ORIGINAL REPORT
Surgery or Non-invasive Treatment for Superficial Basal Cell Carcinoma: Does a Patient Decision Aid Help to Make a Personalized Treatment Decision?
Lieke C. J. VAN DELFT1,2, Myrthe M. G. MOERMANS1,2, Brigitte A. B. ESSERS3, Patty J. NELEMANS4, Klara MOSTERD1,2, Marieke E. C. VAN WINDEN5, Satish F. K. LUBEEK5 and Nicole W. J. KELLENERS-SMEETS1,2
1Department of Dermatology, Maastricht University Medical Center+, Maastricht, 2GROW School for Oncology and Reproduction, Maastricht University, Maastricht, 3Department of Clinical Epidemiology & Medical Technology Assessment, Maastricht University Medical Center+, Maastricht, 4Department of Epidemiology, Maastricht University, Maastricht, and 5Department of Dermatology, Radboud University Medical Center, Nijmegen, the Netherlands
Patients with a superficial basal cell carcinoma can be treated surgically or non-invasively, all with specific (dis)advantages. An investigation was undertaken into whether the preference for surgery or non-invasive treatment of a superficial basal cell carcinoma differs between patients who used a patient decision aid and a control group. Secondly, whether patients were satisfied with their decision post-treatment was investigated. A prospective observational study was performed comparing patients with a superficial basal cell carcinoma who used a patient decision aid (patient decision aid group) with a control group. The primary outcome was the proportion of patients that chose non-invasive treatment. A secondary outcome was the mean score of “effective decision-making” on the Decisional Conflict Scale 3 months post-treatment. In the patient decision aid group, 48.6% (52/109) seemed to prefer non-invasive treatment vs 40.8% (42/103) in the control group (p = 0.255); the result was not significant. Three months post-treatment, the adjusted between-group mean difference in “effective decision-making” was –4.10 (p = 0.082) favouring the patient decision aid group (effect size 0.3). To conclude, patients who used a patient decision aid seemed to choose non-invasive therapy over surgery slightly more often but the result was not significant.
SIGNIFICANCE
Using the patient decision aid did not have a significant effect on the treatment decision. However, patients with a first-time superficial basal cell carcinoma did significantly more often choose non-invasive treatment after using the patient decision aid. Implementation of a patient decision aid could help patients make an effective decision, and one that they are still satisfied with 3 months after treatment.
Key words: basal cell carcinoma; decision-making; shared; decision support techniques.
Citation: Acta Derm Venereol 2025; 105: adv41914. DOI: https://doi.org/10.2340/actadv.v105.41914.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Aug 30, 2024; Accepted after revision: Mar 9, 2025. Published: Apr 7, 2025
Corr: Lieke C. J. van Delft, Dermatology Department, Maastricht University Medical Center+, PO Box 5800, 6229 HX Maastricht, The Netherlands. Email: liekevandelft@msn.com
Competing interests and funding: The authors have no conflicts of interest to declare.
The study was funded by a grant (€3,000) from Health Foundation Limburg (Stichting Akkermans). This is a private foundation that supports scientific research in Limburg, the Netherlands. The grant was used for the development of the patient decision aid.
INTRODUCTION
There are several treatment options for superficial basal cell carcinoma (sBCC), each with specific advantages and disadvantages (1, 2). Surgery is the gold standard treatment with the lowest recurrence rates, but patients may prefer non-invasive therapies for other reasons. Factors like possible complications, side effects, costs, treatment duration, cosmetic outcome, and convenience of treatment (at home or in hospital) can be of influence on patients’ decision-making (3). Which treatment is most suited for an individual patient depends on patients’ values (what they deem important) and their personal situation, which makes the treatment decision a preference-sensitive one.
A patient decision aid (PDA) is a tool that can support patients in making a preference-based treatment decision by presenting characteristics of treatments in an understandable and objective manner (4). Our research group developed and field-tested a PDA for patients with an sBCC (5, 6). The PDA contains information on sBCC, treatment options (surgery, 5-fluorouracil [5FU], imiquimod, photodynamic therapy [PDT], and watchful waiting), the characteristics and outcomes of these therapeutic options, and patient education on UV exposure and self-examination. It also focuses on value elicitation, which means that patients are supported to think about what they deem important attributes of a treatment (5).
