 |
| Average age (years) | 38.56 | 38.0 | 0.894 |
| Average duration of disease (years ± SD) | 1.31 (± 1.71) | 1.65 (± 1.89) | 0.589 |
| Bold values are statistically significant (p < 0.05). | |||
| ANS: (Meth) Acrylate Series – Nails; 2-HEMA: 2-Hydroxyethyl methacrylate. | |||
Occupation
We performed a subgroup comparison between beauticians (n = 113) and consumers (n = 283) who were tested with the ANS. We found that 78.8% (89/113) of the beauticians had a positive patch test to at least 1 acrylate, compared with only 22.6% (64/283) of consumers. Thus, occupational exposure to acrylates in beauty salons is a significant predictor of acrylate allergy in patients with suspected acrylate ACD, with an odds ratio of 12.7 (CI = 7.47 to 21.56, p < 0.0001; Fig. 1). The most common hapten among beauticians was HPMA (88.8%), followed by both 2-HEMA and EGDMA (83.1%). Consumers demonstrated a similar rate of 2-HEMA detection (89.1%), but with a lower prevalence of the other common allergens HPMA (79.7%) and EGDMA (76.6%), p = NS. The mean latency to diagnosis was similar among beauticians (1 year and 3 months, SD ± 1.72) and consumers (1 year and 6 months, SD ± 1.69), p = NS.
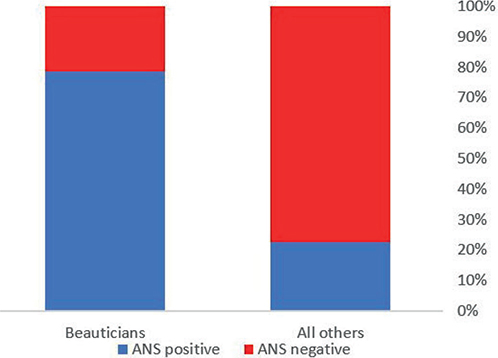
Fig. 1. Occupational exposure in beauty salon exposure renders patients more likely, at an odds ratio of 12.7 (CI = 7.47 to 21.56, p < 0.0001), to test positive for acrylate. ANS: (Meth)Acrylate Series – Nails.
DISCUSSION
The incorporation of 2-HEMA into the EBS raises a fundamental question regarding the criteria for adding the extended ANS along with the EBS. To address this question, we conducted a retrospective analysis of data from 396 patients who were tested for nail acrylate allergy at a single contact dermatitis clinic located in a large tertiary referral centre.
Our study reiterates the striking female predominance and the hands as the most frequent site of nail acrylate dermatitis (91.5%) among patients with ACD (4, 5). Age did not seem to be a risk factor for acrylate allergy, indicating that acrylate ACD can appear at any stage of life. Our data indicate a relatively short median duration from the time of initial symptoms to the time of diagnosis for patients with occupational exposure: 1 year. The data are similar to previously reported series and may be related to the severity of the cutaneous dermatitis induced by acrylates (4), as well as the high frequency of hand involvement compromising manual labour. It may also imply awareness among nail beauticians of the possible development of acrylate ACD.
In our cohort, 3.4% of all patch-tested patients were found to be positive for 2-HEMA, with a notable rise in recent years (Fig. 2). The overall incidence of 2-HEMA allergy in previously reported series throughout the last decade demonstrated a lower incidence in most of Europe, with rates ranging from 1.5% to 2.4% (1, 7, 15, 16), while some countries, such as Spain, reported a higher incidence at 4.3% (17, 18). Higher rates around 3.2% were also consistently observed in North America (19, 20). Previous data support a high prevalence of acrylate allergy in Israel, with studies reporting rates ranging from above 5% to over 8% (21, 22). The high incidence rate in our population might be explained by several factors, including high popularity of acrylate-containing nail polish, improper use of protective measures as well as heightened awareness among both physicians and beauticians. Moreover, the steady worldwide increase in the incidence of acrylate allergy has been widely reported (6, 15, 23, 24). Previous studies have shown that the 2-HEMA patch test is highly effective in identifying acrylate ACD, being able to detect approximately 85–93% of patients with acrylate allergy (2, 4, 21). However, some studies have reported lower detection rates ranging from 63% to 73% (1, 25). Consistent with these findings, our cohort revealed that 2-HEMA was the most prevalent allergen, identifying 131 (85.6%) of the 153 patients with acrylate ACD. The other 2 most prevalent allergens were HPMA and EGDMA, both recognized for their tendency to cross-react with 2-HEMA (26).

