ORIGINAL REPORT
Genetic Variants in the SCN9A Gene are Detected in a Minority of Erythromelalgia Patients
Mari Skylstad KVERNEBO1,2, Celene GRAYSON3, Ioannis M. STYLIANOU3, Virginia WOLOSHEN3, Christopher RADOMSKI3, Cato MØRK4 and Knut KVERNEBO5
1Department of Dermatology, Oslo University Hospital, Rikshospitalet, Oslo, Norway, 2Aleris Medical Center, Stømmen, Norway, 3Xenon Pharmaceuticals Inc., Burnaby, Canada, 4Akershus Dermatology Centre, Lørenskog, Norway, and 5Institute of Clinical Medicine, Faculty of Medicine, University of Oslo, Oslo, Norway
Gain-of-function variants in the voltage-gated sodium channel Nav1.7, encoded by the SCN9A gene, have previously been identified in patients with erythromelalgia, a clinical diagnosis defined by intermittent attacks of painful, hot, swollen, and red skin, predominantly involving the hands and feet. Symptoms are induced or aggravated by warming and relieved by cooling. In primary erythromelalgia there is no known underlying disease. This study investigated the frequency of SCN9A variants in a cohort of primary erythromelalgia patients collected at a single centre, and examined the clinical signs and symptoms associated with identified variants. One hundred patients with possible erythromelalgia were collected prospectively and evaluated by clinical examination. Thirty-five patients fulfilling the clinical criteria of primary erythromelalgia were screened for variants in SCN9A. Five were found to carry likely causal variants, including a variant found in 2 related individuals and a variant not previously described in patients with erythromelalgia. The clinical findings differed significantly between the patients. Overall, in this cohort only 4/34 (11.7%) of unrelated patients had erythromelalgia likely caused by gain-of-function variants in SCN9A. Variants in SCN9A are therefore likely to cause or contribute to primary erythromelalgia in only a small proportion of patients.
SIGNIFICANCE
Erythromelalgia is a condition that is characterized by marked redness, increased skin temperature, and burning pain in the hands and feet. The condition is classified into primary (inherited) and secondary erythromelalgia. The role of genetic mutations in primary erythromelalgia is not fully documented. We have studied variants in the NAV1.7 protein, which is encoded by the SCN9A gene. The NAV1.7 protein is believed to have an important role in amplifying pain signals. A small number of the examined patients had mutations in this gene that could explain their erythromelalgia condition.
Key words: aetiology; genetics; NAV1.7 Voltage Gated Sodium Channel; primary erythromelalgia.
Citation: Acta Derm Venereol 2025; 105: adv42022. DOI: https://doi.org/10.2340/actadv.v105.42022.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Sep 16, 2024; Accepted after revision: Nov 26, 2024; Published: Jan 24, 2025.
Corr: Mari Skylstad Kvernebo, Aleris Strømmen, Støperiveien 5, NO-2010 Strømmen, Norway. E-mail: mari.kvernebo@gmail.com
Competing interests and funding: MK and KK are family related.
Other authors declare no other conflicts of interest.
INTRODUCTION
Erythromelalgia (EM) is a rare, debilitating, neurovascular disorder, defined by spontaneous or easily evoked attacks of burning pain accompanied by increased temperature, swelling, and redness of affected skin areas. The condition predominantly involves the skin on the hands and feet. Cooling relieves the burning pain, often induced or aggravated by warming, exercise, or wearing tight shoes and gloves. In primary EM there is no known underlying disease. The severity of symptoms varies from mild discomfort (most common) to disabling pain and eventually gangrene (1).
Patients with EM represent a heterogeneous group in relation to aetiology, severity, prognosis, and response to therapy (2–4). EM is either a primary condition, or secondary to a wide variety of conditions. The diagnosis is based on the medical history and clinical findings and there are no objective laboratory criteria. Regardless of aetiology, there is evidence of a final common pathway of pathogenesis, which includes maldistribution of skin perfusion with increased perfusion in the deep thermoregulatory plexus and a relative lack of papillary nutritive perfusion causing skin hypoxia (1, 5). The incidence of both primary and secondary EM has been estimated to range from 0.36 to 1.3 per 100,000 persons (6, 7), and the prevalence estimates range from 2 to 15 per 100,000 (1, 8).
