ORIGINAL REPORT
Effect of Betablockers on the Course of Martorell Hypertensive Ulcers: A Retrospective Study
Lucy CLEUSIX#, Olesya PAVLOVA#, Emmanuella GUENOVA and François KUONEN
Department of Dermatology and Venereology, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland
#These authors contributed equally.
Martorell hypertensive ulcer (MHU) represents a painful, difficult-to-handle condition associated with peripheral, subcutaneous arteriolosclerosis caused by chronic hypertensive disease. Betablockers are effective for and widely used to treat hypertensive disease but are reported to exacerbate peripheral vasoconstriction. The effect of betablockers on pre-existing arteriolosclerosis and the course of MHU is, however, unknown. A retrospective study to assess the effect of betablockers on the course and response to treatment of MHU was conducted. Clinical and histopathological data were collected of patients treated for MHU at the authors’ institution between 2014 and 2023 and a side-by-side comparison was performed of patients taking betablockers or not. Analysis focused on MHU severity at presentation, analgesic use, response to therapeutic intervention, and alterations of cutaneous arterioles. The study reports significantly larger ulcers and more frequent use of opioids in patients taking betablockers, while no significant difference was observed in terms of MHU response to treatment. Significantly increased luminal obstruction of peripheral cutaneous arterioles was found in patients taking beta-blockers. Based on these data, betablockers may have a negative effect on the course of MHU and should be carefully assessed in patients with MHU.
SIGNIFICANCE
Martorell hypertensive ulcers represent serious, difficult-to-treat comorbidity associated with long-term uncontrolled arterial hypertension. Beta-blockers are effective for and largely used to treat hypertensive disease but have been reported to induce peripheral vasoconstriction. This study provides additional information concerning beta-blockers’ effect in the pathogenesis of Martorell hypertensive ulcers. Our results suggest that beta-blockers maybe non-optimal treatment choice for patients with already developed Martorell hypertensive ulcers.
Key words: ulcers; vascular disorders; hypertension; Martorell; treatment.
Citation: Acta Derm Venereol 2024; 104: adv41087. DOI https://doi.org/10.2340/actadv.v104.41087.
Copyright: © 2024 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Jun 28, 2024; Accepted after revision: Oct 15, 2024; Published: Nov 7, 2024
Corr: François Kuonen, MD, PhD, Department of Dermatology and Venereology, Lausanne University Hospital and University of Lausanne, Av. de Beaumont 29, CH-1011 Lausanne, Switzerland. Email: Francois.Kuonen@chuv.ch
Competing interests and funding: The authors have no conflicts of interests to declare.
INTRODUCTION
Martorell hypertensive ulcers (MHU) are painful, difficult-to-treat ulcers representing a potentially serious complication of long-term uncontrolled arterial hypertension (1–4). They are commonly seen in women with a reported age range between 50 and 70 years (4, 5). The principal pathophysiological hallmark includes ischaemic arteriolosclerosis, resulting from narrowing small skin blood vessels, most commonly arterioles, that cannot dilate to increase the blood supply (2, 6). This leads to increased resistance to blood flow, a lack of blood delivery, skin necrosis, and death (2–4, 7–9), triggering extremely painful ulceration typically located in the distal part of the lower limb (5, 6, 10–12). While evolution may be favourable upon rapid debridement and skin grafting, many patients show fast progression, severe pain, and early relapse (5, 13). The successful treatment of MHU is thus challenging, requiring adequate pain management, antihypertensive therapy, topical treatment, and surgery (14, 15).
Beta-blockers are largely used to treat hypertensive disease (16, 17). However, depending on their intrinsic pharmacological properties, they may induce peripheral vasoconstriction (16, 18–20). Although betablockers should be used with precaution in patients with peripheral vascular disease and Raynaud’s phenomenon, their effect on the progression/course of MHU is still unknown.
Here, we present a retrospective study comparing side-by-side patients with MHU regarding severity, response to treatment and histological alterations depending on beta-blocker intake.