A large Cochrane review on PDAs concluded that patients with non-dermatological diseases who used a PDA more often chose less invasive treatment options with, for example, a lower risk of complications or fewer side effects (4). Stacey et al. (4) also reported that using a PDA leads to higher quality of the decision, meaning that the match between the chosen treatment and patients’ values improved when a PDA was used. Within the dermatological field little is known about the effects of using a PDA on treatment decisions (7). A pilot study performed with 10 psoriasis patients who used a PDA showed that most patients chose a treatment that matched their disease severity (ranging from topical to systemic oral and injectable treatments) (8). Many dermatologists assume that patients with sBCC prefer non-invasive therapy to surgery, which is in line with studies in other fields where patients more often chose less invasive therapies, but no information is available regarding this topic (9, 10).
The latest Cochrane review on management of BCC concludes that non-invasive treatments are important alternative options for low-risk BCC, as recurrence rates are acceptable (11). Furthermore, physicians and policy-makers may prefer non-invasive therapy because the high incidence of BCC puts a high burden on healthcare resources (12). However, well-informed patients may value low recurrence rate as most important, and could therefore prefer surgery over non-invasive treatments, in contrast to what physicians might think (3). To our knowledge, there is no literature available on the influence of using a PDA on treatment decisions within the field of dermato-oncology.
First, we aimed to study whether patients with an sBCC who used a PDA differ in their preference for surgery vs non-invasive treatment when compared with a control group who did not use a PDA. Secondly, we investigated whether patients are still satisfied with their treatment decision 3 months after treatment.
MATERIALS AND METHODS
Study design
Data from a multicentre prospective observational study were used. The primary aim of that study was to evaluate whether using the PDA led to a reduction in decisional conflict level and increased knowledge of BCC and treatment options (6). The online PDA, along with all information provided to the patients, can be accessed online in Dutch through the following link: https://keuzehulpbcc.nl/. In the current study, information from participants was used to investigate whether using a PDA influenced the treatment decision of patients with a newly diagnosed sBCC.
The group of patients that used the PDA will be referred to as the PDA group; the group that did not use the PDA will be considered the control group. The study protocol was approved by the institutional review board of Maastricht University Medical Centre+ in the Netherlands (METC azM/UM). The study was performed in accordance with the Declaration of Helsinki. The study was registered at clinicaltrials.gov (NCT05628714). Details of the study protocol can be found elsewhere (6).
Participants and data collection
Patients were included if they were over 18 years old, had an sBCC that was clinically or histopathologically confirmed, and were able to read (Dutch). The study was conducted in 2 academic hospitals (Maastricht University Medical Centre+ and Radboud University Medical Centre) and a regional hospital (Catharina Hospital Eindhoven) in the Netherlands.
All patients received information from their physician on the diagnosis, treatment options (surgery versus non-invasive treatments such as imiquimod, 5FU, PDT, and no treatment), associated benefits and risks of treatments, and education on sun exposure and self-examination of the skin. Patients and physicians in the control group came to an immediate shared treatment decision. Patients in the PDA group received a web link to the PDA, and after consulting the PDA, a second appointment took place to make the shared treatment decision (via telephone).
All patients received the Decisional Conflict Scale (DCS) 3 months post-treatment to evaluate their satisfaction with their treatment decision (Appendix A). The DCS is a questionnaire that measures uncertainty associated with health-related decisions and consists of 3 subscales (4, 13). The subscale “effective decision-making” was used in this study and includes 3 questions: (i) “I feel I have made an informed decision”, (ii) “my decision shows what is important to me”, and (iii) “I am satisfied with my decision”. Patients scored the degree of (dis)agreement with these statements on a 5-point Likert scale (the user manual of the DCS was used to calculate final scores ranging from 0–100). Low scores mean that patients are satisfied with their treatment decision after completion of the treatment: patients feel they have made an informed, value-based decision. The minimally relevant effect size (Cohen’s effect size) for the DCS scores on the effective decision-making subscale is considered to be 0.2–0.3 (14).
Baseline characteristics were collected including age, gender, educational level, having a history of BCC, previous experience with surgical and non-invasive treatments, simultaneous treatment of a second/third cutaneous malignancy, and a health-related quality of life visual analogue scale (VAS) score according to the EuroQol 5D-5L questionnaire before treatment (15). Relevant tumour characteristics were also recorded including size (largest diameter in mm) and location.
