ORIGINAL REPORT
Efficacy and Tolerability of Tebentafusp in Metastatic Uveal Melanoma: A Real-life Retrospective Multicentre Study
Lucille VITEK1, Thomas GORONFLOT2, Caroline DUTRIAUX3, Antoine DELEUZE4, Yannick LECORRE5, Anne-Bénédicte DUVAL-MODESTE6, Cécile FRENARD7, Géraldine JEUDY8, Anouck LAMOUREUX9, Caroline GAUDY-MARQUESTE10, Delphine LEGOUPIL11, Barouyr BAROUDJIAN12, Jean-Matthieu L’ORPHELIN13, Lucie PEUVREL14, Amir KHAMMARI15, Laurent MORTIER16# and Gaëlle QUÉREUX15#
1Department of Dermatology, CHU de Nantes, Nantes, 2Nantes University, Pôle Hospitalo-Universitaire 11: Santé Publique, Clinique des Données, INSERM, CIC 1413, CHU Nantes, Nantes, 3Department of Dermatology, Hôpital Saint-André, Bordeaux, 4Medical Oncology, Centre Eugène Marquis, Rennes, 5Department of Dermatology, CHU d’Angers, Angers, 6Université de Rouen, INSERM U519, Dermatologie, CHU de Rouen, Rouen, 7Department of Dermatology, Hôpital Saint-Louis de La Rochelle, La Rochelle, 8Department of Dermatology, Hôpital François-Mitterand, CHU Dijon Bourgogne, Dijon, 9Department of Dermatology, Hôpital Saint-Eloi, CHU de Montpellier, Montpellier, 10Department of Dermatology and Cutaneous Oncology, Aix-Marseille Université (AP-HM), Marseille, 11Department of Dermatology, INNOVEO, le fonds de dotation du CHRU de Brest, Brest, 12Department of Dermatology, Hôpital Saint-Louis (AP-HP), Paris, 13Department of Dermatology, CHU Caen Normandie, Caen, 14Institut de Cancérologie de l’Ouest, Nantes, 15Department of Dermatology, Nantes University, CIC 1413, INSERM UMR 1302/EMR6001 INCIT, CHU de Nantes, Nantes, and 16Department of Dermatology, CHU de Lille, Lille, France
#Shared senior authorship
Metastatic uveal melanoma is a rare disease with a poor prognosis. Usual treatments have not proven effective. Tebentafusp, a bispecific protein targeting melanoma cells and T lymphocytes, is the first approved treatment with a proven survival benefit in a randomized clinical. Our purpose was to evaluate tebentafusp’s real-life efficacy and tolerability for metastatic uveal melanoma. This retrospective study included patients from 14 French centres. Twenty-three patients were included. One-year survival was 66%; median progression-free survival was 5.7 months. Objective response rate was 23% and best overall response was complete remission for 4% of patients; partial remission for 18%, stable disease for 41%, and progressive disease for 36%. The most frequent adverse events were fever, chills, pruritus, and rash; 30% experienced severe adverse events. No death or treatment discontinuation was linked to adverse events. These data showed better overall survival with tebentafusp than that reported in historical cohorts.
SIGNIFICANCE
Metastatic uveal melanoma is a rare disease with a poor prognosis. Tebentafusp, a treatment targeting melanoma cells and T lymphocytes, is the first approved treatment with a proven survival benefit in a randomized clinical trial. We wanted to evaluate its real-life efficacy and tolerability. One-year survival was 66%; median progression-free survival was 5.7 months. The most frequent adverse events were fever, chills, pruritus, and rash. No death or treatment discontinuation was linked to adverse events. Our data showed better overall survival with tebentafusp than that reported in historical cohorts.
Key words: immunotherapy; tebentafusp; uveal melanoma.
Citation: Acta Derm Venereol 2024; 104: adv41297. DOI: https://doi.org/10.2340/actadv.v104.41297.
