SHORT COMMUNICATION
Distinct Impact of Phosphodiesterade-4 (PDE4) Inhibition in Two Pre-clinical Psoriasis Models
Sören DRÄGER1,2, Thorge MESTER1, Hermann TENOR3, Ralf J. LUDWIG1,2 and Katja BIEBER1
1Lübeck Institute of Experimental Dermatology, University of Lübeck, Lübeck, Germany, 2Department of Dermatology, Allergology, and Venereology, University Hospital Schleswig-Holstein (UKSH), Ratzeburger Allee 160, DE-23538 Lübeck, Germany, and 3Topadur Pharma AG, Schlieren, Switzerland. E-mail: soeren.draeger@uksh.de
Citation: Acta Derm Venereol 2025; 105: adv41972. DOI: https://doi.org/10.2340/actadv.v105.41972.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Sep 9, 2024. Accepted after revision: Mar 17, 2025. Published: Apr 7, 2025.
Competing interests and funding: RJL received funding from Topadur Pharma AG to investigate the impact of PDE4 inhibition in preclinical models of inflammatory skin diseases. HT is a full-time employee at TOPADUR Pharma AG.
This research was funded by the Cluster of Excellence “Precision Medicine in Chronic Inflammation” (EXC 2167) and the Research Training Group “Modulation of Autoimmunity” (GRK 1727), both from the Deutsche Forschungsgemeinschaft, the Schleswig-Holstein Excellence-Chair Program from the State of Schleswig Holstein, and an unrestricted research grant from Topadur Pharma.
INTRODUCTION
Psoriasis is a common disease, affecting around 2–3% of the population. While biologicals achieve PASI-75 responses above 80%, their high costs limit accessibility in many countries. For example, in Germany, annual costs are approximately €30,000 for bimekizumab (anti-IL17A/F), €27,000 for tildrakizumab (anti-IL-23), €12,000 for the TYK2 inhibitor deucravacitinib, and €6,000 for the PDE4 inhibitor apremilast (1), underscoring the substantial treatment expenses associated with these medications. In contrast, the phosphodiesterase 4 (PDE4) inhibitor roflumilast, used in chronic obstructive pulmonary disease (COPD), offers a more affordable alternative at treatments costs of approximately €1,000 per year, potentially expanding patient access and reducing healthcare costs. PDE4 is a cAMP hydrolysing phosphodiesterase involved in the signal transduction in many inflammatory cells orchestrating psoriasis. Low cAMP levels, as they may result from upregulated PDE4, favour the release of pro-inflammatory cytokines (2). Inhibiting PDE4 increases intracellular cAMP, reversing this process. In vitro, the PDE4 inhibitor roflumilast is more potent than apremilast reflected by an IC50 to inhibit PDE4 of 0.8 nM (2) and 7.4 nM (3), respectively. The superior potency of roflumilast compared with apremilast to inhibit PDE4 was translated into a comparably higher potency to augment cAMP in PGE2-stimulated peripheral blood mononuclear cells (4). Roflumilast, well established for treatment of severe COPD since 2011, was approved for the topical treatment of psoriasis by the FDA in July 2022. A Danish study showed that systemic roflumilast achieved a PASI-75 reduction in 35% of psoriasis patients at week 12, increasing to 44% by week 24 (5). Different animal models aid in understanding psoriasis pathogenesis and evaluating the potential efficacy of new treatments, though no single model encapsulates all disease aspects (6). In this study, we examined the efficacy of roflumilast in two commonly used psoriasis mouse models: topical Aldara® application and recombinant IL-23 injection. Both have histological and clinical commonalities with human psoriasis, e.g., upregulation of IL-17 and IL-23. Yet, in Aldara-induced psoriasiform dermatitis (AIPD), repeated topical application of Aldara®, containing a TLR7 ligand (Imiquimod) and isostearic acid, additionally exerts a strong systemic inflammatory response, exemplified by increased splenic mass (6, 7). A more subtle induction of psoriasis is achieved by repeated intradermal injections of recombinant murine IL-23, which lead to an initial IL-17 release by γδ-T cells subsequently amplified by macrophage recruitment (8). We aimed to investigate the impact of roflumilast treatment to further validate these pre-clinical model systems for the use of translational psoriasis research.