Fig. 2. Annual incidence of 2-hydroxyethyl methacrylate allergy among patients tested with the (Meth)Acrylate Series – Nails.
We attempted to characterize the 22 patients who displayed an allergic reaction to acrylates but tested negative for 2-HEMA. 2-HEMA-negative acrylate ACD patients in our cohort were more likely to be over 40 and had a higher prevalence of atopy than HEMA-positive patients, consistent with previous reports linking age over 30 to 2-HEMA negativity (18, 22). These findings suggest a potential necessity for more extensive testing in these individuals.
Next, we sought to pinpoint the allergens that would allow us to identify acrylate ACD accurately without subjecting patients to the complete ANS testing protocol. Of the patients with acrylate ACD who were not diagnosed by 2-HEMA, the 2 most common allergens were HPMA and EGDMA. Our results suggest that adding HPMA and EGDMA to 2-HEMA allows diagnosis of 98.0% of all acrylate ACD patients. Similarly, a previous study in Italy also showed EGDMA as a common allergen among acrylate ACD patients who tested negative for 2-HEMA (15). Hence, in practice, a more selective testing approach might be considered for patients suspected of nail acrylate allergy. This approach would offer lower costs and minimize the discomfort of additional patches, as acrylates are known to cause persistent and intense vesicular reactions (8, 15, 16, 26). However, further research is warranted to investigate the potential utility of using the entire tray for patients with certain less common exposures, such as orthopaedic surgeries and industrial workers.
Occupational exposure as an aetiology of acrylate ACD was found in 89/153 (58.2%) of allergic patients, in line with a rate of 57% previously reported by a large European series (2). Beauticians had a high ratio of positive reactions to acrylates: 89 out of 113 (78.8%) were positive for at least 1 hapten. The usage of home kits and non-professional UV-curing nail polish further enhances the risk of developing acrylate sensitization (1, 27–29). This highlights the need to consider more effective preventive measures. For instance, in November 2020, the EU Cosmetic Regulations restricted the use of 2-HEMA for nail cosmetics to professional use only (EC 1223/2009). Moreover, in the USA, recent legislation has been enacted in the form of the Modernization of Cosmetics Regulation Act of 2022 (MoCRA) regarding the regulation of personal care products by the Food and Drug Administration (FDA) (30). In Israel, however, these regulations have not yet been adopted. Given the limited efficacy of gloves as a preventive measure and the low compliance rate, alternative preventive measures with better efficacy should be considered (16, 31–34).
Our study’s limitations include its retrospective design and usage of data files. Additionally, studies show mixed data regarding delayed reactions. While some studies report that up to 16% of patients exhibit delayed reactions to patch testing, with positive reactions only appearing on D7 or later, others have found no delayed reactions at all (15, 35). Therefore, without an additional delayed reading, there is a potential for underestimation of the proportion of positive tests for nail acrylate allergens.
In conclusion, testing for 2-HEMA as part of the present EBS can detect about 85–90% of patients affected by nail acrylate ACD. The additional testing of HPMA, EGDMA, or both, can further enhance diagnostic accuracy to 98%. Consequently, while our findings require further validation through additional studies in diverse cohorts, we propose that the additive value of the entire extended ANS is limited, even when occupational nail-acrylate allergy is suspected. Moreover, the increased prevalence of nail acrylate allergy and the high positivity rate among employees in the beauty industry warrant stricter regulations and the consideration of preventive measures to minimize occupational acrylate allergy.
ACKNOWLEDGEMENTS
IRB approval status: The study was approved by the local IRB committee, protocol number 0630-21-RMB-D.