Copyright: © 2024 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Aug 6, 2024; Accepted after revision: Nov 13, 2024; Published: Dec 12, 2024
Corr: Pr Gaëlle Quereux, Department of Dermatology, CHU de Lille, 8ème étage, 1 place Alexis-Ricordeau, FR-44093 Nantes, France. E-mail: gaelle.quereux@chu-nantes.fr
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Uveal melanoma (UM) is the most common primary intraocular cancer. It affects the choroid in 90% of cases but can also affect the ciliary body or the iris. UM has a prevalence varying from 0.1 to 0.8 per million depending on latitude, age, phototype, and eye colour (1), and accounts for approximately 3%–5% of all melanomas (2). Its specific molecular profile, metastatic pattern, poor prognosis, and tumour-immune microenvironment distinguish it from cutaneous melanoma. Around 50% of patients will develop metastases, mainly in the liver (3). At the metastatic stage, median overall survival (OS) is approximately 1 year (median: 1.1 years; 95% CI: 1.0–1.1 years), and nearly all patients die within 5 years (4). Systemic therapies used in metastatic uveal melanoma (mUM) are the same as in cutaneous melanoma – primarily chemotherapy and immunotherapy. However, probably due to the different molecular and immune profile, these therapies have not proven their efficacy, and data from randomized controlled trials (RCTs) are lacking. The molecular landscape of UM and absence of easy druggable molecular targets make targeted therapies ineffective in UM.
Tebentafusp (TBP), a first-in-class immune-mobilizing monoclonal T-cell receptors against cancer (ImmTAC) agent, is the first approved treatment with a proven survival benefit in a randomized clinical trial for mUM. It consists of a soluble affinity-enhanced HLA-A02:01 restricted T-cell receptor – specific for glycoprotein 100 (gp100) expressed on melanoma cells – fused to an anti-CD3 single-chain variable fragment for engaging T cells (5, 6). About 50% of Caucasian individuals are HLA-A02:01 positive (7).
In the phase I study that included 42 patients who had failed a median of 2 previous treatments, median OS with TBP was 25.5 months and the 1-year OS rate was 67% (8). The follow-up phase II study involved 127 previously treated patients, for whom median OS was 16.8 months and the 1-year OS rate was 62%, despite a response rate of only 5% (9). In a phase III multicentre RCT comparing TBP with the investigator’s choice of treatment (pembrolizumab, ipilimumab, or dacarbazine) in first-line patients, the 1-year OS rate was higher in the TBP group than in the control group (TBP: 73%; control: 59%; hazard ratio [HR]: 0.51) (10). The results of the 3-year analysis confirm the long-term survival benefit of TBP (11). TBP-related adverse events (AEs) are frequent within the first weeks of treatment and then tend to decrease in incidence and severity. The most frequent toxicities can be divided into 2 groups: associated cytokine release syndrome (CRS) (fever, chills, hypotension, and hypoxemia) and skin-related AEs. The most common AEs in the phase III study were rash (83%), fever (76%), and pruritus (69%). Associated CRS occurred in 89% of the patients but was mostly grade 1 (99%). Grade 3 or 4 treatment-related AEs were reported in 44% of patients, but no treatment-related deaths (10). The phase II trial suggested better OS in those with a rash (9). However, the presence of a rash during week 1 was found not to be an independent predictor of overall survival benefit in the phase III study (10).
We conducted a nationwide retrospective multicentre study in France to evaluate the real-life efficacy and tolerability of TBP in patients with unresectable/mUM.
MATERIALS AND METHODS
Study population
This retrospective study was conducted in compliance with the Declaration of Helsinki of the World Medical Association (2013 amended version) on research involving human subjects. We collected data retrospectively using a questionnaire sent out to French centres treating patients with mUM. These centres were identified through the cutaneous oncology group of the French Society of Dermatology and from the national melanoma database (RicMel: NCT03315468). Centres that agreed to participate were asked to provide data on all patients aged > 18 years who had received ≥ 1 dose of TBP for the treatment of a metastatic (stage IV, per 8th edition of American Joint Committee on Cancer [AJCC] TNM system) and unresectable UM. All patients were informed and gave written informed consent for publication of their case details.