MATERIAL AND METHODS
Setting
The procedure followed was in accordance with the Helsinki Declaration of 1975, as revised in 1983 and approved by the institutional review board of Lausanne University Hospital CHUV and the local ethics committee (study 2021-01592). Each patient provided written informed consent. Patients were identified in the internal database using the search terms “necrotic angiodermatitis”, “necrotizing angiodermatitis”, “Martorell’s ulcer”, “hypertensive ulcer”, and “arteriosclerotic ulcer”. The inclusion criteria were age > 18 years and confirmed clinical and histopathological diagnosis of MHU. The exclusion criteria comprised uncertain diagnosis, incomplete clinical and/or histological documentation, and age < 18 years. Collected clinical data comprised gender, age, medication at the time of referral, comorbidities, cardiovascular risk factors, lower legs venous history, hospitalization need, painkiller medication use, ulcer features (first episode/relapse, localization, size at the time of referral, treatment type, and evolution), and skin arterioles characteristics.
Study design and statistical analysis
The analysis focused on 29 patients selected for eligibility from 69 patients. Forty patients were excluded due to either lack of consent/incomplete or clinical-histopathological documentation (Fig. 1). The age ranged from 49 to 94 years, with a mean of 79. The male-to-female ratio was 0.61. The cohort was divided into the beta-blocker group (BB group, n = 11; β1-selective, nebivolol n = 2, metoprolol n = 6, and atenolol n = 2; non-selective, carvedilol n = 1) or non-beta-blocker group (NBB group, n = 18) according to their medication at the time of referral. The main evaluation criteria were the severity of MHU, assessed by the ulcerated area, required pain medication, therapeutic intervention type, clinical evolution, and cutaneous arteriolosclerosis. P-values were calculated using a z-score for 2 population proportions and Student’s t-test for quantitative variables. The statistical analyses were performed using GraphPad Prism® version 9.5.1 (https://www.graphpad.com).
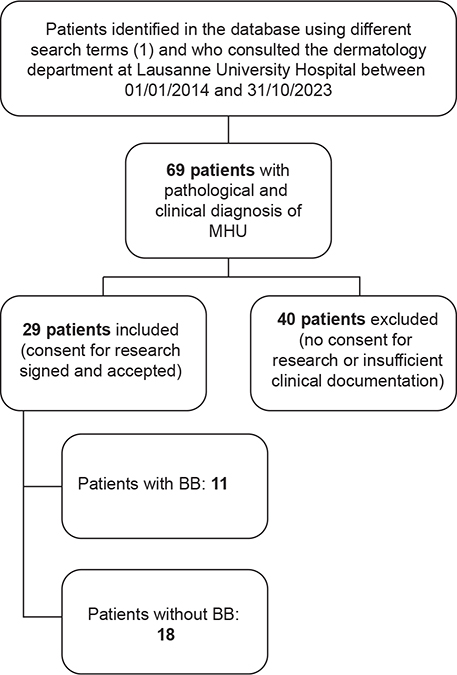
Fig. 1. Study flowchart. MHU: Martorell hypertensive ulcer; BB: betablockers. NBB: non-betablockers (1) search terms: “necrotic angiodermitis”, “necrotizing angiodermitis”, “Martorell’s ulcer”, “hypertensive ulcer”, and “arteriosclerotic ulcer”.
Histological analysis
Skin biopsies from ulcers were performed for diagnostic purposes, according to previous recommendations on biopsies in patients with MHU (5). All histological specimens were initially stained with haematoxylin and eosin (H&E) according to standard protocols (21). We defined arteriole or precapillary artery as a blood vessel measuring 25 to 110 μm in diameter with a media of 2–3 muscle cells in thickness (1, 22) (Fig. 2A, B). We then evaluated the arterioles at the dermal-subcutaneous junction based on previously published MHU vascular histological criteria (9). Arteriolosclerosis was assessed by measuring the wall-to-lumen ratio (WLR) according to the previously described methods (1, 9) (Fig. 2C). A minimum of 3 arterioles at the dermal–subcutaneous junction were measured for each patient. We used the tunica media’s outermost cells to define the vessel’s external diameter.