REFERENCES
- Rolls S, Chowdhury MM, Cooper S, Cousen P, Flynn AM, Ghaffar SA, et al. Recommendation to include hydroxyethyl (meth)acrylate in the British baseline patch test series. Br J Dermatol 2019; 181: 811–817. https://doi.org/10.1111/bjd.17708
- Gonçalo M, Pinho A, Agner T, Andersen KE, Bruze M, Diepgen T, et al. Allergic contact dermatitis caused by nail acrylates in Europe: an EECDRG study. Contact Dermatitis 2018; 78: 254–260. https://doi.org/10.1111/cod.12942
- Forkel S, Schubert S, Corvin L, Heine G, Lang CC V, Oppel E, et al. Contact allergies to dental materials in patients. Br J Dermatol 2024; 190: 895–903. https://doi.org/10.1093/bjd/ljad525
- Raposo I, Lobo I, Amaro C, Lobo M de L, Melo H, Parente J, et al. Allergic contact dermatitis caused by (meth)acrylates in nail cosmetic products in users and nail technicians: a 5-year study. Contact Dermatitis 2017; 77: 356–359. https://doi.org/10.1111/cod.12817
- Gregoriou S, Tagka A, Velissariou E, Tsimpidakis A, Hatzidimitriou E, Platsidaki E, et al. The rising incidence of allergic contact dermatitis to acrylates. Dermatitis 2020; 31: 140–143. https://doi.org/10.1097/DER.0000000000000528
- Montgomery R, Stocks SJ, Wilkinson SM. Contact allergy resulting from the use of acrylate nails is increasing in both users and those who are occupationally exposed. Contact Dermatitis 2016; 74: 120–122. https://doi.org/10.1111/cod.12497
- Uter W, Wilkinson SM, Aerts O, Bauer A, Borrego L, Brans R, et al. Patch test results with the European baseline series, 2019/20: joint European results of the ESSCA and the EBS working groups of ESCD and the GEIDAC. Contact Dermatitis 2022; 87: 343–355. https://doi.org/10.1111/cod.14170
- Sasseville D. Acrylates in contact dermatitis. Dermatitis 2012; 23: 6–16. https://doi.org/10.1097/DER.0b013e31823d1b81
- Aerts O, Herman A, Mowitz M, Bruze M, Goossens A. Isobornyl acrylate. Dermatitis 2020; 31: 4–12. https://doi.org/10.1097/DER.0000000000000549
- Symanzik C, Weinert P, Babić Ž, Hallmann S, Havmose MS, Johansen JD, et al. Allergic contact dermatitis caused by 2-hydroxyethyl methacrylate and ethyl cyanoacrylate contained in cosmetic glues among hairdressers and beauticians who perform nail treatments and eyelash extension as well as hair extension applications: a systematic review. Contact Dermatitis 2022; 86: 480–492. https://doi.org/10.1111/cod.14056
- Gatica-Ortega ME, Rodríguez-Lago L, Beneyto P, Pastor-Nieto MA, Borrego L. Prognosis and sequelae of meth(acrylate) sensitization in beauticians and consumers of manicure materials. Contact Dermatitis 2023; 89: 471–479. https://doi.org/10.1111/cod.14408
- Wilkinson M, Gonçalo M, Aerts O, Badulici S, Bennike NH, Bruynzeel D, et al. The European baseline series and recommended additions: 2019. Contact Dermatitis 2019; 80: 1–4. https://doi.org/10.1111/cod.13155
- Fregert S. Manual of contact dermatitis. 2nd ed. Copenhagen: Munksgaard; 1980.
- Schnuch A, Geier J, Uter W, Frosch PJ, Lehmacher W, Aberer W, et al. National rates and regional differences in sensitization to allergens of the standard series: population-adjusted frequencies of sensitization (PAFS) in 40,000 patients from a multicenter study (IVDK). Contact Dermatitis 1997; 37: 200–209. https://doi.org/10.1111/j.1600-0536.1997.tb02435.x
- Stingeni L, Tramontana M, Bianchi L, Foti C, Patruno C, Gallo R, et al. Contact sensitivity to 2-hydroxyethyl methacrylate in consecutive patients: a 1-year multicentre SIDAPA study. Contact Dermatitis 2019; 81: 216–218. https://doi.org/10.1111/cod.13278
- Havmose M, Thyssen JP, Zachariae C, Johansen JD. Contact allergy to 2-hydroxyethyl methacrylate in Denmark. Contact Dermatitis 2020; 82: 229–231. https://doi.org/10.1111/cod.13439
- Hernández-Fernández CP, Mercader-García P, Silvestre Salvador JF, Sánchez Pérez J, Fernández Redondo V, Miquel Miquel FJ, et al. Candidate allergens for inclusion in the Spanish standard series based on data from the Spanish contact dermatitis registry. Actas Dermosifiliogr 2021; 112: 798–805. https://doi.org/10.1016/j.ad.2021.05.005