The data collected included patient demographics; Eastern Cooperative Oncology Group (ECOG) performance status; tumour genotype and cytogenetic profile, if available; previous local and systemic antitumour therapies; sites and number of organ systems affected by metastases; lactate dehydrogenase (LDH) and alkaline phosphatase (AP) levels at initial TBP administration. During the treatment phase, data on effectiveness (tumour response, OS, progression-free survival [PFS]) and tolerability (AE incidence, severity, and management) were collected.
Study endpoints
The primary endpoint was OS. Secondary endpoints were PFS and best overall response (BOR). Follow-up began at the initiation of TBP treatment. OS was calculated from TBP initiation to censoring or death. Tumoral response was assessed according to Response Evaluation Criteria in Solid Tumors (RECIST; https://recist.eortc.org/), version 1.1. PFS was calculated from TBP initiation to tumoral progression, death, or censoring. The interval for imaging was 3 months.
Percentages of AEs were calculated for fever, hypoxia, hypotension, chills, headache, nausea, rash, and pruritus. Data on severe AEs were collected only for fever, rash, hypoxia, and hypotension. They were defined as Common Terminology Criteria for Adverse Events (CTCAE version 5.0; https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm) grade ≥ 3 for fever and rash, and American Society for Transplantation and Cellular Therapy (ASTCT) Consensus Grading for Cytokine Release Syndrome grade ≥ 3 for hypoxia and hypotension. AE management was reported only for fever, hypoxia, and hypotension. Patients were hospitalized for 1 night with close monitoring (blood pressure, heart rate, saturation, temperature) for at least 16 h during for the first 3 infusions in accordance with the recommendations (https://www.ema.europa.eu/en/documents/product-information/kimmtrak-epar-product-information_en.pdf). From the fourth course onwards, monitoring for 1 h is sufficient, depending on the tolerance of the previous courses.
Statistical analysis
Continuous variables were summarized by means and standard deviations when normally distributed, and medians and interquartile ranges otherwise. Categorical variables were described using frequencies and percentages. Missing data were presented.
OS, PFS, and median time from primary diagnosis to metastatic progression were estimated using the Kaplan–Meier method. Confidence intervals (95%) were calculated. Analyses were performed using R statistical software (v4.1.1; R Core Team; R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
Study population
In this study, we included 23 patients from 14 French oncology and onco-dermatology centres. Baseline characteristics of these patients are summarized in Table I.
The median age of these patients was 63 years (IQR: 54–69 years), and most (61%) were women. In 15 patients, cytogenetic abnormalities or mutations were detected, including chromosome 3 monosomy (n = 4); chromosome 8 polysomy (n = 5); and abnormal BAP1 (n = 4), MBD4 (n = 1), GNAQ (n = 5), or GNA11 (n = 4) genes. The median time from primary diagnosis to metastatic progression was 3.8 years (IQR: 2.7–9.5) and median time from diagnosis of metastatic disease until start of TBP was 9 months (IQR: 4–17). Eleven patients (48%) had received ≥ 1 line of systemic therapy at the metastatic stage (including combined ipilimumab and nivolumab, anti-PD1 monotherapy, or chemotherapy): 5 patients (22%) had received 1 line of treatment, 4 patients (17%) had received 2 lines, and 2 patients (9%) had received 1 line of treatment before TBP initiation.
At the time of TBP initiation, 83% of the patients had an ECOG status of 0, with the remainder having an ECOG status of 1. AP levels were elevated in 32% of patients, while 52% had elevated LDH. HLA-A02:01 testing was positive for all patients tested (n = 23). The AJCC classification was M1a for 38% of patients, M1b for 48%, and M1c for 14%; 96% of patients had multiple metastases. Hepatic metastases only were found in 52% of patients, extrahepatic metastases only (excluding cerebral metastases) in 9%, and both hepatic and extrahepatic metastases in 39%.