METHODS AND RESULTS
Animal experimentation was approved by the respective governmental administration (AZ 92-7/17), and performed by certified staff. All experiments were performed in mice of both sexes, aged between 7 and 11 weeks. The primary endpoint was clinical disease manifestation, expressed by the PASI score on day 5 (AIPD) or the ear thickness on day 16 (IL-23). A p-value less than 0.05 was considered statistically significant. The experiments were performed following established protocols (Fig. 1A, D) (9, 10). AIPD was induced by repetitive, daily topical application of Aldara® (Meda Pharmaceuticals, USA) from day 0–4 (7). IL-23 psoriasiform dermatitis was induced by repetitive intradermal injections of recombinant murine IL-23 every other day from day 0–15, as described (11). Mice were orally treated with roflumilast (5 mg/kg bodyweight) (Sigma-Aldrich, USA) dissolved in 0.8% methylcellulose once daily, beginning 1 day before application of Aldara® or IL-23. Mice treated with vehicle alone served as positive controls. Treatments were continued once daily throughout the experiment. H&E stainings were performed according to established procedures. Epidermal thickness was measured at 10 randomly chosen sites of each section using ImageJ software (https://imagej.net/ij/). Plasma concentrations of cytokines was measured using Luminex® xMAP® technology and performed by Eve Technologies Corporation (Calgary, Alberta, Canada). In the AIPD model, the disease score at the primary endpoint (day 5) measured 7.11 (± 0.68) in the vehicle group (Fig. 1B, C). A similar clinical disease severity was observed in mice treated with roflumilast. Here, the final disease score was 6.50 (± 1.02). Likewise, specific components of the PASI assessment – erythema, infiltration, and desquamation – were similar between the two groups. Concurrently, the degree of weight loss observed in this model was comparable between the mice treated with roflumilast and those administered the vehicle alone. In IL-23-induced psoriasiform dermatitis, the ear thickness measured 496.25 μm (± 53.59) in the control group. Roflumilast ameliorated the disease development, resulting in a significantly reduced ear thickness of 364.27 μm (± 28.73) on day 16 (Fig. 1E, F). Histologically, the epidermal thickness in control mice measured 20.18 μm (± 3.83). In comparison, roflumilast-treated mice showed a reduced mean thickness of 14.23 μm (± 1.53), but this reduction was not statistically significant. (Fig. 1G). The histological score index was 1.65 (± 0.35) in the control group and 1.16 (± 0.31) in the treatment group, also not reaching statistical significance (Fig. 1G). In plasma, concentrations of IL-17F, IL-22, and IL-33 were significantly elevated in the AIPD mouse model (Fig. S1).
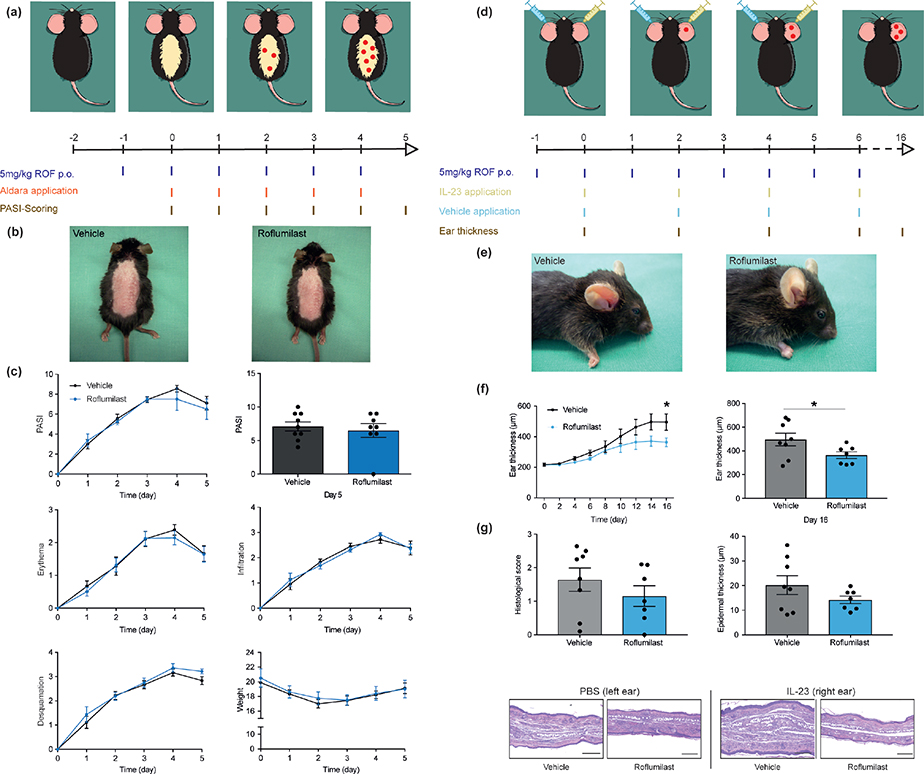
Fig. 1. Distinct clinical outcomes of PDE4 inhibitor roflumilast in Aldara® or interleukin (IL)-23-induced psoriasis mouse models. Aldara®-induced psoriasiform dermatitis (AIPD) is not alleviated by phsphodiesterase-4 inhibition with roflumilast. In contrast, psoriasiform dermatitis induced by recombinant murine IL-23 injection is significantly reduced with roflumilast treatment. (a) Schematic experimental setup of AIPD. Red dots indicate sites of psoriasis manifestation. (b) Representative clinical images of the respective groups in AIPD. (c) Psoriasis area and severity index (PASI) from days 0–5 and PASI score at the primary endpoint (day 5). Individual score values (erythema, infiltration, and desquamation) from day 0–5 and mean weight of the respective groups over time. (d) Schematic experimental setup of IL-23-induced psoriasiform dermatitis. (e) Representative clinical images of the respective groups in IL-23 induced psoriasiform dermatitis. (f) Ear thickness from day 0-16 in IL-23 induced psoriasiform dermatitis and ear thickness at the primary endpoint (day 16). (g) Epidermal thickness and semiquantitative histological score of samples obtained on day 16. Representative histological images of the respective groups. ((c) and (e–g): mean with SEM or scatter dot plot, mixed-effect analysis with Bonferroni correction).