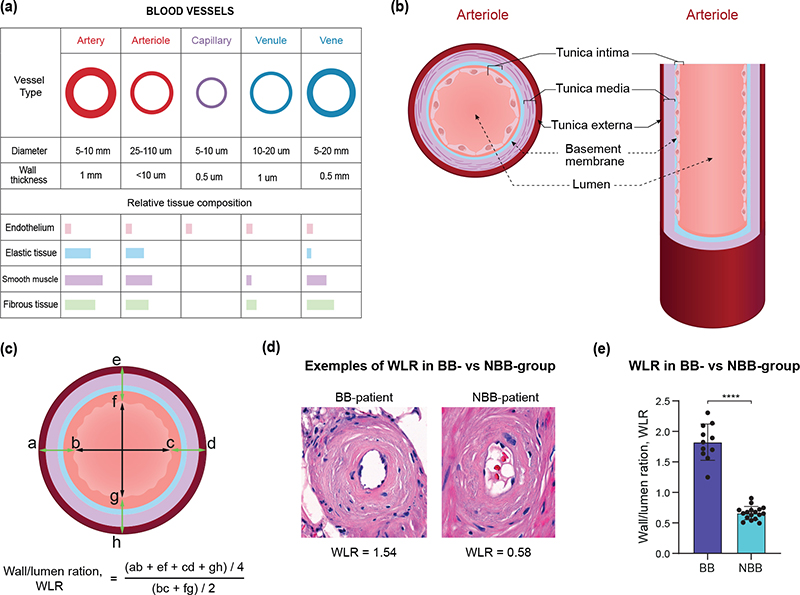
Fig. 2. Assessment of arteriolar wall-to-lumen ratio. (A) Graphic representation of relative size and structure of different vessels in the skin. (B) Schematic presentation of arteriolar anatomy. (C) Quantification of arteriolar wall/lumen ratio (WLR) showing the formula used (bottom). The diameter of the wall is obtained by dividing the summation of a–b, c–d, e–f, g–h by 4. The diameter of the lumen is obtained by dividing the summation of b–c and f–g by 2. (D) Examples and WLR in BB and NBB groups. (E) WLR calculated in the study groups (BB group, n = 11; NBB group, n = 18). All graphs show the average of 3 independent measurements. Error bars represent standard error of the mean (SEM). ****p < 0.0001.
RESULTS
Demographic characteristics of the study population
BB and NBB groups were similar in terms of age (NBB = 78.9 ± 11.1, BB = 80 ± 9.5, p-value 0.77) and male/female sex ratio (NBB = 0.63, BB = 0.57, p-value = 0.99) (Table I). Cardiovascular risk factors were evenly distributed in NBB and BB groups, with arterial hypertension stated in all patients (29 patients including both NBB and BB, 100%), active smoking in 24.1% of patients (NBB = 16.7%, BB = 36.4%, p = 0.23), dyslipidaemia reported in 37.9% of patients (NBB = 50%, BB = 18.2%, p = 0.09) and type 2 diabetes, obesity, and peripheral arterial disease documented in 24.1% of patients (NBB = 27.8%, BB = 18.2%, p = 0.56) (Table I). Chronic venous insufficiency (NBB = 27.8%, BB = 45.4%; p = 0.33) and history of deep or superficial thrombosis (NBB = 5.6%, BB = 27.3%; p = 0.099) were also equally distributed in both groups (Table I).
Betablockers and severity of MHU
We first assessed the association between beta-blocker therapy and the severity of MHU by clinical presentation at the time of referral. Both the BB and NBB groups presented MHU mostly as a first episode (NBB = 83.3%, BB = 81.8%; p = 0.92; Table II). Most patients were eligible for hospitalization rather than ambulatory follow-up, regardless of beta-blocker treatment (NBB = 66.7%, BB = 81.8%, p = 0.37; Table II). However, the BB group displayed significantly larger ulcers compared with the NBB group (NBB = 26.3 cm2 ± 22.7, BB = 44.5cm2 ± 31.1, p = 0.043; Table II).
