QUIZ SECTION
Annular Erythema on the Right Breast: A Quiz
Zhuoyu JIANG, Jianchi MA, and Zhenrui SHI*
Department of Dermatology, Sun Yat-sen Memorial Hospital, Sun Yat-sen University, 107 Yanjiang Rd W, Guangzhou, China 510120.
*E-mail: zrshi1989@outlook.com
Citation: Acta Derm Venereol 2024; 104: adv41176. DOI: https://doi.org/10.2340/actadv.v104.41176.
Copyright: © 2024 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Published: Sep 5, 2024
A woman in her 40s was referred to our hospital due to asymptomatic erythematous lesions on her right breast, which had appeared a month earlier and had gradually expanded. The fluorescence microscopy for fungi yielded negative results. She was previously diagnosed with breast cysts classified as a benign category using a breast imaging-reporting and data system (BI-RADS 2). Otherwise, her medical and family history was unremarkable. On physical examination, erythematous annular plaques were observed around the right areola without scales (Fig. 1). The skin biopsy revealed lymphovascular invasions of dysplastic cells characterized by a high nuclear-cytoplasmic ratio in the superficial dermis (Fig. 2).

Fig. 1. Clinical manifestation presented as annular erythema around the right areola.
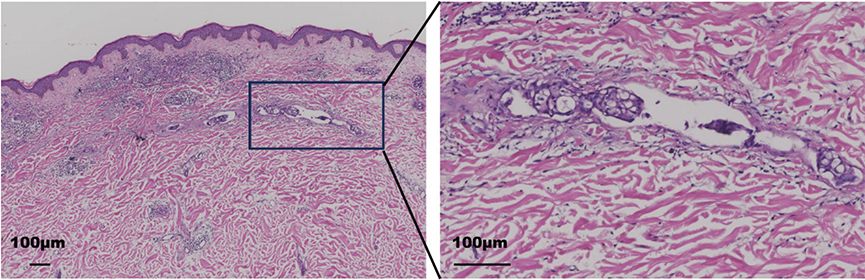
Fig. 2. Haematoxylin–eosin staining of skin biopsy showing lymphovascular invasions of dysplastic cells with scattered infiltration of inflammatory cells in the dermis.
What is your diagnosis?
Differential diagnosis 1: Tinea corporis
Differential diagnosis 2: Erythema annulare centrifugum
Differential diagnosis 3: Erythema gyratum repens
Differential diagnosis 4: Cutaneous metastatic breast cancer
See next page for answer.
ANSWERS TO QUIZ
Annular Erythema on the Right Breast: A Commentary
Diagnosis: Cutaneous metastatic breast cancer
Suspecting cutaneous metastatic cancer, we promptly referred the patient to an oncologist. Subsequent breast magnetic resonance imaging (MRI) displayed malignant neoplastic changes in the right breast involving the areola and metastasis in the ipsilateral axillary lymph node. A punch biopsy of the right axillary lymph nodes confirmed the presence of tumour cells. The tumour was negative for oestrogen receptor and progesterone receptor but positive for human epidermal growth factor receptor 2 (HER2). There was a notable increase in the Ki-67 proliferation index, which was recorded at 40%. Computed tomography (CT) of the head, neck, thorax, and abdomen suggested signs of liver and lung metastases. Consequently, she was diagnosed with right breast cancer with multiple metastases and was enrolled in a clinical trial involving HER2 specific antibody and docetaxel.
Breast cancer remains the primary cause of cancer-related disease burden among women worldwide, affecting 1 in 20 individuals globally and up to 1 in 8 in high-income countries (1). Skin manifestations are reported in 24% of women with metastatic breast cancer, making it the most prevalent cancer to metastasize to the skin in women. Approximately 13.7% of patients exhibit skin lesions either before or concurrently with the diagnosis of breast cancer (2). Cutaneous manifestations of breast cancer (CMBC) are commonly observed on the chest and abdominal areas but can also manifest on the limbs and in the head and neck regions. CMBC can present in various forms, with nodules being the most prevalent in 80% of cases. Other manifestations include alopecia, telangiectasia, melanoma-like lesions, erysipeloid carcinoma, subungual metastases, en cuirasse carcinoma, zosteriform metastases, eyelid metastases, and Paget-like lesions. The occurrence of annular erythema as a cutaneous symptom of breast cancer is rarely documented. To the best of our knowledge, only 9 cases of CMBC presenting as annular erythema have been reported, including ours (3–5). Importantly, all instances of CMBC with annular erythema occurred post-diagnosis of breast cancer, highlighting the diagnostic challenges posed by such atypical skin manifestations in our case.
The annular erythema subtype of cutaneous metastasis from breast cancer, resembling erythema annulare centrifugum or tinea corporis, often exhibits HER2 overexpression and lacks hormone receptors. This particular subtype, distinguished by cancer cells infiltrating dermal lymphovascular vessels without involving the dermis, is recognized as the classic histological hallmark of inflammatory breast cancer (IBC) (6). IBC, accounting for 2.5% of all breast cancer cases, is notably aggressive, characterized by a heightened risk of recurrence, aggressive disease progression, and diminished survival rates. Therefore, it is essential for the dermatologist to recognize this clinical form of cancer metastasis.
REFERENCES
- Britt KL, Cuzick J, Phillips KA. Key steps for effective breast cancer prevention. Nat Rev Cancer 2020; 20: 417–436. https://doi.org/10.1038/s41568-020-0266-x
- Johnson C, Friedmann DP, Gade A, Dhawan N, Hinchee-Rodriguez K, Mishra V, et al. Cutaneous manifestation as initial presentation of metastatic breast cancer: a systematic review. Cutis 2021; 107: E29–E36. https://doi.org/10.12788/cutis.0223
- Sabater V, Ferrando F, Morera A, Palomar L. Cutaneous metastasis of inflammatory breast carcinoma mimicking an erythema annulare centrifugum: a sign of locally recurrent cancer. Clin Exp Dermatol 2016; 41: 906–910. https://doi.org/10.1111/ced.12953
- Youh J, Yamaguchi Y, Hiraguchi E. Centrifugally spreading annular erythema as a dermatological indicator of metastatic breast carcinoma. Cureus 2024; 16: e51641. https://doi.org/10.7759/cureus.51641
- Cohen PR. Pleomorphic appearance of breast cancer cutaneous metastases. Cureus 2021; 13: e20301. https://doi.org/10.7759/cureus.20301
- Jagsi R, Mason G, Overmoyer BA, Woodward WA, Badve S, Schneider RJ, et al. Inflammatory breast cancer defined: proposed common diagnostic criteria to guide treatment and research. Breast Cancer Res Treat 2022; 192: 235–243. https://doi.org/10.1007/s10549-021-06434-x