Efficacy
By the end of follow-up (median: 12 months; IQR: 8–14), 8 deaths (35%) had occurred. The 1-year OS was 66% (95% CI: 48–90) (Fig. 1). Median OS could not be calculated as over half of the patients were alive by the end of their follow-up; however, the lower bound of the 95% CI suggests it was greater than 10.8 months (95% CI: 10.8 months–NA).
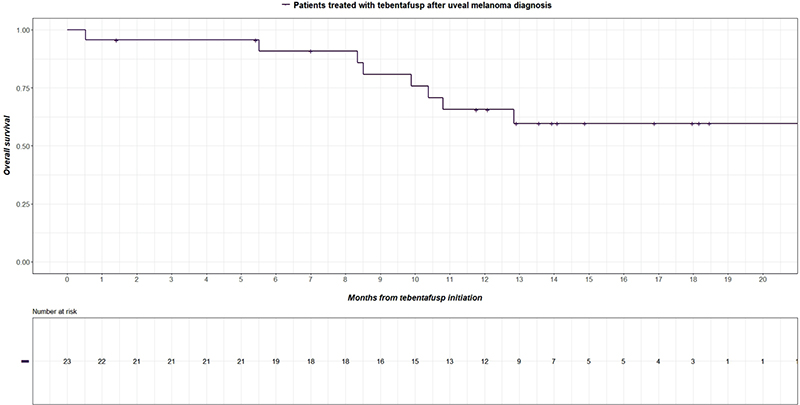
Fig. 1. Kaplan–Meier estimates of overall survival. Plus signs indicate censored data.
Median PFS was 5.7 months (95% CI: 3.2 months–NA) and the 1-year PFS rate was 34% (95% CI: 18%–63%) (Fig. 2).
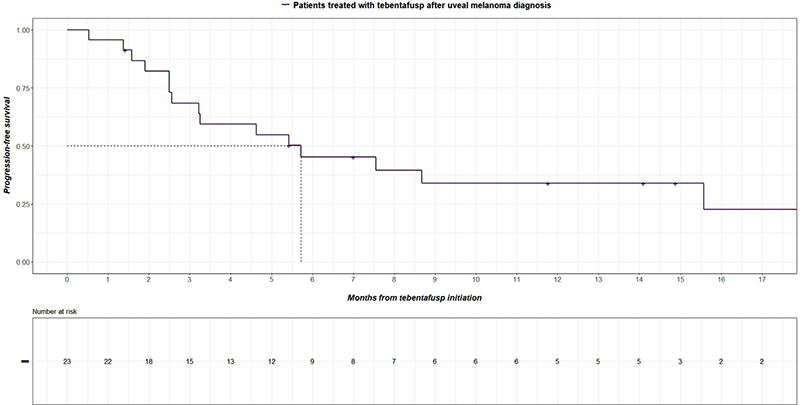
Fig. 2. Kaplan–Meier estimates of progression-free survival. Plus signs indicate censored data.
The BOR was, in 4% of cases, complete remission; 18% partial remission; 41% stable disease; and 36% progressive disease. Thus, the objective response rate (defined as complete or partial response, per RECIST guideline) was 23% and the disease control rate (defined as complete response, partial response, or stable disease, per RECIST guideline) was 64%.
At the end of follow-up, TBP treatment was ongoing for 43% of patients. In addition, 65% of patients had progressed on TBP and 35% had died. The median duration of treatment was 6.9 months (IQR: 4.6–13.5 months). The main reasons for discontinuation of TBP were progression in 77% of cases, death in 15% of cases, and the onset of acute leukaemia concomitant with disease progression in 1 patient.
We found no significant correlation between efficacy and ECOG status (HR = 1.51, 95% CI: 0.30–7.48), LDL level (HR = 0.40, 95% CI: 0.08–2.08), AP level (HR = 0.25, 95% CI: 0.05–1.15), TNM classification/size of the largest metastasis (3.1 to 8 cm, HR = 3.48, 95% CI: 0.39–31.16. > 8 cm, HR = 7.74, 95% CI: 0.70–86.15) and liver metastasis only vs extra-hepatic metastasis (HR = 0.78, 95% CI: 0.19–3.29).