Primary EM was the first human disorder to be linked to genetic variants within the SCN9A gene encoding for Nav1.7, a voltage-gated sodium channel involved in nociception. Rare, heterozygous missense variants in SCN9A identified in EM patients have been demonstrated to cause a gain-of-function of Nav1.7 leading to nociceptive dysfunction in in vitro electrophysiology experiments (6, 9). Pathogenic variants in SCN9A have also been reported in several other pain-related conditions (10–12). In familial cases of EM, there can be considerable clinical heterogeneity between family members with the same variant in SCN9A, particularly regarding the severity and age of onset (13, 14). While the genetic evidence for variants n SCN9A causing EM is compelling, only a relatively small proportion of primary EM cases have been shown to have variants in this gene (10, 15, 16). As EM is a rare condition, publications on the underlying genetics of the condition are often based on relatively few examined cases. In this study we have examined the frequency of SCN9A variants in a cohort of 35 patients suffering from primary EM, collected at a single centre. We also explore the relationship between the clinical presentation of these patients and their SCN9A genotypes.
MATERIALS AND METHODS
Study cohort
Erythromelalgia (EM) is a condition with intermittent attacks of painful, hot, swollen, and red extremities. EM is defined by spontaneous or easily evoked attacks of burning pain accompanied by increased temperature, swelling, and redness of affected skin areas. Cooling relieves the burning pain, often induced or aggravated by warming and exercise. In primary EM there is no known underlying disease. The diagnosis is based solely on the history and clinical findings and is often under-recognized by physicians. In Norway, there is greater awareness of the condition due to a number of publications, lectures, and media presentations by our research group attached to the Oslo University Hospital (OUH), Norway. Over a period of 34 years we have collected a cohort of 272 patients suffering from EM (2), mostly referred from general practitioners and dermatologists.
Following a presentation of EM on the Norwegian Broadcasting Corporation (NBC) in March 2014 (https://www.nrk.no/livsstil/fotter-som-brenner-1.11636326), individuals with “burning feet” were invited to respond to an e-mail address. Five hundred and twenty-nine respondents were invited to complete a questionnaire regarding their EM symptomatology. Of the 125 subjects who completed the questionnaire, 100 subjects with possible EM were evaluated at our clinic. Standard biochemical tests including full blood count with white cell differential count, level of blood sugar, antinuclear antibody, and relevant rheumatologic testing (17) were performed for all participants in order to exclude cases of secondary EM. Chest X-rays or CT scans were taken to exclude lung disease (n = 12). Small-fibre neurography was performed in a subset of 8 cases with symptoms suggestive of small-fibre neuropathy (i.e., numbness, tingling or, allodynia).
Sequencing of SCN9A
EDTA blood (20 ml) was collected and stored at –70 °C. Genomic DNA was extracted from whole blood using the PureGene DNA extraction kit (Qiagen, Redwood City, CA, USA). Whole genome sequencing was performed by Macrogen Inc. (Seoul, South Korea) by generating paired-end (2 × 150 bp) sequence reads using the Illumina HiSeq X Ten platform (https://www.illumina.com/). For all samples the entire SCN9A gene including introns, exons, and UTRs was captured at mean depth of > 30X.
Reads were aligned to UCSC Genome Browser build hg19 (https://genome.ucsc.edu/) with the Burrows-Wheeler Aligner (BWA-MEM v.0.7.12; https://bio-bwa.sourceforge.net/), and variants were called with the Genome Analysis Toolkit HaplotypeCaller (v.2.3; https://gatk.broadinstitute.org/hc/en-us/articles/360037225632-HaplotypeCaller) and annotated using Variant Effect Predictor (VEP-75; https://www.ensembl.org/info/docs/tools/vep/index.html). Visual validation of coverage, sequence quality, alignment, and variant calling was performed using the Integrative Genomics Viewer (https://igv.org/).
All SCN9A rare coding variants with a minor allele frequency (MAF) of less than 0.01 that were identified by next-generation sequencing were confirmed by Sanger sequencing using standard protocols. Briefly, oligonucleotide primers were designed to capture 200–300 bp of unique sequence flanking the target variant. Amplicons were sequenced on an ABI 3730XL DNA sequencer (Beckman Genomics, Danvers, MA, USA). Sequences were analysed using Sequencher 5.0 software (Gene Codes, Ann Arbor, MI, USA).
