ORIGINAL REPORT
Hydroxychloroquine-induced Sweet’s Syndrome: A Case Report and Literature Review
Gustavo ALMEIDA-SILVA1  , Joana ANTUNES1,2 , Inês TRIBOLET DE ABREU1 , Filipe MONTEIRO1 , Pedro VASCONCELOS1, Luís SOARES-ALMEIDA1,2 and Paulo FILIPE1ñ3
, Joana ANTUNES1,2 , Inês TRIBOLET DE ABREU1 , Filipe MONTEIRO1 , Pedro VASCONCELOS1, Luís SOARES-ALMEIDA1,2 and Paulo FILIPE1ñ3
1Dermatology Department, Unidade Local de Saúde Santa Maria, Lisbon, 2Dermatology University Clinic, Faculty of Medicine, University of Lisbon, Lisbon, and 3Dermatology Research Unit, Instituto de Medicina Molecular, University of Lisbon, Lisbon, Portugal
Sweet’s syndrome (or acute febrile dermatosis) is a neutrophilic dermatosis with a characteristic presentation encompassing specific clinical (fever and erythemato-violaceous oedematous papules, plaques and nodules), laboratory (neutrophilia and increased inflammatory markers), and histological (dermal neutrophilic infiltrate without vasculitis) features. Its pathophysiology is poorly understood but there seems to be an auto-inflammatory component related to mutations in inflammasome genes. It has been subdivided into its classic form, malignancy-associated, and drug-induced, according to its aetiology. The condition usually responds rapidly to steroid therapy, but recurrences are common. This report presents an extremely rare case of hydroxychloroquine-induced Sweet’s syndrome, plus a review of the literature, which encompasses 3 previous cases of Sweet’s syndrome induced by hydroxychloroquine and 1 induced by chloroquine. Despite being relatively easy to diagnose, aetiological investigation poses challenges to the clinician, especially in the elderly population, as several confounding factors might be present. Further studies are necessary to shed light on the pathophysiology behind this entity, to further facilitate diagnostic workup and treatment strategies.
SIGNIFICANCE
Dermatological conditions (for example, Sweet’s syndrome) may be behind many more serious systemic diseases but may also be due to adverse drug reactions. It is complex to distinguish among all possible causes and we present some insight that might be helpful in doing so. Furthermore, we present some very rare cases of hydroxychloroquine-induced Sweet’s syndrome and review all previously reported cases. Our work is important to heighten awareness and improve the diagnosis and investigation of this condition.
Key words: Sweet; hydroxychloroquine; chloroquine; drug-induced; neutrophilic.
Citation: Acta Derm Venereol 2025; 105: adv41333. DOI: https://doi.org/10.2340/actadv.v105.41333.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Aug 13, 2024. Accepted after revision: Dec 9, 2024. Published: Jan 8, 2025.
Corr: Gustavo Almeida-Silva, Dermatology Department, Unidade Local de Saúde Santa Maria, Lisbon, Portugal. E-mail: 29711@ulssm.min-saude.pt
Competing interests and funding: The authors have no conflicts of interests to declare.
INTRODUCTION
Sweet’s syndrome (or acute febrile neutrophilic dermatosis) is one of the neutrophilic dermatoses, alongside pyoderma gangrenosum and subcorneal pustular dermatosis, among others. Despite being clinically heterogeneous, all these conditions exhibit intense neutrophilic infiltrate on histopathological examination. This entity is usually sub-grouped into (i) classic form (which encompasses idiopathic cases as well as those associated with either infections, vaccination, pregnancy, or inflammatory bowel disease), (ii) malignancy-associated (more frequently related to haematological malignancies), and (iii) drug-induced (1–6). To our knowledge there have only been 3 previously reported cases of hydroxychloroquine-induced Sweet’s syndrome (7, 8).
CASE REPORT
We report the case of a 71-year-old Brazilian man, who came to our walk-in emergency dermatology clinic with a 3-day history of widespread erythemato-violaceous papulonodules and plaques on the face, upper and lower limbs, and the trunk. He also reported fever (38.5ºC) and mentioned he had re-started therapy with hydroxychloroquine about a week before the onset of the symptoms. There was no history of previous infection or vaccination.
He mentioned similar symptoms 2 months previously, about 2 weeks after he had first been prescribed hydroxychloroquine for arthralgias. However, at that time, he discontinued hydroxychloroquine and took over-the-counter hydroxyzine 25 mg, which resulted in remission of the lesions.