DISCUSSION
The oral PDE4 inhibitor apremilast has been used to treat patient with psoriasis for over a decade. In 2022, the FDA approved roflumilast for the topical treatment of psoriasis. However, systemic (oral) roflumilast has only been approved for the treatment of severe COPD, and therefore has not been widely used in psoriasis. A recent Danish study suggests that systemic roflumilast may be more effective than apremilast (5), which may reflect the higher potency to inhibit PDE4 (4). Roflumilast has been infrequently studied in murine psoriasis models. Data with roflumilast in validated mouse disease models may allow cellular and molecular insights on the drugs’ mode of action to be obtained and, together with clinical findings, may encourage pivotal phase 3 clinical trials that could lead to the approval of this cost-effective treatment. For instance, Xu et al. (12) found that topical roflumilast application in the AIPD mouse model did not alter PASI scores or cAMP levels, whereas intraperitoneally applied apremilast (1 mg/kg) exerted a disease-modifying effect in AIPD (13). In contrast, we observed that oral roflumilast treatment did not result in any significant change in disease manifestation in the AIPD model. Given that different murine models replicate certain aspects of the human disease, using multiple models is beneficial for translational research. Hence, we also evaluated the impact of oral roflumilast in the IL23-induced mouse model of psoriasis. Here, disease severity was reduced and the pre-defined primary endpoint was met. Evaluating roflumilast in both AIPD and IL-23 models highlights differences in pathogenesis and offers more robust data. This points to inherent differences between the 2 models. First, Aldara® is not only a potent TLR7 agonist but also acts as a weak cAMP-PDE inhibitor (14). Therefore, its intrinsic PDE4 inhibitory activity may prevent the observation of any additional effects from “add-on” PDE4 inhibitors. Additionally, the robust activation of TLR7 by Aldara® results in a strong immune response, as evidenced by increased plasma concentrations of IL-17F, IL-22, and IL-33, as well as an increased splenic mass in this model (7). Consistent with this, our findings show that in the AIPD mouse model further PDE4 inhibition by roflumilast does not produce any amelioration of disease. In contrast, roflumilast-treated mice in the IL-23 model exhibited reduced disease severity. In this model, repeated injections of IL-23 stimulate T cells, specifically γδ-T cells, to secrete IL-17 and IL-22, which drive disease progression (15). T cell regulation is dependent on cAMP, with elevated levels exerting an inhibitory effect. By inhibiting PDE4, roflumilast prevents the hydrolysis of cAMP, leading to increased intracellular cAMP levels and thereby effectively ameliorating the disease. In summary, the distinct mechanistic pathways underlying disease induction are essential for accurately interpreting the observed results. Nevertheless, further studies dissecting psoriasis model differences are warranted. This study underlines that caution should be applied if research is based on single murine disease models, considering the different disease induction mechanisms. Finally, systemic (oral) application of roflumilast in psoriasis warrants further randomized controlled clinical trials and could emerge as a cost-effective and safe alternative treatment for psoriasis.
ACKNOWLEDGEMENTS
The authors would like to thank Ibrahim Osman Ibrahim and Saeedeh Ghorbanalipoor for assisting with the mouse experiments. ChatGPT 4o was used to enhance readability and language.
IRB approval status: Animal experimentation was approved by the respective governmental administration (AZ 92-7/17).