Betablockers and pain control
Next, we analysed the association between betablocker therapy and the intensity of MHU using prescribed pain medication during follow-up as a surrogate marker. As expected, most patients received paracetamol in both groups (NBB = 55.6%, BB = 54.5%, p = 0.96; Table II). Metamizole was rarely prescribed (NBB = 5.6%, BB = 9.1%; p = 0.71; Table II). However, BB and NBB groups differed significantly regarding opioid prescription, with most BB patients requiring opioid-based pain control compared with the NBB group (NBB = 5.6%, BB = 63.6%, p = 0.0006; Table II).
Betablockers and therapy response
We further assessed the potential association between betablocker treatment and MHU response to therapy. Importantly, BB and NBB groups did not differ in terms of therapeutic strategy, with most patients eligible for debridement/necrosectomy and autologous split-thickness skin graft (NBB = 72.2%, BB = 72.7%, p = 0.98; Table II). Response to treatment was assessed 6 months after debridement/necrosectomy and autologous split-thickness skin graft. Overall, incomplete response and relapse rates did not differ between the 2 groups (NBB = 53.8%, BB = 37.5%; p = 0.46; Table II).
Assessment of luminal obstruction
Both larger ulcer size and increased prescription of opioids in the BB group suggested that betablockers may act on MHU pathogenesis. We thus investigated histological alterations found in arterioles of BB and NBB groups. Meticulous analysis confirmed structural changes associated with MHU in both groups, including endothelial hyperplasia, proliferation and thickening of the inner elastic lamina, nuclear hyperplasia of tunica media, reduction of lumen size, occasional thrombotic occlusion, and different degrees of periarteriolar fibrosis. To best assess the severity of luminal obstruction, we then calculated the ratio between the thickness of the arterial wall and the lumen (wall-to-lumen ratio, WLR), according to a previously described protocol (9) (Fig. 2C). Remarkably, we found significantly increased WLR in the BB compared with the NBB group (NBB = 0.66 ± 0.11; BB = 1.82 ± 0.38; p < 0.0001; Fig. 2D–E). Increased WLR in the BB group reflected both thicker arteriolar walls and smaller lumens (Fig. 3).

Fig. 3. Assessment of the lumen’s diameters and a wall thickness in BB and NBB groups. (A) Schematic representation of wall thickness and lumens diameter of arterioles in BB and NBB groups. (B) Lumen’s diameters and (C) wall thickness in BB versus NBB group (BB group, n = 11; NBB group, n = 18). All graphs show the average of 3 independent measurements. Error bars represent standard error of the mean (SEM). **p < 0.01.
DISCUSSION
Our study finds a significant association between beta-blocker treatment and the severity of the MHU course. We report significantly larger ulcers, increased opioid-based pain control, and more severe arteriolar luminal obstruction measured by arterial WLR in patients taking betablockers.
MHU ulcers result from ischaemic necrosis. Ulcer size consequently reflects ischaemic damage, while excruciating pain associated with MHU reflects ischaemic pain. The double observation of larger ulcers and increased opioid take in the BB group strongly suggest that betablockers may have a critical, negative effect in the pathogenesis of MHU. Consistently, we found significantly reduced arteriolar lumens in the periphery of MHU in the BB group, thus explaining reduced skin perfusion and increased ischaemic consequences, such as cellular damage, cell death, and stronger activating pain signals in the affected area.
The effect of beta-blockers on skin microcirculation remains controversial. While beta-blockers have long been known to cause peripheral vasoconstriction (17, 19, 23), recent studies fail to detect significant effect (24, 25). This may be partly due to the fact that beta-blockers represent a heterogeneous group of antihypertensive drugs with distinct pharmacological properties, resulting in varying effects on skin microcirculation. Indeed, a recent, broad meta-analysis reported differing degrees of vasoconstrictive effects among individual beta-blockers, largely influenced by their intrinsic sympathomimetic activity or vasodilatory properties, rather than β1-selectivity (19). While this highlights the absence of a uniform class effect, it suggests that beta-blockers with intrinsic sympathomimetic activity may be preferable for patients with peripheral vascular diseases (19). Notably, our study included 4 beta-blockers lacking intrinsic sympathomimetic activity, which may account for the observed effects on MHU disease.