Safety
Treatment-related adverse events (TRAEs) experienced by the patients are summarized in Table II. Overall, 87% (n = 20) of the patients experienced ≥ 1 AE. The most frequent were cytokine-related AEs (fever, 83% of patients; chills, 73%; hypotension, 29%) and skin-related AEs such as pruritus (70%) and rash (61%). Nausea was reported in 17% of patients and headache in 14% of patients. Other reported AEs were depigmentation of the skin in 3 patients; poliosis in 1 patient; and palmar– plantar erythrodysesthesia in 4 patients. A 72-year-old female patient was diagnosed with acute myeloid leukaemia 55 days after TBP initiation. Severe AEs occurred in 30% of patients and included 5 cases of rash, 4 cases of fever, and 2 cases of severe rash and fever combined (Fig. 3). There were no deaths or discontinuation of TBP related to AEs.

Fig. 3. Frequencies and severity of treatment-related adverse events. PPE: palmar–plantar erythrodysesthesia.
Intervention for CRS was paracetamol, antihistamines, corticosteroids, oxygen, and vascular filling therapy when needed, in accordance with the recommendations (https://www.ema.europa.eu/en/documents/product-information/kimmtrak-epar-product-information_en.pdf). There was no grade ≥ 3 for hypotension or hypoxemia, which means there was no use of nasal oxygen therapy > 6 L/min, high concentration mask, Venturi mask, or positive pressure (NIV, intubation) and no need for cardioactive fluids.
Most AEs occurred during the dose escalation phase and then decreased in frequency and severity. Among patients who experienced AEs with TBP, 45% were free of side effects after the first 3 weeks of treatment. No grade 3–4 CRS was observed after the first 3 doses. A grade ≥ 3 rash was observed after the first 3 doses. It was a recurrent rash, which had started during the third dose. It was a diffuse rash that regressed within 24 h on dermo corticoids and antihistamines and then subsequently resolved.
DISCUSSION
This was the first French real-life multicentre study to assess the efficacy and safety of TBP in mUM. The 1-year OS rate was 66% and median PFS was 5.7 months in our cohort of 23 patients.
The 1-year survival rate in our study was consistent with rates reported for the phase I (67%) and phase II (62%) studies (8, 9). However, it was lower than in the phase III (73%) study, likely because patients in that study were receiving first-line therapy, whereas 48% of our patients had previously failed several lines of therapy (10). Elevated LDH levels and poorer prognoses were more common in our study than in the phase III study, reflecting a higher metastatic burden and possibly explaining our lower 1-year OS rate (10). Furthermore, because of the real-life design of our study, we included patients regardless of any comorbidities.
A recent retrospective real-life study investigated TBP effectiveness and safety in 78 German patients. The authors did not provide the 1-year OS rate, but the median OS was 22.0 months and median PFS was 3.3 months, similar to the phase III study (12).
Median PFS and tumour response to TBP were both low in our study, like those in the literature (8–10), implying a clinically significant effect on patient outcomes, despite the lack of radiographically significant tumour shrinkage. In the phase III study, an OS benefit was also observed in patients for whom progression was the best objective response (HR = 0.43). A recent analysis compared post progression OS among patients who received TBP after progression and among those who did not. Those who did receive TBP following progression fared better (HR = 0.67). Some patients in the TBP arm also experienced disease stabilization for > 3 months after initial progression (13). Circulating tumour DNA decrease is associated with better overall survival and could be a new biomarker to assess TBP efficacity (9–11).