Outcome measures
The primary outcome of this study is the proportion of patients that chose non-invasive treatment. The secondary outcomes were the mean scores on the subscale “effective decision-making” and separate questions of this subscale of the DCS at 3 months post-treatment. The effect size was calculated to assess the clinical relevance of the effect of the PDA on patient satisfaction with the treatment decision.
Statistical analysis
Categorical and nominal variables are expressed as absolute numbers and percentages. Continuous variables are presented as median with range (if non-normally distributed) or as mean values with standard deviation (if normally distributed). A multivariate logistic regression analysis was performed to calculate odds ratios with p-values with adjustment for potential confounding by baseline differences between the groups. An adjusted odds ratio > 1 indicates a preference for non-invasive treatment over surgery.
The scores on the subscale “effective decision-making” were checked for normality, and between-group differences in mean scores were tested for significance with a t-test for independent samples.
The effect size (Cohen’s d) was calculated by dividing the mean difference between the 2 groups by the standard deviation of the mean difference. A multivariate linear regression analysis was conducted to adjust for potential confounding by baseline differences between the PDA group and control group.
We considered p-values < 0.05 as statistically significant. The data were analysed using SPSS version 23.0 (IBM Corp, Armonk, NY, USA) or OpenEpi (https://openepi.com/).
The sample size was calculated to detect a Cohen’s effect size of 0.4 (for the total score on the DCS in the primary study) (6) in accordance with the DCS user manual (14) with a power of 80% and a two-sided alpha of 5%. Both groups required at least 99 patients. The predicted response rate was 80%. Thus, per group, the aim was to include 123 patients (99/0.8).
RESULTS
In the period April 2018 to July 2019, before the PDA was implemented, 120 patients were included in the control group of which 103 patients (86%) completed all questionnaires. None of the patients refused participation in the control group. The PDA was implemented in the period July 2019 to December 2020. Thirty-four patients did not want to participate for different reasons. Fifteen of these patients indicated that they were certain of their decision even before using the PDA (11 of these patients chose surgical treatment, 2 chose imiquimod, for the other 2 patients the decision was unknown). Ultimately, 133 patients were included in the PDA group of which 109 patients (82%) responded. The patient flow is shown in Fig. 1. The reasons for incomplete response or non-response were not clear.
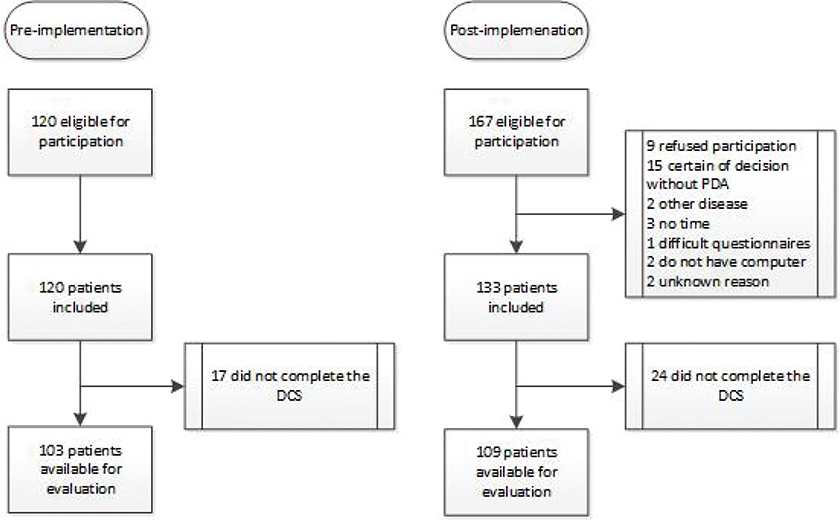
Fig. 1. Patient flowchart: data used to evaluate the primary outcome measure. DCS: Decisional Conflict Scale; PDA: patient decision aid.
Table I presents the distribution of baseline characteristics in the PDA and control group. There were several small differences, especially for BCC size, but these differences were not statistically significant.
