SHORT COMMUNICATION
Diffuse Pain Revealing Clinically Unapparent Subcutaneous Sarcoidosis
Marien CHIARA1 and Prochore KAMGANG SEMEU1,2*
1Department of Internal Medicine, Brugmann University Hospital, Building K, Gate K1. 4, Avenue A Van Gehuchten, BE-1020 Brussels and 2Faculty of Medicine, Université Libre de Bruxelles, Brussels, Belgium. *E-mail: Prochore.kamgang@chu-brugmann.be
Citation: Acta Derm Venereol 2024; 104: adv41137. DOI: https://doi.org/10.2340/actadv.v104.41137.
Copyright: © 2024 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Jul 7, 2024. Accepted: Jul 29, 2024. Published: Sep 9, 2024
Competing interests and funding: The authors have no conflict of interest to declare.
INTRODUCTION
Diagnosing chronic widespread musculoskeletal pain remains a challenge as it encompasses a wide range of different conditions. Among these, most patients with sarcoidosis report pain that is either musculoskeletal or small-fibre neuropathy related (1, 2). How sarcoidosis may induce musculoskeletal pain remains unclear.
CASE DESCRIPTION
A 52-year-old woman attended the outpatient clinic for all-day-long musculoskeletal pain that started 3 years earlier. This mainly involved the lower and upper limbs. She had been taking paracetamol, NSAIDs, sometimes tramadol and she had been undergoing physiotherapy. She was finally diagnosed as having fibromyalgia.
Her past medical records included hypertension, obstructive sleep apnoea syndrome, and type 2 diabetes mellitus for which she was on lisinopril plus hydrochlorothiazide and metformin. In addition, a stage III pulmonary sarcoidosis was diagnosed 10 years earlier. She then received a 1-year course of corticosteroids. Sarcoidosis had been considered in remission since then. She did not have any respiratory complaints.
On examination, her skin was unremarkable, as were cardiac and lung auscultation. Palpation of both upper and lower limbs revealed muscle tenderness. Muscle strength and peripheral neurological examination remained normal.
Laboratory tests showed only moderate inflammation: CRP 26.9 mg/L (<5). Previous blood tests displayed a similar range of inflammation as far back as 4 years earlier. An extensive workup was undertaken, including for viral, autoimmune, and systemic inflammatory diseases, which remained normal. Plain film and power doppler found neither articular erosions nor synovitis. Electromyography was performed and remained unremarkable. Chest scan, pulmonary function tests, and angiotensin converting enzyme (ACE) were not consistent with evolution of sarcoidosis. Myositis was also suggested. CK levels were normal. MRI of the lower limb did not find inflammation, oedema, or muscle structure anomaly. No hypersignal along the fascia was found, thus ruling out fasciitis.
An FDG PET scan showed multiple hypermetabolic infiltrates within the subcutaneous tissue, mainly located at the back of the thighs (Fig. 1a). A deep skin biopsy of the back of the thigh, including fascia, was then carried out. Pathological study found, within the adipose tissue, multiple foci of inflammatory cells including lymphocytes and multinucleated giant cells. Fibrous span between fat lobules also contained giant cells (Fig. 1b and c). In addition, asteroid bodies and inclusion bodies strongly suggested sarcoidosis. The fascia was not involved. Hypodermal sarcoidosis was then diagnosed.
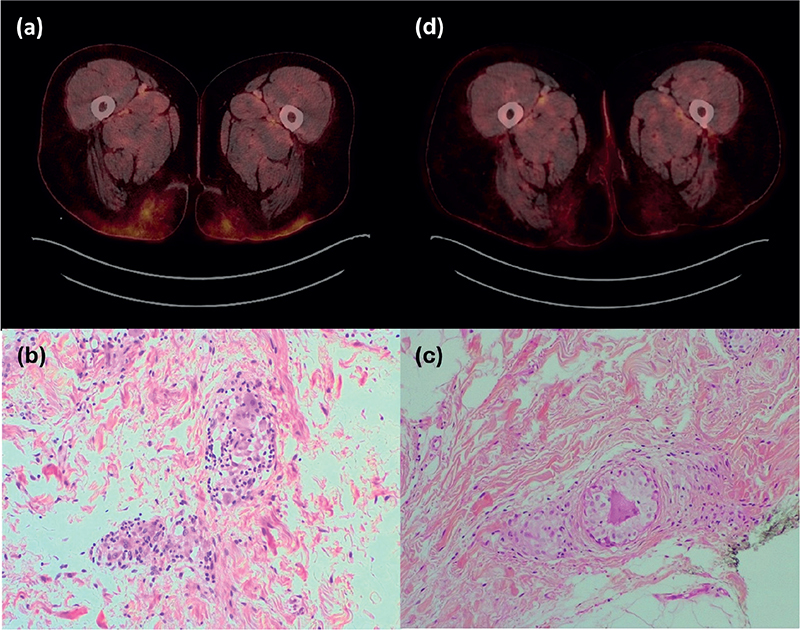
Fig. 1. Granulomatous infiltration of the hypoderm. (A) At the time of diagnosis: marked metabolic activity underlies the skin of the back of the thighs and extends deeper in the adipose tissue. (B) and (C) Biopsy studies: granulomas of different sizes lying within the fibrous span. Fat lobules appear closer. (C) An unusual triangular-shaped multinucleated giant cell (HES x 200). (D) FDG PET image 1 year following treatment start. Mild residual activity within the fat tissue.