The patient’s medical history was relevant for HIV-1 infection since 1995, for which he was treated with dolutegravir/rilpivirine and had had an undetectable viral load for several years. His latest CD4 count showed 405 cells/μL. He also had a history of pancytopenia and hand arthralgias due to chronic parvovirus B19 infection (persistently positive viral loads on PCR tests).
On examination dozens of tumid oedematous and erythemato-violaceous plaques and nodules were seen, gradually coalescing to form small to medium, irregular, sharply bordered, oedematous plaques, some with a vesicle-like appearance in the centre. They were symmetrically distributed on his arms, forearms, neck, back, and face (Fig. 1).
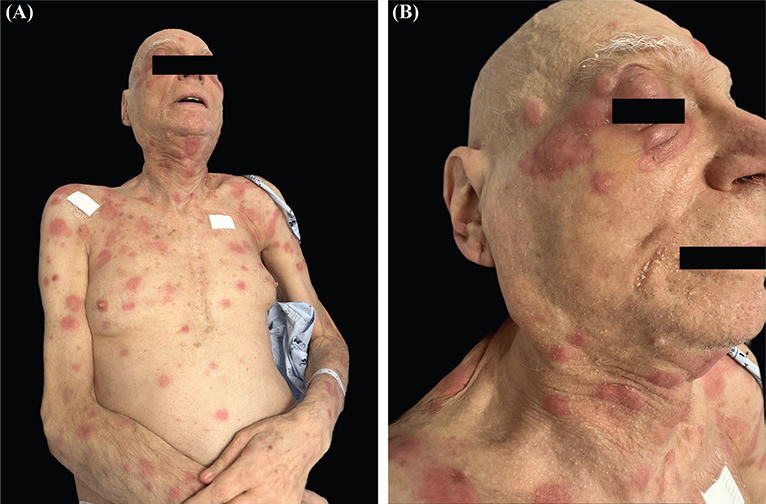
Fig. 1. Clinical pictures: erythemato-violaceous papules, nodules and plaques on (A) upper body and (B) face.
Complete blood count revealed neutrophilia (85.1%) without leucocytosis (9.2x109/L) and increased inflammatory markers (ESR 120 mm/h and CRP 8.99 mg/dL). To rule out neoplasm and infection, a full blood panel was performed, including blood cultures, viral serologies, and immunofixation, and the results were unremarkable. He underwent full-body computed tomography, which identified no tumours.
Skin biopsies were performed, and histopathological examination later showed normal epidermis but revealed neutrophilic inflammatory infiltrate, both interstitial and perivascular, in the superficial dermis. It also showed capillary ectasia around the papillary dermis but displayed no signs of vasculitis. These finds were consistent with Sweet’s syndrome (Fig. 2).
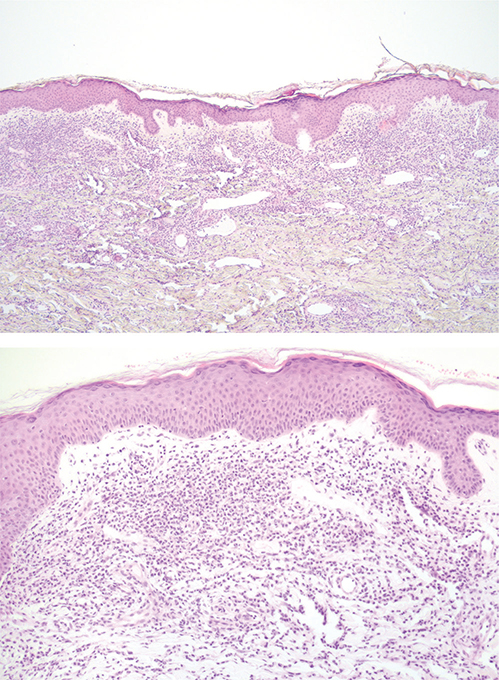
Fig. 2. Histopathological findings: neutrophilic inflammatory infiltrate in the upper dermis without vasculitis, papillary dermal oedema, dense diffuse and perivascular neutrophilic infiltrate, dilation of blood vessels.
The patient was started on prednisolone 20 mg/day, hydroxychloroquine was withdrawn, and the lesions remitted almost completely within 1 week.
A final diagnosis of Sweet’s syndrome was made, as our patient fulfilled 2 major and 3 minor criteria, as defined by Von den Driesch in 1994 (9).