- Gatica-Ortega ME, Pastor-Nieto MA, Giménez-Arnau AM, Mercader-García P, Sanz-Sánchez T, Carrascosa-Carrillo JM, et al. 2-Hydroxyethyl methacrylate (2-HEMA) sensitization, a global epidemic at its peak in Spain? Contact Dermatitis 2024; 90: 507–513. https://doi.org/10.1111/cod.14520
- DeKoven JG, Warshaw EM, Reeder MJ, Atwater AR, Silverberg JI, Belsito DV, et al. North American Contact Dermatitis Group Patch Test Results: 2019–2020. Dermatitis 2023; 34: 90–104. https://doi.org/10.1089/derm.2022.29017.jdk
- DeKoven JG, Warshaw EM, Zug KA, Maibach HI, Belsito DV, Sasseville D, et al. North American Contact Dermatitis Group Patch Test Results: 2015–2016. Dermatitis 2018; 29: 297–309. https://doi.org/10.1097/DER.0000000000000417
- Slodownik D, Kaplan Y, Sprecher E, Daniely D. The added value of patch testing beyond the baseline tray. Dermatitis 2022; 33: 227–231. https://doi.org/10.1097/DER.0000000000000889
- Hilewitz D, Trattner A, Reiter O, Uvaidov V, Noyman Y, Solomon Cohen E, et al. Pandemic of sensitivity to acrylate containing nail cosmetic among young Israeli women? Result of patch testing 2-hydroxyethyl methacrylate in the European baseline series. Contact Dermatitis 2024 Aug 24 [Online ahead of print]. https://doi.org/10.1111/cod.14683
- Uter W, Werfel T, Lepoittevin JP, White IR. Contact allergy: emerging allergens and public health impact. Int J Environ Res Public Health 2020; 17: 2404. https://doi.org/10.3390/ijerph17072404
- Steunebrink IM, de Groot A, Rustemeyer T. Contact allergy to acrylate-containing nail cosmetics: a retrospective 8-year study. Contact Dermatitis 2024; 90: 262–265. https://doi.org/10.1111/cod.14475
- Fisch A, Hamnerius N, Isaksson M. Dermatitis and occupational (meth)acrylate contact allergy in nail technicians: a 10-year study. Contact Dermatitis 2019; 81: 58–60. https://doi.org/10.1111/cod.13216
- De Groot AC, Rustemeyer T. 2-Hydroxyethyl methacrylate (HEMA): a clinical review of contact allergy and allergic contact dermatitis. Part 2. Cross- and co-sensitization, other skin reactions to HEMA, position of HEMA among (meth)acrylates, sensitivity as screening agent, presence of HEMA in commercial products and practical information on patch test procedures. Contact Dermatitis 2024; 90: 1–16. https://doi.org/10.1111/cod.14430
- Tramontana M, Hansel K, Bianchi L, Marietti R, Stingeni L. Use of self-applied sculptured gel nails may increase the risk of allergy to (meth)acrylates in children and adolescents. J Eur Acad Dermatol Venereol 2021; 35: e765–e767. https://doi.org/10.1111/jdv.17429
- Gatica-Ortega ME, Pastor-Nieto MA, Gil-Redondo R, Martínez-Lorenzo ER, Schöendorff-Ortega C. Non-occupational allergic contact dermatitis caused by long-lasting nail polish kits for home use: ‘the tip of the iceberg’. Contact Dermatitis 2018; 78: 261–265. https://doi.org/10.1111/cod.12948
- Roy F, Besner Morin C. Pseudo-psoriatic nails caused by at-home gel manicure. J Cutan Med Surg 2023; 27: 169–170. https://doi.org/10.1177/12034754231159593
- Filley AR, Woodruff CM. The modernization of cosmetics regulation act of 2022: what dermatologists need to know. J Am Acad Dermatol 2023; 89: 629–631. https://doi.org/10.1016/j.jaad.2023.04.024
- Morgado F, Batista M, Gonçalo M. Short exposures and glove protection against (meth)acrylates in nail beauticians: thoughts on a rising concern. Contact Dermatitis 2019; 81: 62–63. https://doi.org/10.1111/cod.13222
- Fremlin G, Sansom J. Acrylate-induced allergic contact dermatitis in a car windscreen repairer. Occup Med (Chic Ill) 2014; 64: 557–558. https://doi.org/10.1093/occmed/kqu095
- Ursberg AM, Bergendorff O, Thorsson AC, Isaksson M. Is there a good in vivo method to show whether gloves are sufficiently protective when a nail technician is exposed to (meth)acrylates? An in vivo pilot study. Contact Dermatitis 2016; 75: 62–65. https://doi.org/10.1111/cod.12573
- Havmose M, Thyssen JP, Zachariae C, Johansen JD. Artificial nails and long-lasting nail polish in Danish hairdressers: self-use, occupational exposure and related eczema. Acta Derm Venereol 2022; 102: adv00818. https://doi.org/10.2340/actadv.v102.4524
- Cantwell HM, Drage LA, el-Azhary RA, Hall MR, Killian JM, Yiannias JA, et al. The final patch test read: day 5 or day >7? Dermatitis 2020; 31: 42–52. https://doi.org/10.1097/DER.0000000000000562