An oral course of 24 mg methylprednisolone was given and then gradually tapered over the following months. Consequently, the diffuse painful syndrome reduced. Methotrexate was added a few months later as relapse occurred, presenting as pain recurrence along with increase of CRP. Finally, inflammation normalized 1 year after corticosteroids were started. A novel FDG PET scan found a frank reduction of the highly metabolically active infiltration of the thigh back (Fig. 1d).
DISCUSSION
This case shows a never previously described sarcoidosis involvement of the hypoderm. The skin is the second most common organ affected by sarcoidosis, with highly variable visible and non-painful lesions on the skin. Likewise, subcutaneous sarcoidosis usually refers to granulomatous infiltration with subcutaneous nodules or change in skin thickness (3). Pain in sarcoidosis may originate from joints, muscles, and increasingly recognized small-fibre neuropathy (2). It has been proven that sensory nerves also innervate the subcutaneous fatty tissue (4, 5). This suggests that inflammation driven by granulomas may activate sensory nervous fibres located within the hypoderm. Thus, this case provided a pathological basis for the so-called muscle pain.
Second, the FDG PET scan was able to indicate that an ongoing inflammatory process was developing under the skin. While most diagnostic studies rely on assessing small-fibre neuropathy in sarcoidosis-associated widespread pain, FDG PET scan could provide proof of abnormal metabolic activity under the skin. It should be remembered that these manifestations may develop without any other organ involvement. The hypermetabolic activity on FDG PET scan was mainly located in the thighs whilst the patient had widespread pain. This probably reflected the rate of inflammation on different areas of the body.
Interestingly, steroid therapy relieve the symptoms while others have reported that the latter was non-effective in small-fibre neuropathy (6).
We have presented a case of sarcoidosis-associated diffuse pain and have shown that this was related to granulomatous inflammation under the skin. This also suggest that PET scan may be useful to assessing sarcoidosis-induced ill-defined pain.
ACKNOWLEDGEMENT
This study was submitted to the local IRB: Comité d’éthique CHU Brugmann and was approved under the reference no. CE2021/270. In addition, informed consent was signed by the patient.
REFERENCES
- Maugars Y, Berthelot JM, Le Goff B, Darrieutort-Laffite C. Fibromyalgia and associated disorders: from pain to chronic suffering, from subjective hypersensitivity to hypersensitivity syndrome. Front Med 2021; 8: 666914. https://doi.org/10.3389/fmed.2021.666914
- Voortman M, Hendriks CMR, Elfferich MDP, Bonella F, Møller J, De Vries J, et al. The burden of sarcoidosis symptoms from a patient perspective. Lung 2019; 197: 155-161. https://doi.org/10.1007/s00408-019-00206-7
- Caplan A, Rosenbach M, Imadojemu S. Cutaneous sarcoidosis. Semin Respir Crit Care Med 2020; 41: 689-699. https://doi.org/10.1055/s-0040-1713130
- Roosterman D, Goerge T, Schneider S, Bunnett NW, Steinhoff M. Neuronal control of skin function: the skin as a neuro-immuno-endocrine organ. Physiol Rev 2006; 86: 1309-1379. https://doi.org/10.1152/physrev.00026.2005
- Raasing LRM, Vogels OJM, Veltkamp M, van Swol CFP, Grutters JC. Current view of diagnosing small fiber neuropathy. J Neuromuscul Dis 2021; 8: 185-207. https://doi.org/10.3233/JND-200490
- Tavee J, Culver D. Sarcoidosis and small-fiber neuropathy. Curr Pain Headache Rep 2011; 15: 201-206. https://doi.org/10.1007/s11916-011-0180-8