SHORT COMMUNICATION
Pemphigoid with Autoantibodies against p200 and all Subunits of Laminin 332 Associated with Drug Eruption Caused by Piperacillin/tazobactam
Hanako MIYAHARA1, Rie HONDA1, Shusaku ITO1, Norito ISHII2 and Toshifumi NOMURA3*
1Dermatology Division, Hitachi General Hospital, Ibaraki, 2Department of Dermatology, Kurume University School of Medicine, Kurume, and 3Department of Dermatology, Institute of Medicine, University of Tsukuba, 1-1-1 Tennodai, Tsukuba, Ibaraki 305-8575, Japan. *E-mail: nomura@md.tsukuba.ac.jp
Citation: Acta Derm Venereol 2025; 105: adv41369. DOI: https://doi.org/10.2340/actadv.v105.41369.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Aug 24, 2024. Accepted after revision: Feb 19, 2025. Published: Mar 12, 2025.
INTRODUCTION
The most common types of pemphigoid include bullous pemphigoid, which presents with tense blisters mainly on the skin; mucous membrane pemphigoid, which presents with blisters and erosions predominantly on the mucous membranes; and anti-p200 pemphigoid, which is clinically similar to bullous pemphigoid and precedes psoriasis in one-third of patients (1). In bullous pemphigoid, BP180 and BP230 are the known target antigens (1). In mucous membrane pemphigoid, BP180, BP230, laminin 332, α6β4 integrin, laminin 311, and type VII collagen are the target antigens, as is p200 in anti-p200 pemphigoid (1).
Anti-p200 pemphigoid is a rare subepidermal blistering disease that manifests as mucosal lesions in approximately 20–38.5% of patients (2–4). Autoantibodies against laminin 332 have been detected in mucous membrane pemphigoid (5). Pemphigoid with autoantibodies against both p200 and laminin 332 is extremely rare. Herein, we report a case of pemphigoid with antibodies against p200 and all subunits of laminin 332 that was exacerbated by a drug eruption.
CASE REPORT
An 87-year-old Japanese man with a history of dementia but no specific history of skin disease was treated with piperacillin/tazobactam for pneumonia. On day 11 after the initiation of antibiotics, skin erosions developed on the extremities and face, particularly around the mouth and eyes. Because a drug eruption caused by piperacillin/tazobactam was suspected, the administration was promptly discontinued, and the patient was referred to our hospital.
The physical examination revealed tense blisters and erosions with crusts on the eyelids, lips, chin, neck, and penis (Fig. 1A, B). Skin erosions, erythema, and tense blisters were observed on the extremities (Fig. 1C). The patient was in very poor condition, and we could not perform a skin biopsy at that time. A chemiluminescent enzyme immunoassay was negative for anti-BP180 NC16a domain antibodies and anti-desmoglein 1 and 3 antibodies. Clinically, the patient was diagnosed with a severe drug eruption. Although oral prednisolone (PSL; 20 mg, 0.3 mg/kg/day) ameliorated the skin lesions, they recurred after the oral dose of PSL was tapered to 10 mg on the 17th day. At that time, erosions with crusts were noted on the lips and eyelids, and multiple erythematous areas, erosions, and tense blisters were observed on the trunk and extremities (Fig. 1D–F). A skin biopsy of the left thigh revealed a subepidermal blister with lymphocytic and neutrophilic infiltration into the dermis (Fig. 2A). Direct immunofluorescence (IF) staining revealed linear depositions of IgG, IgM, and C3 along the basement membrane zone (BMZ) (Fig. 2B). Indirect IF staining of 1 M sodium chloride-split skin revealed a linear deposition of IgG on the dermal side (Fig. 2C). Immunoblotting analysis of purified human laminin 332 showed that IgG autoantibodies in the patient’s serum reacted with the α3, β3, and γ2 subunits of laminin 332 (Fig. 2D). Immunoblotting analysis of normal human dermal extract detected anti-200 kDa laminin γ1 autoantibodies in the patient’s serum (Fig. 2E) but not autoantibodies against BP180, BP230, or type VII collagen. Based on these findings, pemphigoid with autoantibodies against all subunits of laminin 332 and p200 was diagnosed. Oral PSL (60 mg/day, 1 mg/kg/day) rapidly ameliorated the skin lesions.

Fig. 1. Clinical presentation at the initial visit. (A, B) Erosions with crusts on the eyelids, lips, chin, neck, and penis. (C) Erosions and tense blisters with less erythema on the forearms. Clinical presentation at the time of relapse showing (D) erosions with crusts on the lips and eyelids and (E, F) erythema, erosions, and tense blisters on the trunk and dorsum of the foot.