LITERATURE REVIEW
In 2019, Bodard et al. (7) reported 2 cases of patients who developed Sweet’s syndrome following therapy with hydroxychloroquine for lupus erythematous and Sjögren’s syndrome, respectively. In the same year, Manzo et al. (8) reported 1 case of hydroxychloroquine-induced Sweet’s syndrome in a patient with Sjögren’s syndrome. Interestingly, as happened in our case, Manzo’s patient also experienced Sweet’s manifestations twice after a drug rechallenge was attempted. A similar scenario was previously described by El Moutaoui et al. (10) in 2009, the only report of chloroquine-induced Sweet’s syndrome describing a similar drug re-challenge scenario (Table I).
| Case reports | Year of publication | Offending drug | Underlying disease | Sweet’s syndrome criteria | DISS criteria |
| Bodard et al. (7) (2 cases) | 2019 | Hydroxychloroquine | SS | 2 major+2 minor | 5/5 |
| SLE | 2 major+2 minor | 5/5 | |||
| Manzo et al. (8) | 2019 | Hydroxychloroquine | SS | 2 major+3 minor | 5/5 |
| El Moutaoui et al. (10) | 2009 | Chloroquine | SLE | 2 major+3 minor | 5/5 |
DISCUSSION
Despite having a typical clinical presentation, the aetiological investigation of Sweet’s syndrome may prove challenging, especially in the elderly population, as these patients typically have more comorbidities and are polymedicated. Thorough review of systems is mandatory and, especially in the setting of immunosuppression, workup should include exclusion of underlying neoplasm (11, 12).
Some authors have considered HIV to be a risk factor for Sweet’s syndrome. Several mechanisms have been considered, namely neutrophilic chemotaxis in relation to a hypersensitivity reaction (13, 14), compromised T-helper lymphocytic function (15, 16), or HIV transactivating proteins (17), but no consensus has been reached. A review by Mudroch et al. (12) found most cases of Sweet’s syndrome reported in HIV-positive patients had other causes, namely immune reconstitution inflammatory syndrome in 25% of cases, AIDS-defining conditions, infections, and drugs. Although there have been some case reports of Sweet’s syndrome as an initial presentation of HIV (13, 17), others merely hypothesize HIV to be the causative agent after other aetiologies have been ruled out. None of the published cases suggest a link between Sweet’s syndrome and CD4 cell count, viral load, or disease duration (18–21). In our case, the fact that the patient presented the symptoms on 2 different occasions following the introduction of 1 drug and the fact that he had been HIV positive for over 20 years and had undetectable viral load seems to favour another aetiology.
Drug-induced Sweet’s syndrome is a rare entity. It is estimated that drug-induced Sweet’s syndrome accounts for less than 10% of all cases of Sweet’s syndrome (22, 23). A French study from 2023 found only 136 cases out of 994,789 adverse drug reaction events reported in a pharmacovigilance database. The most frequently reported offenders were bortezomib, azacitidine, pegfilgastrim, azathioprine, and bendamustine (24).
In 1996, Walker and Cohen (25) outlined specific criteria for drug-induced Sweet’s syndrome, which the patient in our case fulfilled entirely (Table II).
When the Naranjo score (26) was applied, our patient scored 9, which considers the drug as definitely having caused the adverse drug reaction.
In conclusion, this case report highlights a rare instance of hydroxychloroquine-induced Sweet’s syndrome, adding to the limited body of literature on drug-induced Sweet’s syndrome. The pathophysiology underlying this adverse reaction remains incompletely understood but may involve a hypersensitivity mechanism, immune dysregulation, or direct toxic effect on neutrophils. In recent years, Sweet’s syndrome has been categorized as an auto-inflammatory disease, which means that mutations in inflammasome genes might play a role in perpetuating recurrent inflammation despite the absence of circulating antigens (27–32). It is most frequently associated with colony-stimulating factors or cytostatic drugs, although many other associations have been described before (33). To our knowledge, it is the 4th published case establishing the association between hydroxychloroquine and Sweet’s syndrome and the first reporting a patient who did not have an autoimmune connective tissue disease.
Further studies and case reports are needed to better understand the incidence and mechanisms, and thus ameliorate diagnostic workup and management strategies. By documenting this case, we hope to provide valuable insights for healthcare providers, enhancing their ability to diagnose and manage similar cases effectively.