In practice, hypertension and pain management are the foremost priorities in the treatment of patients with MHU. Opioid use should be reduced to avoid the risk of dependence. Our study supports that switching from beta-blockers to alternative anti-hypertensive therapy e.g., calcium channel blockers and angiotensin-converting enzyme inhibitors) would prevent larger ulceration, reduce pain, and diminish opiate consumption in patients with MHU.
Study limitations
This study has several limitations. One of them is the retrospective character of the study. The clinical cases were collected in 1 institution from patients seen in our department between 2014 and 2023. This long study period, due to the rather limited incidence of Martorell’s disease, may have caused the heterogeneity of the study population, particularly regarding therapeutic measures and the use of different antihypertensive drugs, which have changed over the years. Also, several patients had to be excluded from the study due to the lack of consent or incomplete clinical-histopathological documentation. This selection procedure also represents a bias regarding extrapolation of the results to a non-selective patient population in daily clinical practice. Finally, although cardiovascular risk factors and venous history are similarly distributed between BB and NBB patients (see Table I), we cannot rule out differences in severity, which may contribute to the observed variations in ulcer size and/or opioid requirements.
Conclusion
This study provides insights into the relationship between betablocker use and the severity of MHU. Based on our data, betablockers may have a negative effect on the course of MHU and should be carefully assessed in patients with MHU. Further studies are needed to assess the exact mechanism of this phenomenon and the respective effects related to beta-blockers with distinct pharmacological properties. Importantly, our results suggest that, when possible, beta-blockers should be switched in favour of alternative antihypertensive strategies in patients suffering from MHU.
ACKNOWLEDGEMENTS
Ethics statement: All patients gave written informed consent to publish their case details.
Data availability statement: The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- Farber EM, Hines EA, Jr., Montgomery H, McK Craig W. The arterioles of the skin in essential hypertension. J Invest Dermatol 1947; 9: 285–298. https://doi.org/10.1038/jid.1947.101
- Vuerstaek JD, Reeder SW, Henquet CJ, Neumann HA. Arteriolosclerotic ulcer of Martorell. J Eur Acad Dermatol Venereol 2010; 24: 867–874. https://doi.org/10.1111/j.1468-3083.2009.03553.x
- Alavi A, Mayer D, Hafner J, Sibbald RG. Martorell hypertensive ischemic leg ulcer: an underdiagnosed Entity. Adv Skin Wound Care 2012; 25: 563–572. https://doi.org/10.1097/01.ASW.0000423442.08531.fb
- Martorell F. Hypertensive ulcer of the leg. J Cardiovasc Surg 1978; 19: 599–600.
- Hafner J, Nobbe S, Partsch H, Läuchli S, Mayer D, Amann-Vesti B, et al. Martorell hypertensive ischemic leg ulcer: a model of ischemic subcutaneous arteriolosclerosis. Arch Dermatol 2010; 146: 961–968. https://doi.org/10.1001/archdermatol.2010.224
- Reeder SW, Middelburg TA, Neumann HA. An extremely painful ulcer on the lower leg; Martorell arteriolosclerotic ulcer. Ned Tijdschr Geneeskd 2009; 153: B421.