In the case of metastatic uveal melanoma, it is complicated to assess the efficacy of a treatment as there is no standard of care treatment. Many treatments have been tested, mainly in phase I–II studies. Some reported encouraging results but most were small studies with heterogeneous survival outcomes. Our 1-year OS rate for mUM patients administered TBP (66%) is higher than those reported, for all treatments combined, in the 2 main mUM meta-analyses by Rantala et al. (OS: 52%; median OS: 12 months; 2,494 patients included) and Khoja et al. (OS: 42%; median OS: 10 months; 912 patients included) respectively (4, 14).
Chemotherapy is not effective in mUM (15). Immunotherapy appears to be less efficient in UM, compared with cutaneous melanoma, probably due to a lower mutational burden, a different immunological microenvironment, and low PD-L1 expression. Simple immunotherapy does not appear to increase survival (4, 14). The efficacy of dual ipilimumab–nivolumab immunotherapy is still debated. Two recent phase II studies assessing it diverge in their findings: 1 reported a promising median survival of 19.1 months despite significant grade 3 or 4 AEs (16), while the other observed a median survival of 12.7 months (17). Two recent studies indirectly comparing TBP with dual ipilimumab–nivolumab immunotherapy appear to confirm the benefit of TBP (HR = 0.43) (18). Median OS was higher among TBP-treated patients (22.4 months) than in those treated with a combined immune checkpoint blockade (15.7 months) (19).
The best sequence of treatment in mUM is also a matter of debate. The real-life study by Tomsitz et al. (12) noted that median survival was longer among patients treated with a first-line immune checkpoint inhibitor followed by TBP (28 months) than among those treated with first-line TBP followed by immunotherapy (24 months) (p = 0.257). In contrast, another retrospective multicentre cohort study suggested similar efficacy, whether TBP was administered before or after anti-PD1+ipilimumab (20).
Liver-directed treatment involves surgery, local chemotherapy, immunoembolization and selective internal radiation therapy. In a recent metanalysis (4), median OS was longer with surgery (17 months), isolated hepatic perfusion (16 months), and immunoembolization (20 months). Another meta-analysis also found that patients receiving liver-directed treatments had significantly longer PFS and OS (14). These data should be interpreted carefully as they come from non-controlled studies on small and highly specific groups of patients with better prognoses and metastases usually limited to the liver. Finally, these 2 studies did not include patients treated with TBP. Novel approaches combining regional and systemic therapies, capitalizing on tumour-intrinsic vulnerabilities or aiming to enhance the antitumor immune response, are being developed to improve the outcomes in patients with metastatic uveal melanoma (21).
AEs were very frequent in our study. Overall, the safety profile was similar to that of the phase III study, mainly involving associated CRS-related (fever and chills) and cutaneous side effects. Cytokine-mediated AEs are mediated by T-cell activation and were reported in most patients, fever and chills being the most common. Cutaneous AEs were the second most common AEs and are likely caused by TBP recognition of gp-100 expressing melanocytes. Rash was less frequent in our study (61%) than in the phase III study (83%) (10), possibly due to the retrospective design of the former. No new safety signals occurred with 3 years’ follow-up (11). The percentage of TRAEs in our study was on a par with that in the real-life retrospective study by Tomsitz et al. (12). AEs were primarily mild to moderate; however, severe AEs occurred in 30% of patients, which is slightly below the percentage of grade 3 AEs in the phase III study (44%). These severe AEs were rash and fever. There was no death or discontinuation of TBP related to AEs.
A major limitation of our study was its retrospective design, which meant that the completeness of clinical data was beyond our control and depended on the usual practices of each centre: TRAEs were probably underestimated and data primarily concerning initial melanoma characteristics were missing. Patients were neither randomized nor was there a control group aside from a comparison with data from existing literature, which weakens the ability to draw definitive conclusions from the study’s findings. Moreover, we did not collect data on TBP interruption or postponement due to AEs. Another limitation was the small number of patients, due to the low prevalence of this disease. Probably due to this lack of power, we found no significant correlation between efficacy and other variables of interest: ECOG, LDH lever, AP lever, TNM classification, and presence of extra-hepatic metastasis. Finally, our results, although weaker – probably due to the small number of patients included – support the benefit of TBP, which is largely demonstrated by the phase III clinical trial. Nevertheless, we are aware that our real-life study on a small number of patients is not fully representative of the broader treatment experience.