ACKNOWLEDGEMENTS
Data availability: The data used to support the findings of this study are available from the corresponding author upon request.REFERENCES
- Starita-Fajardo G, Lucena-López D, Ballester-Martínez MA, Fernández-Guarino M, González-García A, et al. Treatment strategies in neutrophilic dermatoses: a comprehensive review. Int J Mol Sci 2023; 24: 15622. https://doi.org/10.3390/ijms242115622
- Giasuddin AS, El-Orfi AH, Ziu MM, El-Barnawi NY. Sweet’s syndrome: is the pathogenesis mediated by helper T cell type 1 cytokines? J Am Acad Dermatol 1998; 39: 940–943. https://doi.org/10.1016/S0190-9622(98)70266-X
- Weiss EH, Ko CJ, Leung TH, Micheletti RG, Mostaghimi A, Ramachandran SM, et al. Neutrophilic dermatoses: a clinical update. Curr Dermatol Rep 2022; 11: 89–102. https://doi.org/10.1007/s13671-022-00355-8
- Heath MS, Ortega-Loayza AG. Insights into the pathogenesis of Sweet’s syndrome. Front Immunol 2019; 10: 414. https://doi.org/10.3389/fimmu.2019.00414
- Rochet NM, Chavan RN, Cappel MA, Wada DA, Gibson LE, et al. Sweet syndrome: clinical presentation, associations, and response to treatment in 77 patients. J Am Acad Dermatol 2013; 69: 557–564. https://doi.org/10.1016/j.jaad.2013.06.023
- Moschella SL, Davis MDP. Neutrophilic dermatoses. In: Bolognia JL, Jorizzo JL, Schaffer JV, editors. Dermatology. 3rd ed. Philadelphia: Elsevier Saunders, 2012: p. 423–438.
- Bodard Q, Carre D, Chenal P, Zarnitsky C, Midhat M, et al. Drug-induced Sweet’s syndrome related to hydroxychloroquine: about 2 cases. Rev Med Interne 2020; 41: 289–292. https://doi.org/10.1016/j.revmed.2019.08.010
- Manzo C, Pollio N, Natale M. Sweet’s syndrome following therapy with hydroxychloroquine in a patient affected with elderly-onset primary Sjogren’s syndrome. Medicines (Basel) 2019; 6: 111. https://doi.org/10.3390/medicines6040111
- von den Driesch P. Sweet’s syndrome (acute febrile neutrophilic dermatosis). J Am Acad Dermatol 1994; 31: 535–556. https://doi.org/10.1016/S0190-9622(94)70215-2
- El Moutaoui L, Zouhair K, Benchikhi H. Sweet syndrome induced by chloroquine. Ann Dermatol Venereol 2009; 136: 56–57. https://doi.org/10.1016/j.annder.2008.05.024
- Duke WH, Pantanowitz L. Editorial comment: Sweet syndrome – a diagnosis seeking a cause. AIDS Read 2008; 18: 136–138.
- Mudroch SM, Rohan C, Conger NG, Lindholm DA. Sweet syndrome in an elderly man with well-controlled human immunodeficiency virus. Cureus 2020; 12: e10330. https://doi.org/10.7759/cureus.10330
- Brady RC, Morris J, Connelly BL, Boiko S. Sweet’s syndrome as an initial manifestation of pediatric human immunodeficiency virus infection. Pediatrics 1999; 104: 1142–1144. https://doi.org/10.1542/peds.104.5.1142
- Haddow LJ, Lehloenya R, Mosam A, Malaka S, Moosa MY. Sweet syndrome: adverse drug reaction or novel manifestation of HIV-associated immune reconstitution inflammatory syndrome? J Am Acad Dermatol 2011; 65: e23–25. https://doi.org/10.1016/j.jaad.2010.11.052
- Deasy AM, Walker B, Layton AM, Lacey CJ. Sweet’s syndrome in a patient with haemophilia, HIV and hepatitis C infection. Int J STD AIDS 2012; 23: e11–13. https://doi.org/10.1258/ijsa.2009.009314
- Dong RJ, Huang SZ, Upadhyay P, Shrestha S, Zhai YJ, Li YY. Thalidomide in the treatment of Sweet’s syndrome and eosinophilic folliculitis associated with immune reconstitution inflammatory syndrome. Front Med (Lausanne) 2020; 6: 343. https://doi.org/10.3389/fmed.2019.00343
- Cabanillas M, Rodríguez-Blanco I, Sánchez-Aguilar D, Toribio J. Sweet syndrome: first manifestation of human immunodeficiency virus infection? Actas Dermosifiliogr 2008; 99: 83–84. https://doi.org/10.1016/S1578-2190(08)70204-X
- Hilliquin P, Marre JP, Cormier C, Renoux M, Menkes CJ, Puissant A. Sweet’s syndrome and monarthritis in a human immunodeficiency virus-positive patient. Arthritis Rheum 1992; 35: 484–486. https://doi.org/10.1002/art.1780350423
- Inamadar AC, Anitha B. HIV-seropositive patient with Sweet’s syndrome and nodular scleritis, showing dramatic response after adding dapsone to systemic corticosteroid therapy. Int J Dermatol 2008; 47: 836–838. https://doi.org/10.1111/j.1365-4632.2008.03648.x
- Corral M, Arana E, Recarte M, Marcia A, Fritschy M. Sweet syndrome in HIV-positive patient. Arch Argent Dermatol 2014; 64: 66–71.