RESULTS
Patient characteristics
The diagnosis of primary EM was confirmed in 47 of 100 patients evaluated at our clinic. The remaining 53 individuals did not meet the diagnostic criteria. The study population showed large heterogeneity with regard to age at onset and severity of symptoms. Thirty-five predominantly Caucasian patients with primary EM consented to participate in the genetic screening, including 27 females and 8 males, with a mean age of 46.1 years (range 23–78 years) (Fig. 1).
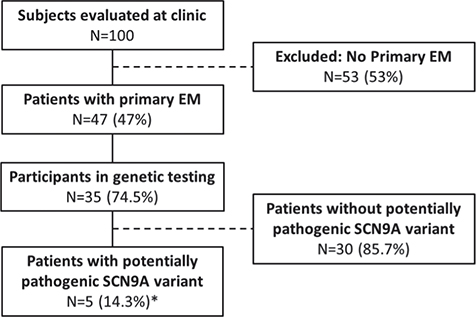
Fig. 1. Patients evaluated for primary EM at Oslo University Hospital and analysed for potentially pathogenic variants in SCN9A. Genetic screening of SCN9A variants was performed using whole genome sequencing. *Two patients with variants were a mother and daughter.
Genetic screening of SCN9A
Of the 35 patients screened, 15 (2 males and 13 females) had coding variants identified in the SCN9A gene (Table I). Five of the 15 patients with a variant in SCN9A reported a family history of EM. Two of these variants (I228M, I848T) have been previously described as pathogenic in patients with EM and 1 variant (V1820F) has not been previously reported in patients with EM. In addition, 3 common coding variants were also observed among the 35 patients: P610T, R1110Q, and W1150R, which were observed in 2, 1, and 7 patients respectively. Based on the observed rate of how often these variants occur in the general population without EM, none of these common variants occurred in the EM cohort more frequently than was expected by chance.
| Subject, sex | Age, years | Family history | Onset of EM symptoms | Cooling category | VAS | Nav1.7 variant | MAF (%) | |
| 14 (F) | 77 | Yes | Childhood | 3 | 0–8 | I228M | 0 | Likely causal |
| 24 (F) | 73 | No | 30 years of age | 1–2 | 0–4 | I228M | 0 | |
| 01 (F)* | 58 | Yes | Early childhood | 8 | 10 | I848T | 0 | |
| 02 (F)* | 34 | Yes | Early childhood | 3 | 4–7 | I848T | 0 | |
| 27 (F) | 41 | Yes | Late teens | 3 | 0–7 | V1820F | 0.000014 | |
| 19 (M) | 37 | No | 30 years of age | 4 | 4–9 | P610T | 0.024 | Common variants |
| 28 (F) | 28 | No | Childhood | 2–3 | 0–8 | P610T | 0.024 | |
| 26 (F) | 34 | No | Early teens | 1 | 0–5 | R1110Q | 0.020 | |
| 02 (F)* | 34 | Yes | Childhood | 3 | 4–7 | W1150R | 0.127 | |
| 18 (M) | 38 | No | Unknown | W1150R | 0.127 | |||
| 20 (F) | 46 | No | 33 years of age | W1150R | 0.127 | |||
| 26 (F) | 33 | No | 20 years of age | W1150R | 0.127 | |||
| 30 (F) | 35 | No | 32 years of age | W1150R | 0.127 | |||
| 33 (F) | 44 | No | 42 years of age | W1150R | 0.127 | |||
| 37 (F) | 46 | No | 45 years of age | W1150R | 0.127 | |||
| MAF: Minor allele frequencies as listed in the gnomAD database v2.1.1 (http://gnomad.broadinstitute.org). Age: In years at examination. Cooling category: According to an eight-category cooling scale describing the extent of cooling as a sign of disease activity during the last week before examination (Kalgaard et al. 1997 [2]). VAS: Ten-category scale of intensity was used to assess the minimal and maximal level of pain (Hawker et al. 2011 [32]). *Carriers of the I848T variant are a mother and daughter. | ||||||||
I228M variant. The I228M variant in the SCN9A gene is suspected to be causal for EM and has been previously described in patients suffering from EM and small fibre neuropathy (19–21). This variant was identified in 2 unrelated female patients (Subjects 14 and 24) in this study.