Primary outcome
In the PDA group 48.6% (52/109) preferred non-invasive treatment vs 40.8% (42/103) in the control group. This difference was not statistically significant (p = 0.255). The unadjusted odds ratio was 1.37 (95% CI 0.80–2.37, p = 0.255). After adjustment for small differences in baseline characteristics between the PDA and control group using multivariate linear regression, the adjusted odds ratio was 1.51 (95% CI 0.82–2.78, p = 0.185) (Table II). The patients in the PDA group who chose a non-invasive treatment option most often preferred imiquimod (39/52, 75%), followed by 5FU (8/52, 15.4%), and MAL-PDT (5/52, 9.6%). Only 1 patient chose watchful waiting. In the control group most patients chose imiquimod (34/42, 81%), followed by 5FU (2/42, 4.8%), and MAL-PDT (6/42, 14.3%).
Table II indicates to what extent patient and tumour characteristics are associated with treatment choice. Patients with a positive history of BCC were more likely to choose non-invasive treatment than patients who presented with a first BCC (OR = 2.28, p = 0.014). Patients with an sBCC on the extremities also seemed to prefer non-invasive treatment more frequently compared with patients with an sBCC in the head and neck area, but this difference was not statistically significant (OR = 2.37, p = 0.077).
Effective decision-making 3 months post-treatment
Table III shows that, 3 months post-treatment, the mean score on the DCS subscale “effective decision-making” for the PDA-group was 10.33 (SD 12.85) compared with 14.92 (18.04) in the control group. Lower scores indicate more satisfaction with the treatment decision in hindsight. The mean difference in subscale score between groups with and without PDA is –4.59 (95% CI –9.14 to –0.05, p = 0.048) favouring the PDA group. Cohen’s effect size for the score on the “effective decision-making” subscale is 0.29.
| PDA group Mean (SD) | Control group Mean (SD) | Mean difference (PDA control) | Cohen’s effect size | p-value | |
| Subscale | 10.33 (12.85) | 14.92 (18.04) | –4.59 | 0.29 | 0.048 |
| Question 1 | – | – | –0.26 | 0.29 | 0.055 |
| Question 2 | – | – | –0.24 | 0.28 | 0.062 |
| Question 3 | – | – | –0.10 | 0.10 | 0.487 |
| The mean could not be calculated for the separate questions. The minimally relevant effect size (Cohen’s effect size) for the DCS scores on the effective decision-making subscale is 0.2–0.3 (14). SD: standard deviation; DCS: Decisional Conflict Scale. |
|||||
After adjustment for between-group differences in sex, age, study centre, educational level, having a BCC in the medical history, location and diameter of the sBCC, and baseline EuroQol-VAS score, the adjusted mean difference was –4.10 (95% CI –8.73 to 0.52, p = 0.082).
The first 2 questions were associated with a similar effect size favouring the PDA group: “I feel I have made an informed choice” (mean difference = –0.26, 95% CI –0.52–0.01, p = 0.055, Cohen’s d = 0.29) and “My decision shows what is important to me” (mean difference = –0.24, 95% CI –0.49–0.01, p = 0.062, Cohen’s d = 0.28), although the results were not statistically significant. With respect to the third question “I am satisfied with my decision”, the mean difference between the PDA and control group and effect size were smaller (mean difference = –0.10, 95% CI –0.38–0.18, p = 0.487, Cohen’s d = 0.10).
DISCUSSION
This prospective multicentre trial including patients with a newly diagnosed sBCC shows that patients who used a PDA seemed to choose non-invasive therapy more often compared with a control group, although this result was not statistically significant. Three months post-treatment, patients who used the PDA seemed more likely to feel like they had made an “effective decision”. Effect sizes were near 0.3, which is clinically relevant, but statistical significance was not reached.
In both groups, more than half of the patients chose surgical treatment. Former research also showed that many patients consider effectiveness the most important aspect of treatment (3). However, in the PDA group patients seemed to choose non-invasive treatment somewhat more often compared with the control group. Due to a lack of significance we could not confirm the hypothesis that well-informed patients, who used a PDA would more frequently choose non-invasive treatment options. Stacey et al. provided an extensive description of choices made by patients for multiple health-related decisions (4). Patients using a PDA less often chose elective surgery and testing in other medical fields. For example, patients who used a PDA less often chose to test prostate specific antigen (screening), more often decided to start medication for cardiovascular disease (prevention) instead of a wait-and-see policy (with more future risks), and less frequently chose to take antibiotics for upper respiratory infection (treatment) (4). The slight preference of patients in the PDA group for non-invasive treatment was not statistically significant. However, if patients in the PDA group chose non-invasive treatment more frequently, this might be a result of an improved estimation of benefits but also risks of treatments, and of an improved clarification of values. This would be in line with the results from the field testing of this PDA which showed that patients’ knowledge improved after using the PDA (6). Stacey et al. (4) also reported on studies that evaluated the accuracy of patients’ perceived risks and outcomes of treatments. Accuracy was defined as the percentage of patients whose judgements were in line with the available scientific evidence for the probabilities of these (risk) outcomes. A strong improvement was found; for every 1,000 patients who did not use a PDA, 269 were likely to accurately interpret treatment risks compared with 565 per 1,000 patients after using a PDA. Furthermore, it is known that most patients deem high efficacy the most important aspect of treatment (3). Possibly, due to elaborate value clarification, other treatment characteristics play a more important role in the decision-making process after using the PDA. This may guide more patients to choose non-invasive treatment as opposed to patients who did not use the PDA (3).