REFERENCES
- Pharmindex [Internet]. [cited 2024 Aug 12]. Available from: http://www.gelbe-liste.de
- Hatzelmann A, Schudt C. Anti-inflammatory and immunomodulatory potential of the novel PDE4 inhibitor roflumilast in vitro. J Pharmacol Exp Ther 2001; 297: 267–279. https://doi.org/10.1016/S0022-3565(24)29537-9
- Man H wah, Schafer P, Wong LM, Patterson RT, Corral LG, Raymon H, et al. Discovery of (S)-N-{2-[1-(3-Ethoxy-4-methoxy-(Apremilast ), a potent and orally active phosphodiesterase 4 and tumor necrosis factor-alpha inhibitor. J Med Chem 2009; 52: 1522–1524. https://doi.org/10.1021/jm900210d
- Walsh NM. Comparison of the modes of action of Apremilast and Roflumilast. Enlighten thesxes. Glasgow: University of Glasgow; 2015.
- Gyldenløve M, Meteran H, Sørensen JA, Fage S, Yao Y, Lindhardsen J, et al. Efficacy and safety of oral roflumilast for moderate-to-severe psoriasis-a randomized controlled trial (PSORRO). Lancet Reg Health – Eur 2023; 30: 100639. https://doi.org/10.1016/j.lanepe.2023.100639
- Swindell WR, Johnston A, Carbajal S, Han G, Wohn C, Lu J, et al. Genome-wide expression profiling of five mouse models identifies similarities and differences with human psoriasis. PLoS ONE 2011; 6: e18266. https://doi.org/10.1371/journal.pone.0018266
- Fits LVD, Mourits S, Voerman JSA, Kant M, Boon L, Laman JD, et al. Imiquimod-induced psoriasis-like skin inflammation in mice is mediated via the IL-23/IL-17 axis. J Immunol 2009; 182: 5836–5845. https://doi.org/10.4049/jimmunol.0802999
- Gauld SB, Gauvin D, Olson L, Leys L, Paulsboe S, Liu Z, et al. Mechanistic and pharmacological assessment of murine IL-23 mediated psoriasiform dermatitis: implications for drug discovery. J Dermatol Sci 2018; 92: 45–53. https://doi.org/10.1016/j.jdermsci.2018.08.001
- Bieber K, Bezdek S, Gupta Y, Vorobyev A, Sezin T, Gross N, et al. Forward genetics and functional analysis highlight Itga11 as a modulator of murine psoriasiform dermatitis. J Pathol 2023; 261: 184–197. https://doi.org/10.1002/path.6162
- Dräger S, Kalies K, Sidronio TB, Witte M, Ludwig RJ, Bieber K. Increased TREM-1 expression in inflamed skin has no functional impact on the pathogenesis of cutaneous disorders. J Dermatol Sci 2017; 88: 139–155. https://doi.org/10.1016/j.jdermsci.2017.05.016
- Chan JR, Blumenschein W, Murphy E, Diveu C, Wiekowski M, Abbondanzo S, et al. IL-23 stimulates epidermal hyperplasia via TNF and IL-20R2-dependent mechanisms with implications for psoriasis pathogenesis. J Exp Med 2006; 203: 2577–2587. https://doi.org/10.1084/jem.20060244
- Xu R, Feng S, Ao Z, Chen Y, Su C, Feng X, et al. Long-acting β2 adrenergic receptor agonist ameliorates imiquimod-induced psoriasis-like skin lesion by regulating keratinocyte proliferation and apoptosis. Front Pharmacol 2022; 13: 865715. https://doi.org/10.3389/fphar.2022.865715
- Uchida H, Kamata M, Shimizu T, Egawa S, Ito M, Takeshima R, et al. Apremilast downregulates interleukin-17 production and induces splenic regulatory B cells and regulatory T cells in imiquimod-induced psoriasiform dermatitis. J Dermatol Sci 2021; 104: 55–62. https://doi.org/10.1016/j.jdermsci.2021.08.001
- Ernst O, Failayev H, Athamna M, He H, Tsfadia Y, Zor T. A dual and conflicting role for imiquimod in inflammation: a TLR7 agonist and a cAMP phosphodiesterase inhibitor. Biochem Pharmacol 2020; 182: 114206. https://doi.org/10.1016/j.bcp.2020.114206
- Sutton CE, Lalor SJ, Sweeney CM, Brereton CF, Lavelle EC, Mills KHG. Interleukin-1 and IL-23 induce innate IL-17 production from γδ t cells, amplifying Th17 responses and autoimmunity. Immunity 2009; 31: 331–341. https://doi.org/10.1016/j.immuni.2009.08.001