I848T variant. Two related patients (mother and daughter) had an I848T variant in the SCN9A gene (Subjects 01 and 02) and have been described previously (1, 22). The I848T variant is typically associated with early-onset EM and is the most common causal variant associated with EM (22–24).
V1820F variant. The variant V1820F has not been previously reported in EM, but was identified in 1 patient (Subject 27). This variant is likely to be causative or contributing to EM in this patient due to the rarity of the variant in the general population, and predictions from in silico algorithms.
R1110Q variant. The R1110Q genetic variant was found in 1 patient (Subject 26).
P610T variant. Two patients (Subjects 19 and 28) had the P610T variant in the SCN9A gene.
W1150R variant. Seven patients were found to be heterozygous carriers of the W1150R variant in the SCN9A gene. Based on the allele frequency of this variant (0.127), we expected to see approximately 8.9 alleles by chance. The variant is therefore considered to be both common and not enriched in EM patients, and is therefore unlikely to cause or contribute to EM.
Appendix S1 provides detailed description of medical history and phenotypes for different mutations within the SCN9A gene.
DISCUSSION
In this cohort of 47 patients with primary EM, 35 patients consented to participate in genetic testing for variants in the SCN9A gene. Five patients had variants likely to be causative for EM. Excluding 1 of the relatives of these carriers (carriers of I848T were mother–daughter), this represents 4 proband cases in 34 unrelated subjects, therefore 11.7% of EM cases in this cohort can be explained by likely causal variants in SCN9A.
Ten further subjects were carriers of more common coding variants, none of which appear to be enriched in our EM patients relative to the expected allele frequencies of those variants in non-EM populations.
Selection and population
The majority of patients in this study were recruited by self-referrals after a television presentation. EM is described in all age groups, but all participants in this study were adults and Caucasians, reflecting the Norwegian population.
In the present cohort female EM sufferers were dominant. Previous reports have also shown a female majority among primary EM patients (2). The patients with variants thought to be causal for EM (I484T and V1820F) all describe heredity of EM, through only female family members. One of the 2 patients with I228M variant, which is suspected to be causal of EM, also describes her mother as having had EM symptoms.
All female patients had a gradual onset of symptoms, in contrast to the only male participant who could specify the exact month when symptoms started at the age of 30.
The mother and daughter with the I848T variant have constant symptoms with fluctuating intensity. All other patients describe intermittent EM symptoms. For some periods they are free from pain, while during attacks they may feel intense burning pain and needs to cool affected extremities.
I848T variant
The mother and daughter with I848T variant have previously been reported in the literature (22). This variant is thought to cause hyper-excitability and may lead to premature depolarization of the neuronal cell membrane, lowering the threshold for activation of other sodium channels located in the vicinity (10).
V1820F variant
The V1820F variant in Nav1.7, encoded by the SCN9A gene, has not previously been described. This amino acid residue is located in the C terminus intracellular part of the protein, which is not typically associated with EM. However, it is most probably causative or contributing to EM, based on its high conservation across all human voltage-gated sodium channels and in silico predictions.
The SCN9A gene codes for the sodium voltage-gates channel Nav1.7 and gain of function variants have been associated with pain disorders such as EM, paroxysmal extreme pain disorder (PEPD), and small-fibre neuropathy. These 3 disorders are categorized as painful neuropathies and may share overlapping symptoms (25). Previous reports on PEPD describe this as a very rare condition with onset in the neonatal period or infancy, with persistence throughout life. PEPD is characterized by attacks of excruciating deep burning pain, often in the rectal, ocular, or mandibular areas. Autonomic manifestations predominate initially, with skin flushing in all and harlequin colour change and tonic attacks in most. Dramatic syncopes have been described (26). The V1820F variant has not previously been described to be associated with EM or PEPD. Our patient has symptoms that resemble PEPD as well as EM. In addition to burning pain from the hands and feet, she describes rectal and jaw pain, but does not recall pain attacks as a child, which most PEPD patients do. Flushing in affected areas is not observed. She has fainted during rectal pain attacks on 2 occasions. She also described continuous vestibular pain over a period of 2 years, a symptom that is not connected to PEPD in the literature. Her pain symptoms may be an expression of dysfunctional neurological regulation.