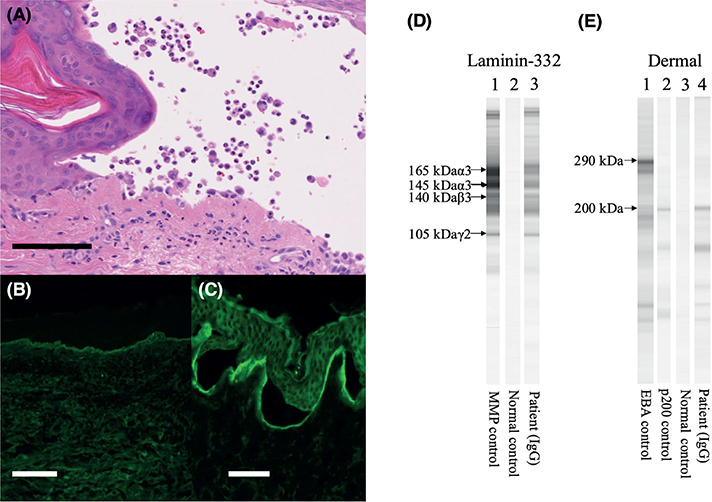
Fig. 2. (A) Haematoxylin-eosin staining of a skin biopsy of erythema on the left thigh showing a subepidermal blister and lymphocytic and neutrophilic infiltration in the dermis (bar=100 μm). (B) Direct immunofluorescence staining showing linear IgG deposition along the basement membrane zone (bar=100 μm). (C) Indirect immunofluorescence staining showing IgG deposition on the dermal side of 1 M NaCl split skin. (bar=50 μm). (D) Immunoblotting analysis of purified human laminin 332. IgG antibodies in the patient’s serum reacted with the 165 kDa, 145 kDa α3, 140 kDa β3, and 105 kDa γ2 subunits. (E) Immunoblotting analysis of a purified human dermal extract. IgG antibodies in the patient’s serum reacted with 200 kDa laminin γ1 (p200).
Piperacillin/tazobactam was administered for a urinary tract infection on day 5 after the initiation of PSL (60 mg). Similar to the initial symptoms, erythema with erosions appeared on the trunk and extremities on the fourth day of piperacillin/tazobactam administration. Discontinuation of piperacillin/tazobactam immediately attenuated the skin symptoms. The Naranjo score was 6, indicating the coexistence of a drug eruption and pemphigoid. Cyclosporine A (150 mg/day) was added on day 36, after increasing the PSL dose to 60 mg/day. Over 6 weeks, the PSL dose was gradually decreased to 30 mg/day. After discharge from the hospital, the patient continued receiving 30mg/day of PSL from his family physician, because he was unable to visit our hospital.
DISCUSSION
In the present case, the patient was initially suspected of having a drug eruption from piperacillin/tazobactam, or pemphigoid. Because performing a skin biopsy was difficult, we made a tentative diagnosis of a drug eruption based on negative anti-BP180 NC16a domain antibodies. The subsequent course and laboratory tests led to the diagnosis of both a drug eruption and pemphigoid, with autoantibodies against all subunits of laminin 332 and p200. Distinguishing rapidly progressing pemphigoid from a drug eruption is difficult. Although pemphigoid generally follows a chronic course, drug eruptions often present with acute onsets. Notably, pemphigoid with a rapid progression mimicking Stevens–Johnson syndrome has been reported (6, 7). In these cases, a drug eruption, rather than pemphigoid, was suspected at the initial visit because of the rapid clinical course, similar to that in the present case. In addition, although pemphigoid associated with piperacillin/tazobactam has not been reported, bullous pemphigoid associated with amoxicillin has been reported (8, 9). Although the role of a drug eruption in the development of pemphigoid is unclear in our case, the fragility of the BMZ due to the drug eruption may have contributed to the onset of pemphigoid.
For anti-p200 pemphigoid, mucous involvement is uncommon, whereas skin symptoms are predominant. Its histopathology is characterized by subepidermal blisters with neutrophil infiltration (2, 4). As 90% of anti-p200 pemphigoid sera recognize laminin γ1, anti-laminin γ1 pemphigoid has been proposed as a new term for this disease (2). Recently, Goletz et al. revealed that anti-p200 pemphigoid sera show reactivity against laminin β4, and laminin β4 is an additional target antigen in anti-p200 pemphigoid (2, 10). In contrast, pemphigoid with autoantibodies against laminin 332 typically presents with mucous involvement, which is histopathologically characterized by subepidermal blisters with sparse inflammatory cells (5, 11). Only 2 cases of pemphigoid with autoantibodies against all subunits of laminin 332 and p200 have been reported, and both showed skin and mucosal involvement (12, 13). Liu et al. showed that the levels of autoantibodies against both p200 and laminin 332 decreased after treatment (13). Furthermore, the levels of autoantibodies against laminin 332 increased during relapse, whereas autoantibodies against p200 were not evaluated (13). Although the autoantibody levels and histopathology were not analysed at the initial diagnosis in the present case, the histopathology at relapse revealed neutrophilic infiltration, which, together with the absence of mucous symptoms, shows features of anti-p200 pemphigoid.