We found that sBCC patients using the PDA more often felt that they made an “effective decision” 3 months after treatment. Making an effective decision is defined as retrospectively being satisfied with the treatment decision and having the feeling they were well informed to make the decision (14). The observed effect sizes were near 0.3, which is considered clinically relevant (14). The results were not statistically significant, but the sample size enabled detection of an effect size ≥ 0.4 for the total DCS score and was too small to detect smaller effects with statistical significance. Nevertheless, these results might reflect the added value of the PDA to a conversation between patient and physician alone. This is in line with outcomes of a meta-analysis that reviewed the effect of PDAs based on the Ottawa Decision Support Framework (16). Ten trials showed that, when compared with usual care, patients who received a PDA had a reduced perception of ineffective decision-making (mean difference = −5.56; 95% CI −9.30 to −1.82).
After mutual adjustment, the odds ratios for tumour or patient characteristics of influence show that a positive history of BCC was associated with a significantly increased odds ratio indicating preference for non-invasive treatment over surgery (Table II). Patients with a history of BCC might be less impacted or stressed by receiving a skin cancer diagnosis compared with patients with a first BCC. A study investigating perceptions of patients with BCC showed that 36.1% experienced shock (trauma/stress) on the announcement of their diagnosis (17). Furthermore, almost half of those patients were scared of metastasis or mortality after the dermatologist used the word “cancer”. Experiencing stress and fright after a diagnosis of skin cancer was found not to be associated with a type of skin cancer, but with the word “cancer” itself (18). Compared with patients with a newly diagnosed BCC, patients with a history of BCC might be less shocked and thus more inclined to choose non-invasive treatment despite lower effectiveness.
There are some limitations to this study. First, the patients in the PDA group were included during the first stages of the COVID-19 pandemic, which means that more patients might have chosen non-invasive therapies (imiquimod and 5FU) to avoid additional hospital visits. Secondly, this study was powered to detect an effect size of 0.4 with regard to the total score on the DCS instead of the score on the subscale “effective decision-making”. The sample size was too small to detect significant between-group differences of 0.2–0.3 (14). Finally, the PDA group was given time to reflect on the decision and had a second conversation with their physician whereas the control group made the decision on first encounter. This could introduce some disparity.
Conclusion
Patients with an sBCC who used a PDA seemed more likely to prefer non-invasive therapy over surgery compared with a control group, but the result did not reach significance. Although non-significant, using a PDA had a clinically relevant effect on effective decision-making 3 months post-treatment, which may reflect the added value of the PDA.