I228M variant
The I228M variant has been described in patients with small-fibre neuropathy and EM. One of the 2 participants with an I228M variant has axonal neuropathy according to neurography examination. The other has not been examined for neuropathy.
This variant has been known to result in reduced length of neurites from neurons with the I228M variant in the Nav1.7 channel (27). The I228M variant has also been shown to have impaired slow-inactivation, and hyper-excitability in both trigeminal ganglion and dorsal root ganglion neurons (20).
The 2 patients with I228M variants describe, in contrast to the other patients in this study, worsening of EM symptoms when drinking alcohol, which may underline that these patients are sensitive to neuroactive substances. One of these patients experiences pain relief from using lidocaine patches, whereas the other patient experiences relief with gabapentin. Both lidocaine and gabapentin have direct effects on nerve impulse transmission because lidocaine inhibits such impulses and gabapentin is thought to reduce excitatory neurotransmitters within the CNS (28, 29).
Remarkably, these 2 patients have been active athletes all their lives, in contrast to most EM patients, who usually provoke symptoms through activity. One of the 2 patients in this study experienced a late onset of EM symptoms in her early thirties. This concurs with a previous report that refers to late onset of EM with this variant (22).
R1110Q and P610T variants
The P610T allele occurs at a rate of 0.025 in the general population, and therefore we expected to see ~1.75 individuals carrying this variant by chance. Similar to the R1110Q, the variant is therefore considered to be both common and not enriched in EM patients, and is therefore unlikely to cause or contribute to EM.
The R1110Q variant has an allele frequency of 0.02 in the general population and based on 35 sequenced patients (70 alleles) we expected this variant to be present in ~1.4 patients by chance. The variant is therefore considered to be both common and not enriched in EM patients and is therefore unlikely to cause or contribute to EM.
The P610T variant in the SCN9A gene is a variant of unknown significance. One study reports a prevalence of P610T of 10 out of 210 control Caucasian chromosomes (30). The same study states that the P610T is shared by the proband and an unaffected, but not an affected sibling. The limited number of reports on this specific variant makes it difficult to assess the true prevalence. Probably the variant itself is too common to be causal.
Both the patients with the P610T variant had elevated blood sugar values and insulin resistance at a young age. Diabetes is known to be a separate cause for neuropathy but is seldom a cause of EM. Both patients also suffer from recurrent depressive episodes, which could theoretically be linked to a nerve dysfunction.
The aetiology of EM has been debated for a number of years. Some authors have proposed that most cases of EM are caused by haematological conditions (31). Others have argued that the condition is caused by variants and accompanying dysfunction in autonomous nerves (25). In previous publications we have argued that EM is not a separate disease entity, but a symptom complex caused by dysregulation of microvascular perfusion in affected skin (1, 32). The dysregulation causes maldistribution of perfusion with increased thermoregulatory flow in the deep skin plexus (arterio-venous shunting), and with a relative reduction of nutritive perfusion in papillary capillaries, causing sub-epidermal areas with hypoxia. Such maldistribution can be caused by (i) autonomous nerve dysfunction secondary to variants in SCN9A, thin fibre neuropathy, diabetes, nerve injury etc.; (ii) haematological conditions such as polycythaemia and leukaemia affecting hemorheology; (iii) Pathological blood–tissue diffusion barrier (e.g., diabetes) or (iv) drugs or other chemical substances that affect regulation of microvascular perfusion.
In summary, 35 patients with primary EM were screen-ed for variants in SCN9A. Five individuals were found to carry variants likely to cause EM, including 1e novel variant and a variant found in 2 related individuals. Overall, 4/34 (11.7%) unrelated individuals studied had EM likely caused by gain-of-function variants in the Nav1.7. The results show that variants in SCN9A are likely to cause or contribute to primary EM in a relatively small proportion of patients.
ACKNOWLEDGEMENT
IRB approval status: Biobanc approved by the Norwegian Directorate of Health, Regional Ethical Committee Sør-Øst D, University of Oslo, Norway, 13 June 2008 (S-08433d, 2008/10617). Studt Langtidsoppflging av pasienter med erythromelalgia approved by Regional Committee Sør-Øst, University of Oslo, Norway, 18 November 2015 (2015/183).