The strength of our study is that we considered TBP treatment in a real-life setting with a heterogeneous population representative of daily practice, including patients receiving second-line therapy and patients with abnormal laboratory test results.
In conclusion, our real-life retrospective multicentre study observed a 1-year OS of 66% in patients treated with TBP for unresectable and metastatic uveal melanoma, which was lower than in the phase III study but still higher than those reported, for all treatments combined, in historical cohorts. Future RCTs comparing TBP with double immunotherapy are warranted.
ACKNOWLEDGEMENTS
The authors would like to thank the Groupe de Cancérologie Cutanée of the Société Française de Dermatologie (French Society of Dermatology) for their support.
IRB approval status: The RicMel database (Clinical Trials n°. NCT03315468) gathers data from clinical centres in different French regions. The study received ethics committee approval on 9 February 2012 (no. 12.108) from the Independent Ethics Committee in Paris and received authorization from the French Data Protection Agency (CNIL, DR-2012-259) on 28 May 2012.
REFERENCES
- Virgili G, Gatta G, Ciccolallo L, Capocaccia R, Biggeri A, Crocetti E, et al. Incidence of uveal melanoma in Europe. Ophthalmology 2007; 114: 2309–2315. https://doi.org/10.1016/j.ophtha.2007.01.032
- Jager MJ, Shields CL, Cebulla CM, Abdel-Rahman MH, Grossniklaus HE, Stern MH, et al. Uveal melanoma. Nat Rev Dis Primers 2020; 6: 1–25. https://doi.org/10.1038/s41572-020-0158-0
- Garg G, Finger PT, Kivelä TT, Simpson ER, Gallie BL, Saakyan S, et al. Patients presenting with metastases: stage IV uveal melanoma, an international study. Br J Ophthalmol 2022; 106: 510–517. https://doi.org/10.1136/bjophthalmol-2020-317949
- Rantala ES, Hernberg M, Kivelä TT. Overall survival after treatment for metastatic uveal melanoma: a systematic review and meta-analysis. Melanoma Res 2019; 29: 561–568. https://doi.org/10.1097/CMR.0000000000000575
- Bossi G, Buisson S, Oates J, Jakobsen BK, Hassan NJ. ImmTAC-redirected tumour cell killing induces and potentiates antigen cross-presentation by dendritic cells. Cancer Immunol Immunother 2014; 63: 437–448. https://doi.org/10.1007/s00262-014-1525-z
- Damato BE, Dukes J, Goodall H, Carvajal RD. Tebentafusp: T cell redirection for the treatment of metastatic uveal melanoma. Cancers 2019; 11: 971–987. https://doi.org/10.3390/cancers11070971
- Marincola FM, Venzon D, White D, Rubin JT, Lotze MT, Simonis TB, et al. HLA association with response and toxicity in melanoma patients treated with interleukin 2-based immunotherapy. Cancer Res 1992; 52: 6561–6566.