- Coutinho P, Moura A, Souza B, António B, Alencar R, Valle F. Sweet syndrome and HIV infection: What can we interpret? Rev Soc Port Dermatol Venereol 2018; 76: 439. https://doi.org/10.29021/spdv.76.4.931
- Marcoval J, Martín-Callizo C, Valentí-Medina F, Bonfill-Ortí M, Martínez-Molina L. Sweet syndrome: long-term follow-up of 138 patients. Clin Exp Dermatol 2016; 41: 741–746. https://doi.org/10.1111/ced.12899
- Nelson CA, Noe MH, McMahon CM, Gowda A, Wu B, Ashchyan HJ, et al. Sweet syndrome in patients with and without malignancy: a retrospective analysis of 83 patients from a tertiary academic referral center. J Am Acad Dermatol 2018; 78: 303–309.e4. https://doi.org/10.1016/j.jaad.2017.09.013
- Martin S, Trenque T, Herlem E, Boulay C, Pizzoglio V, Azzouz B. Drug-induced Sweet’s syndrome: a case/non-case study in the French pharmacovigilance database. Br J Clin Pharmacol 2023; 9. https://doi.org/10.1111/bcp.15873
- Walker DC, Cohen PR. Trimethoprim-sulfamethoxazole-associated acute febrile neutrophilic dermatosis: case report and review of drug-induced Sweet’s syndrome. J Am Acad Dermatol 1996; 34: 918–923. https://doi.org/10.1016/S0190-9622(96)90080-8
- Naranjo CA, Busto U, Sellers EM, Sandor P, Ruiz I, Roberts EA, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther 1981; 30: 239–245. https://doi.org/10.1038/clpt.1981.154
- Saavedra AP, Kovacs SC, Moschella SL. Neutrophilic dermatoses. Clin Dermatol 2006; 24: 470–481. https://doi.org/10.1016/j.clindermatol.2006.07.009
- Imhof L, Meier B, Frei P, Kamarachev J, Rogler G, Kolios A, et al. Severe Sweet’s syndrome with elevated cutaneous interleukin-1β after azathioprine exposure: case report and review of the literature. Dermatology 2015; 230: 293–298. https://doi.org/10.1159/000371879
- Cohen PR. Sweet’s syndrome: a comprehensive review of an acute febrile neutrophilic dermatosis. Orphanet J Rare Dis 2007; 2: 34. https://doi.org/10.1186/1750-1172-2-34
- Richard SA, Kampo S, Hechavarria ME, Sackey M, Buunaaim ADB, Kuugbee ED, et al. Elucidating the pivotal immunomodulatory and anti-inflammatory potentials of chloroquine and hydroxychloroquine. J Immunol Res 2020; 2020: 4582612. https://doi.org/10.1155/2020/4582612
- Masters SL, Simon A, Aksentijevich I, Kastner DL. Horror autoinflammaticus: the molecular pathophysiology of autoinflammatory disease. Annu Rev Immunol 2009; 27: 621–668. https://doi.org/10.1146/annurev.immunol.25.022106.141627
- Cohen PR, Kurzrock R. Sweet’s syndrome revisited: a review of disease concepts. Int J Dermatol 2003; 42: 761–778. https://doi.org/10.1046/j.1365-4362.2003.01891.x
- Villarreal-Villarreal CD, Ocampo-Candiani J, Villarreal-Martínez A. Sweet syndrome: a review and update. Actas Dermosifiliogr 2016; 107: 369–378. https://doi.org/10.1016/j.ad.2015.12.001