REFERENCES
- Kvernebo K. Erythromelalgia: a condition caused by microvascular arteriovenous shunting. VASA 1998; 51.
- Kalgaard OM, Seem E, Kvernebo K. Erythromelalgia: a clinical study of 87 cases. J Intern Med 1997; 242: 191–197. https://doi.org/10.1046/j.1365-2796.1997.00185.x
- Davis MP, O’Fallon W, Rogers IR, Rooke TW. Natural history of erythromelalgia: presentation and outcome in 168 patients. Arch Dermatol 2000; 136: 330–336. https://doi.org/10.1001/archderm.136.3.330
- Mork C, Kvernebo K. Erythromelalgia – a mysterious condition? Arch Dermatol 2000; 136: 406–409. https://doi.org/10.1001/archderm.136.3.406
- Mork C, Asker CL, Salerud EG, Kvernebo K. Microvascular arteriovenous shunting is a probable pathogenetic mechanism in erythromelalgia. J Invest Dermatol 2000; 114: 643–646. https://doi.org/10.1046/j.1523-1747.2000.00944.x
- Alhadad A, Wollmer P, Svensson A, Eriksson KF. Erythromelalgia: incidence and clinical experience in a single centre in Sweden. Vasa 2012; 41: 43–48. https://doi.org/10.1024/0301-1526/a000162
- Reed KB, Davis MD. Incidence of erythromelalgia: a population-based study in Olmsted County, Minnesota. J Eur Acad Dermatol Venereol 2009; 23: 13–15. https://doi.org/10.1111/j.1468-3083.2008.02938.x
- Friberg D, Chen T, Tarr G, van Rij A. Erythromelalgia? A clinical study of people who experience red, hot, painful feet in the community. Int J Vasc Med 2013; 2013: 864961. https://doi.org/10.1155/2013/864961
- Yang Y, Wang Y, Li S, Xu Z, Li H, Ma L, et al. Mutations in SCN9A, encoding a sodium channel alpha subunit, in patients with primary erythermalgia. J Med Genet 2004; 41: 171–174. https://doi.org/10.1136/jmg.2003.012153
- Drenth JP, Te Morsche RH, Mansour S, Mortimer PS. Primary erythermalgia as a sodium channelopathy: screening for SCN9A mutations: exclusion of a causal role of SCN10A and SCN11A. Arch Dermatol 2008; 144: 320–324. https://doi.org/10.1001/archderm.144.3.320
- Klein CJ, Wu Y, Kilfoyle DH, Sandroni P, Davis MD, Gavrilova RH, et al. Infrequent SCN9A mutations in congenital insensitivity to pain and erythromelalgia. J Neurol Neurosurg Psychiatry 2013; 84: 386–391. https://doi.org/10.1136/jnnp-2012-303719
- McDonnell A, Schulman B, Ali Z, Dib-Hajj SD, Brock F, Cobain S, et al. Inherited erythromelalgia due to mutations in SCN9A: natural history, clinical phenotype and somatosensory profile. Brain 2016; 139: 1052–1065. https://doi.org/10.1093/brain/aww007
- Dib-Hajj SD, Cummins TR, Black JA, Waxman SG. Sodium channels in normal and pathological pain. Annu Rev Neurosci 2010; 33: 325–347. https://doi.org/10.1146/annurev-neuro-060909-153234
- Goldberg YP, Price N, Namdari R, Cohen CJ, Lamers MH, Winters C, et al. Treatment of Na(v)1.7-mediated pain in inherited erythromelalgia using a novel sodium channel blocker. Pain 2012; 153: 80–85. https://doi.org/10.1016/j.pain.2011.09.008
- Burns TM, Te Morsche RH, Jansen JB, Drenth JP. Genetic heterogeneity and exclusion of a modifying locus at 2q in a family with autosomal dominant primary erythermalgia. Br J Dermatol 2005; 153: 174–177. https://doi.org/10.1111/j.1365-2133.2005.06441.x
- Zhang Z, Schmelz M, Segerdahl M, Quiding H, Centerholt C, Jureus A, et al. Exonic mutations in SCN9A (NaV1.7) are found in a minority of patients with erythromelalgia. Scand J Pain 2014; 5: 217–225. https://doi.org/10.1016/j.sjpain.2014.09.002