- Carvajal RD, Nathan P, Sacco JJ, Orloff M, Hernandez-Aya LF, Yang J, et al. Phase I study of safety, tolerability, and efficacy of tebentafusp using a step-up dosing regimen and expansion in patients with metastatic uveal melanoma. J Clin Oncol 2022; 40: 1939–1948. https://doi.org/10.1200/JCO.21.01805
- Carvajal RD, Butler MO, Shoushtari AN, Hassel JC, Ikeguchi A, Hernandez-Aya L, et al. Clinical and molecular response to tebentafusp in previously treated patients with metastatic uveal melanoma: a phase 2 trial. Nat Med 2022; 28: 2364–2373. https://doi.org/10.1038/s41591-022-02015-7
- Nathan P, Hassel JC, Rutkowski P, Baurain JF, Butler MO, Schlaak M, et al. Overall survival benefit with tebentafusp in metastatic uveal melanoma. N Engl J Med 2021; 385: 1196–1206. https://doi.org/10.1056/NEJMoa2103485
- Hassel JC, Piperno-Neumann S, Rutkowski P, Baurain JF, Schlaak M, Butler MO, et al. Three-year overall survival with tebentafusp in metastatic uveal melanoma. N Engl J Med 2023; 389: 2256–2266. https://doi.org/10.1056/NEJMoa2304753
- Tomsitz D, Ruf T, Heppt M, Staeger R, Ramelyte E, Dummer R, et al. Tebentafusp in patients with metastatic uveal melanoma: a real-life retrospective multicenter study. Cancers 2023; 15: 3430–3444. https://doi.org/10.3390/cancers15133430
- Sullivan RJ, Milhem MM, Demidov LV, Lewis KD, Schlaak M, Piperno-Neumann S, et al. Treatment with tebentafusp beyond radiographic progressive disease (PD) in metastatic uveal melanoma (mUM). J Clin Oncol 2022; 40: 9585–9585. https://doi.org/10.1200/JCO.2022.40.16_suppl.9585
- Khoja L, Atenafu EG, Suciu S, Leyvraz S, Sato T, Marshall E, et al. Meta-analysis in metastatic uveal melanoma to determine progression free and overall survival benchmarks: an international rare cancers initiative (IRCI) ocular melanoma study. Ann Oncol 2019; 30: 1370–1380. https://doi.org/10.1093/annonc/mdz176
- Rantala ES, Hernberg MM, Piperno-Neumann S, Grossniklaus HE, Kivelä TT. Metastatic uveal melanoma: the final frontier. Prog Retin Eye Res 2022; 90: 101041–101094. https://doi.org/10.1016/j.preteyeres.2022.101041
- Pelster MS, Gruschkus SK, Bassett R, Gombos DS, Shephard M, Posada L, et al. Nivolumab and ipilimumab in metastatic uveal melanoma: results from a single-arm phase II study. J Clin Oncol 2021; 39: 599 607. https://doi.org/10.1200/JCO.20.00605
- Piulats JM, Espinosa E, de la Cruz Merino L, Varela M, Alonso Carrión L, Martín-Algarra S, et al. Nivolumab plus ipilimumab for treatment-naïve metastatic uveal melanoma: an open-label, multicenter, phase II trial by the Spanish Multidisciplinary Melanoma Group (GEM-1402). J Clin Oncol 2021; 39: 586–598. https://doi.org/10.1200/JCO.20.00550
- Piulats Rodriguez JM, Piperno-Neumann S, Rutkowski P, Nathan P, Hassel JC, Espinosa E, et al. A propensity score weighted comparison of tebentafusp or pembrolizumab versus combination ipilimumab and nivolumab in untreated metastatic uveal melanoma. Ann Oncol 2022; 33: S924. https://doi.org/10.1016/j.annonc.2022.07.949
- Petzold A, Steeb T, Wessely A, Koch EAT, Vera J, Berking C, et al. Is tebentafusp superior to combined immune checkpoint blockade and other systemic treatments in metastatic uveal melanoma? A comparative efficacy analysis with population adjustment. Cancer Treat Rev 2023; 115: 102543–102551. https://doi.org/10.1016/j.ctrv.2023.102543
- Dimitriou F, Hassel JC, Orloff M, Hughes I, Kapiteijn E, Mehmi I, et al. Treatment sequence with tebentafusp (tebe) and anti-PD1/ipilimumab (PD1+IPI) in HLA-A2*02:01 patients (pts) with metastatic uveal melanoma (mUM). Ann Oncol 2022; 33: S929. https://doi.org/10.1016/j.annonc.2022.07.958
- Carvajal RD, Sacco JJ, Jager MJ, Eschelman DJ, Olofsson Bagge R, Harbour JW, et al. Advances in the clinical management of uveal melanoma. Nat Rev Clin Oncol 2023; 20: 99–115. https://doi.org/10.1038/s41571-022-00714-1