In the present case, a drug eruption developed concurrently with and exacerbated the pemphigoid. Owing to the co-occurrence of these 2 conditions, the diagnosis was difficult. Clinicians should consider the possibility of the concurrent development of a drug eruption and pemphigoid in patients with rapidly progressing pemphigoid.
REFERENCES
- Schmidt E, Zillikens D. Pemphigoid diseases. Lancet 2013; 381: 320–332. https://doi.org/10.1016/S0140-6736(12)61140-4
- Dainichi T, Koga H, Tsuji T, Ishii N, Ohyama B, Ueda A, et al. From anti-p200 pemphigoid to anti-laminin γ1 pemphigoid. J Dermatol 2010; 37: 231–238. https://doi.org/10.1111/j.1346-8138.2009.00793.x
- Goletz S, Hashimoto T, Zillikens D, Schmidt E. Anti-p200 pemphigoid. J Am Acad Dermatol 2014; 71: 185–191. https://doi.org/10.1016/j.jaad.2014.02.036
- Kridin K, Ahmed AR. Anti-p200 pemphigoid: a systematic review. Front Immunol 2019; 10: 2466. https://doi.org/10.3389/fimmu.2019.02466
- Shi L, Li X, Qian H. Anti-laminin 332-type mucous membrane pemphigoid. Biomolecules 2022; 12: 1461. https://doi.org/10.3390/biom12101461
- Murata S, Sumikawa Y, Takahashi H, Ota M, Kusatake K, Niihara H, et al. Case of mucous membrane pemphigoid with immunoglobulin G antibodies to the beta 3 subunit of laminin-332 showing clinically Stevens–Johnson syndrome-like generalized blistering mucocutaneous lesions. J Dermatol 2015; 42: 1126–1128. https://doi.org/10.1111/1346-8138.13062
- Sugawara A, Koga H, Tsutsumi M, Ishii N, Nakama T. A case of mucous membrane pemphigoid with anti-laminin alpha 3 and beta 3 antibodies initially mimicking Stevens–Johnson syndrome. Int J Dermatol 2022; 61: e199–e200. https://doi.org/10.1111/ijd.15714
- Miralles J, Barnadas MA, Baselga E, Gelpí C, Rodríguez JL, de Moragas JM. Bullous pemphigoid-like lesions induced by amoxicillin. Int J Dermatol 1997; 36: 42–47. https://doi.org/10.1111/j.1365-4362.1997.tb03302.x
- Verheyden MJ, Bilgic A, Murrell DF. A systematic review of drug-induced pemphigoid. Acta Derm Venereol 2020; 100: adv00224. https://doi.org/10.2340/00015555-3457
- Goletz S, Pigors M, Lari TR, Hammers CM, Wang Y, Emtenani S, et al. Laminin β4 is a constituent of the cutaneous basement membrane zone and additional autoantigen of anti-p200 pemphigoid. J Am Acad Dermatol 2024; 90: 790–797. https://doi.org/10.1016/j.jaad.2023.11.014
- Rose C, Schmidt E, Kerstan A, Thoma-Uszynski S, Wesselmann U, Käsbohrer U, et al. Histopathology of anti-laminin 5 mucous membrane pemphigoid. J Am Acad Dermatol 2009; 61: 433–440. https://doi.org/10.1016/j.jaad.2009.02.012
- Li X, Qian H, Ishii N, Yamaya M, Fukuda H, Mukai H, et al. A case of concurrent antilaminin γ1 pemphigoid and antilaminin-332-type mucous membrane pemphigoid. Br J Dermatol 2014; 171: 1257–1259. https://doi.org/10.1111/bjd.13107
- Liu W, Sun X, Gao Y, Li H, Shi L, Cheng L, et al. A Chinese case of concurrent anti-laminin γ1 pemphigoid and anti-laminin 332-type mucous membrane pemphigoid. J Dermatol 2023; 50: e69–e71. https://doi.org/10.1111/1346-8138.16513