- Faber CG. Gain of function NaV1.7 mutations in idiopathic small fiber neuropathy. Ann Neurol 2012: 71: 26–39. https://doi.org/10.1002/ana.22485
- Estacion M, Han C, Choi JS, Hoeijmakers JG, Lauria G, Drenth JP, et al. Intra- and interfamily phenotypic diversity in pain syndromes associated with a gain-of-function variant of NaV1.7. Mol Pain 2011; 7: 92. https://doi.org/10.1186/1744-8069-7-92
- Eijkenboom I, Sopacua M, Hoeijmakers JGJ, de Greef BTA, Lindsey P, Almomani R, et al. Yield of peripheral sodium channels gene screening in pure small fibre neuropathy. J Neurol Neurosurg Psychiatry 2019; 90: 342–352. https://doi.org/10.1136/jnnp-2018-319042
- Namer B, Orstavik K, Schmidt R, Kleggetveit IP, Weidner C, Mork C, et al. Specific changes in conduction velocity recovery cycles of single nociceptors in a patient with erythromelalgia with the I848T gain-of-function mutation of Nav1.7. Pain 2015; 156: 1637–1646. https://doi.org/10.1097/j.pain.0000000000000229
- Han C, Dib-Hajj SD, Lin Z, Li Y, Eastman EM, Tyrrell L, et al. Early- and late-onset inherited erythromelalgia: genotype–phenotype correlation. Brain 2009; 132: 1711–1722. https://doi.org/10.1093/brain/awp078
- Wu MT, Huang PY, Yen CT, Chen CC, Lee MJ. A novel SCN9A mutation responsible for primary erythromelalgia and is resistant to the treatment of sodium channel blockers. PloS One 2013; 8: e55212. https://doi.org/10.1371/journal.pone.0055212
- Brouwer BA, Merkies IS, Gerrits MM, Waxman SG, Hoeijmakers JG, Faber CG. Painful neuropathies: the emerging role of sodium channelopathies. J Peripher Nerv Syst 2014; 19: 53–65. https://doi.org/10.1111/jns5.12071
- Fertleman CR, Ferrie CD, Aicardi J, Bednarek NA, Eeg-Olofsson O, Elmslie FV, et al. Paroxysmal extreme pain disorder (previously familial rectal pain syndrome). Neurology 2007; 69: 586–595. https://doi.org/10.1212/01.wnl.0000268065.16865.5f
- Persson AK, Liu S, Faber CG, Merkies IS, Black JA, Waxman SG. Neuropathy-associated Nav1.7 variant I228M impairs integrity of dorsal root ganglion neuron axons. Ann Neurol 2013; 73: 140–145. https://doi.org/10.1002/ana.23725
- Sills GJ. The mechanisms of action of gabapentin and pregabalin. Curr Opin Pharmacol 2006; 6: 108–113. https://doi.org/10.1016/j.coph.2005.11.003
- Derry S, Wiffen PJ, Moore RA, Quinlan J. Topical lidocaine for neuropathic pain in adults. Cochrane Database Syst Rev 2014: 2014: CD010958. https://doi.org/10.1002/14651858.CD010958.pub2
- Samuels ME, te Morsche RH, Lynch ME, Drenth JP. Compound heterozygosity in sodium channel Nav1.7 in a family with hereditary erythermalgia. Mol Pain 2008; 4: 21. https://doi.org/10.1186/1744-8069-4-21
- Michiels JJ, Drenth JP, Van Genderen PJ. Classification and diagnosis of erythromelalgia and erythermalgia. Int J Dermatol 1995; 34: 97–100. https://doi.org/10.1111/j.1365-4362.1995.tb03587.x
- Mork C, Kvernebo K, Asker CL, Salerud EG. Reduced skin capillary density during attacks of erythromelalgia implies arteriovenous shunting as pathogenetic mechanism. J Invest Dermatol 2002; 119: 949–953. https://doi.org/10.1046/j.1523-1747.2002.00218.x
- Lebwohl M, Heymann WR, Berth-Jones J, Coulson I. Treatment of skin disease: comprehensive therapeutic strategies. 4th ed. Edinburgh: Saunders; 2014.
- Hawker GA, Mian S, Kendzerska T, French M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res (Hoboken) 2011; 63: S240–S252. https://doi.org/10.1002/acr.20543