ACKNOWLEDGEMENTS
IRB approval status: approved by METC azM/UM
REFERENCES
- Kim JYS, Kozlow JH, Mittal B, Moyer J, Olencki T, Rodgers P. Guidelines of care for the management of basal cell carcinoma. J Am Acad Dermatol 2018; 78: 540–559. https://doi.org/10.1016/j.jaad.2017.10.006
- Peris K, Fargnoli MC, Garbe C, Kaufmann R, Bastholt L, Seguin NB, et al. Diagnosis and treatment of basal cell carcinoma: European consensus-based interdisciplinary guidelines. Eur J Cancer 2019; 118: 10–34. https://doi.org/10.1016/j.ejca.2019.06.003
- Neal DE, Feit EM, Etzkorn JR. Patient preferences for the treatment of basal cell carcinoma: a mapping review of discrete choice experiments. Dermatol Surg 2018; 44: 1041–1049. https://doi.org/10.1097/DSS.0000000000001564
- Stacey D, Legare F, Lewis K, Barry MJ, Bennett CL, Eden KB, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev 2017; 4: CD001431. https://doi.org/10.1002/14651858.CD001431.pub5
- van Delft LCJ, Essers BAB, Nelemans PJ, Mosterd K, Kelleners-Smeets NWJ. Development of a patient decision aid for superficial basal cell carcinoma. Br J Dermatol 2021; 184: 744–746. https://doi.org/10.1111/bjd.19662
- van Delft LCJ, Essers BAB, Nelemans PJ, Mosterd K, van Winden MEC, Romaen IFL, et al. Effectiveness of a patient decision aid for patients with superficial basal cell carcinoma: a pre- and post-implementation study. Patient Educ Couns 2023; 115: 107907. https://doi.org/10.1016/j.pec.2023.107907
- Tan J, Linos E, Sendelweck MA, van Zuuren EJ, Ersser S, Dellavalle RP, et al. Shared decision making and patient decision aids in dermatology. Br J Dermatol 2016; 175: 1045–1048. https://doi.org/10.1111/bjd.14803
- Tan J, Wolfe B. Improved decisional conflict and preparedness for decision making using a patient decision aid for treatment selection in psoriasis: a pilot study. J Cutan Med Surg 2014; 18: 114–118. https://doi.org/10.2310/7750.2013.13113
- Arits AH, Mosterd K, Essers BA, Spoorenberg E, Sommer A, De Rooij MJ, et al. Photodynamic therapy versus topical imiquimod versus topical fluorouracil for treatment of superficial basal-cell carcinoma: a single blind, non-inferiority, randomised controlled trial. Lancet Oncol 2013; 14: 647–654. https://doi.org/10.1016/S1470-2045(13)70143-8
- Bath-Hextall F, Ozolins M, Armstrong SJ, Colver GB, Perkins W, Miller PS, et al. Surgical excision versus imiquimod 5% cream for nodular and superficial basal-cell carcinoma (SINS): a multicentre, non-inferiority, randomised controlled trial. Lancet Oncol 2014; 15: 96–105. https://doi.org/10.1016/S1470-2045(13)70530-8
- Thomson J, Hogan S, Leonardi-Bee J, Williams HC, Bath-Hextall FJ. Interventions for basal cell carcinoma: abridged Cochrane systematic review and GRADE assessments. Br J Dermatol 2021; 185: 499–511. https://doi.org/10.1111/bjd.19809
- Verkouteren JAC, Ramdas KHR, Wakkee M, Nijsten T. Epidemiology of basal cell carcinoma: scholarly review. Br J Dermatol 2017; 177: 359–372. https://doi.org/10.1111/bjd.15321
- Koedoot N, Molenaar S, Oosterveld P, Bakker P, de Graeff A, Nooy M, et al. The decisional conflict scale: further validation in two samples of Dutch oncology patients. Patient Educ Couns 2001; 45: 187–193. https://doi.org/10.1016/S0738-3991(01)00120-3
- O’Connor A. User manual: Decisional Conflict Scale 2010. Available from: https://decisionaid.ohri.ca/docs/develop/User_Manuals/UM_decisional_conflict.pdf
- Ravens-Sieberer U, Wille N, Badia X, Bonsel G, Burstrom K, Cavrini G, et al. Feasibility, reliability, and validity of the EQ-5D-Y: results from a multinational study. Qual Life Res 2010; 19: 887–897. https://doi.org/10.1007/s11136-010-9649-x
- Hoefel L, Lewis KB, O’Connor A, Stacey D. 20th Anniversary Update of the Ottawa Decision Support Framework: Part 2 Subanalysis of a systematic review of patient decision aids. Med Decis Making 2020; 40: 522–539. https://doi.org/10.1177/0272989X20924645
- Aymonier M, Taieb C, Corgibet F, Joly P, Sei JF, Chaussade V, et al. Patient perception of the diagnosis announcement and its impact on quality of life of patients with primary melanoma or basal cell carcinoma. Acta Derm Venereol 2022; 102: adv00717. https://doi.org/10.2340/actadv.v102.2217
- Khoshab N, Vaidya TS, Dusza S, Nehal KS, Lee EH. Factors contributing to cancer worry in the skin cancer population. J Am Acad Dermatol 2020; 83: 626–628. https://doi.org/10.1016/j.jaad.2019.09.068