- Woolling KR. Hypertensive-ischemic ulcer. An atypical ischemic necrosis of the skin. Jama 1964; 187: 196–201. https://doi.org/10.1001/jama.1964.03060160024006
- Duncan HJ, Faris IB. Martorell’s hypertensive ischemic leg ulcers are secondary to an increase in the local vascular resistance. J Vasc Surg 1985; 2: 581–584. https://doi.org/10.1016/0741-5214(85)90013-8
- Deinsberger J, Brugger J, Tschandl P, Meier-Schiesser B, Anzengruber F, Bossart S, et al. Differentiating Arteriolosclerotic Ulcers of Martorell from Other Types of Leg Ulcers Based on Vascular Histomorphology. Acta Derm Venereol 2021; 101: adv00449. https://doi.org/10.2340/00015555-3804
- Deinsberger J, Moschitz I, Marquart E, Manz-Varga AK, Gschwandtner ME, Brugger J, et al. Development of a localization-based algorithm for the prediction of leg ulcer etiology. J Dtsch Dermatol Ges 2023; 21: 1339–1349. https://doi.org/10.1111/ddg.15192
- Romanelli MR, Thayer JA, Neumeister MW. Ischemic Pain. Clin Plast Surg 2020; 47: 261–265. https://doi.org/10.1016/j.cps.2019.11.002
- Weber B, Deinsberger J, Hafner J, Beltraminelli H, Tzaneva S, Böhler K. Localization-mapping of arteriolosclerotic ulcers of Martorell using two-dimensional computational rendering reveals a predominant location on the mid-lateral lower leg. J Eur Acad Dermatol Venereol 2021; 35: e40–e42. https://doi.org/10.1111/jdv.16787
- Choucair MM, Fivenson DP. Leg ulcer diagnosis and management. Dermatol Clin 2001; 19: 659–678. https://doi.org/10.1016/S0733-8635(05)70307-7
- Csuka EA, Ward SC, Ekelem C, Csuka DA, Ardigò M, Mesinkovska NA. Reflectance Confocal Microscopy, Optical Coherence Tomography, and Multiphoton Microscopy in Inflammatory Skin Disease Diagnosis. Lasers in Surgery and Medicine 2021; 53: 776–797. https://doi.org/10.1002/lsm.23386
- Malhi HK, Didan A, Ponosh S, Kumarasinghe SP. Painful Leg Ulceration in a Poorly Controlled Hypertensive Patient: A Case Report of Martorell Ulcer. Case Rep Dermatol 2017; 9: 95–102. https://doi.org/10.1159/000468977
- Herrick AL. The pathogenesis, diagnosis and treatment of Raynaud phenomenon. Nat Rev Rheumatol 2012; 8: 469–479. https://doi.org/10.1038/nrrheum.2012.96
- Lacourcière Y, Lefebvre J, Provencher P, Poirier L. Comparison of quinapril and atenolol as single drugs or in combination with hydrochlorothiazide in moderate to severe hypertensives, using automated ambulatory monitoring. Br J Clin Pharmacol 1993; 35: 121–127. https://doi.org/10.1111/j.1365-2125.1993.tb05677.x
- Brand FN, Larson MG, Kannel WB, McGuirk JM. The occurrence of Raynaud’s phenomenon in a general population: the Framingham Study. Vasc Med 1997; 2: 296–301. https://doi.org/10.1177/1358863X9700200404
- Khouri C, Jouve T, Blaise S, Carpentier P, Cracowski JL, Roustit M. Peripheral vasoconstriction induced by β-adrenoceptor blockers: a systematic review and a network meta-analysis. Br J Clin Pharmacol 2016; 82: 549–560. https://doi.org/10.1111/bcp.12980
- Marshall AJ, Roberts CJ, Barritt DW. Raynaud’s phenomenon as side effect of beta-blockers in hypertension. Br Med J 1976; 1: 1498–1499. https://doi.org/10.1136/bmj.1.6024.1498
- Feldman AT, Wolfe D. Tissue processing and hematoxylin and eosin staining. Methods Mol Biol 2014; 1180: 31–43. https://doi.org/10.1007/978-1-4939-1050-2_3
- Tu T-Y, Chao PC-P. Continuous blood pressure measurement based on a neural network scheme applied with a cuffless sensor. Microsyst Technol 2018; 24: 4539–4549. https://doi.org/10.1007/s00542-018-3957-4
- Yang A, Yu G, Wu Y, Wang H. Role of β2-adrenergic receptors in chronic obstructive pulmonary disease. Life Sci 2021; 265: 118864. https://doi.org/10.1016/j.lfs.2020.118864
- Ubbink DT, Verhaar EE, Lie HK, Legemate DA. Effect of beta-blockers on peripheral skin microcirculation in hypertension and peripheral vascular disease. J Vasc Surg 2003; 38: 535–540. https://doi.org/10.1016/S0741-5214(03)00419-1
- Paravastu SC, Mendonca DA, Da Silva A. Bêta-bloquants pour la maladie artérielle périphérique. Cochrane Database Syst Rev 2013; 2013: CD005508. https://doi.org/10.1002/14651858.CD005508.pub3