QUIZ SECTION
Asymptomatic Annular Lesions in a 54-year-old Woman: A Quiz
Vincent KIMPE1*, Sébastien MENZINGER1,2, Gürkan KAYA1,2 and Yassaman ALIPOUR TEHRANY1
1Department of Dermatology, and 2Department of Clinical Pathology, University Hospital of Geneva, Geneva, Switzerland. *E-mail: vincent.kimpe@hug.ch
Citation: Acta Derm Venereol 2024; 104: adv42156. DOI: https://doi.org/10.2340/actadv.v104.42156.
Copyright: © 2024 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Published: Nov 27, 2024
A 54-year-old female patient known to have gout presented to the dermatology clinic with lesions that had appeared approximately 2 months before on her upper chest, arms, and hands. The lesions were asymptomatic. The patient noted a centrifugal evolution during the first few weeks; the lesions then stabilized in size and appearance. There was no recent history of fever, weight loss, night sweats, or other systemic symptoms. Physical examination revealed annular plaques with a raised erythematous border and an atrophic, hypopigmented centre, distributed on the neck, chest, proximal arms, and hands (Fig. 1). The lower limbs were spared. Palpation of the lymph nodes was unremarkable, as was the rest of the clinical examination. Histopathological analysis of a skin biopsy showed a granulomatous infiltrate with many multinucleated giant cells in the superficial and mid-dermis associated with elastolysis and elastophagocytosis, and without necrobiosis, mucin deposits, or actinic elastosis (Fig. 2).

Fig. 1. Clinical presentation. Annular plaques with a raised erythematous rim, and an atrophic, hypopigmented centre, distributed on the chest.
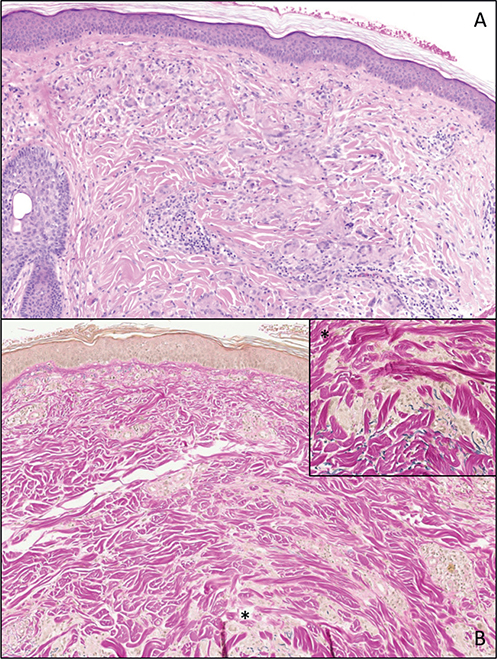
Fig. 2. Histopathological examination. Haematoxylin and eosin staining (original magnification 10×) (A): an interstitial granulomatous infiltrate with many giant cells is observed in the mid-dermis, associated with few lymphocytes; Miller staining (original magnification 10×) (B): Complete loss of the elastic network in the mid-dermis, associated with the fragmentation (elastolysis) and engulfment of the elastic fibres by giant multinucleated cells (elastophagocytosis) (inset: higher magnification 20× of the zone indicated *).
What is your diagnosis?
Differential diagnosis 1: Granuloma annulare
Differential diagnosis 2: Tinea corporis
Differential diagnosis 3: Lupus erythematosus
Differential diagnosis 4: Annular elastolytic giant cell granuloma
See next page for answer.
ANSWERS TO QUIZ
Asymptomatic Annular Lesions in a 54-year-old Woman: A Commentary
Diagnosis: Annular elastolytic giant cell granuloma
Annular elastolytic giant cell granuloma (AEGCG) is a non-infectious granulomatous skin disease and a distinctive clinico-pathological entity, which must be distinguished from actinic granuloma (AG) and granuloma annulare (GA). The descriptive term AEGCG was first used by Hanke et al. in 1979 (1) based on very similar histopathological reports by O’Brien in 1975 (2), who had coined the aetiological term AG. The latter attributed the pathogenesis of AG to actinic skin damage, i.e., chronic exposure to ultraviolet (UV) irradiation, whereas Hanke et al. did not consider actinic elastosis to be an obligatory constituent of AEGCG (3). The clinical presentation of AEGCG is characterized by asymptomatic annular lesions, a few centimetres in diameter, with erythematous raised rim and hypopigmented centre, on sun-exposed or non-sun-exposed areas, usually in middle-aged women (3). AG lesions are clinically very similar to those of AEGCG, but present only on sun-exposed skin and can be linked to photo-exacerbation (4). In comparison, GA has been recognized as a distinct entity, and typically presents as localized or generalized, skin-coloured, red, yellow, or tan dermal papules, arranged or coalescing in reticulate, arciform, or annular patterns, usually on the extremities. From a histopathological point of view, AEGCG presents as an interstitial granulomatous infiltrate with many giant multinucleated cells showing elastophagocytosis and a distinct loss of elastic tissue. Palisading of histiocytes is either absent or minimal, and necrobiosis and mucin deposits are not classical features of this condition. The histological features of AG are relatively similar except for the presence of actinic elastosis. GA, on the other hand, is characterized by a central area of necrobiosis of collagen with mucin deposits, surrounded by a palisade of histiocytes with few giant multinucleated cells (3, 5, 6). Nevertheless, elastophagocytosis can also be observed in GA.
In a recent review of 105 cases of AEGCG, the most frequently associated systemic disease was diabetes mellitus (DM), in 10 patients. In other studies, up to 37–40% of patients with AEGCG have associated DM. Aso et al. postulate that structural damage to elastic fibres caused by hyperglycaemia may precipitate inflammatory responses involved in AEGCG (7, 8). AEGCG has also been associated with hematologic and solid malignancies such as acute myeloid leukaemia, T-cell lymphoma, gastric carcinoma, or prostate carcinoma. In 2 cases, AEGCG resolved with treatment of the malignancy, and in 1 of these AEGCG relapsed with recurrence of the malignancy (3, 7, 9). Gyldenløve et al. (10) hypothesize that AEGCG lesions are a paraneoplastic phenomenon through host defence against a tumour antigens mechanism. In our patient, we performed laboratory tests including complete blood count, renal function, and hepatic tests, Hb1Ac, rheumatoid factors, ANA, and protein electrophoresis, all of which were found to be within normal limits.
The natural course of AEGCG is chronic, with frequent cases of spontaneous resolution. Although level of evidence remains low, proposed treatments range from topical, intralesional, or systemic corticosteroids, phototherapy (narrowband UVB, psoralen–UVA, retinoids–psoralen–UVA), to topical calcineurin inhibitors, with generally good, reported results (3, 7). We initiated treatment with class IV topical corticosteroids with a favourable, albeit slow, resolution of the lesions.
References
- Hanke CW, Bailin PL, Roenigk HH. Annular elastolytic giant cell granuloma: a clinicopathologic study of five cases and a review of similar entities. J Am Acad Dermatol 1979; 1: 413–421. https://doi.org/10.1016/S0190-9622(79)70033-8
- O’Brien JP. Actinic granuloma: an annular connective tissue disorder affecting sun and heat-damaged (elastotic) skin. Arch Dermatol 1975; 111: 460–466. https://doi.org/10.1001/archderm.111.4.460
- Gutiérrez-González E, Pereiro M, Toribio J. Elastolytic actinic giant cell granuloma. Dermatol Clin 2015; 33: 331–341. https://doi.org/10.1016/j.det.2015.03.002
- Wee JS, Moosa Y, Misch K, Chong H, Natkunarajah J. Actinic granuloma: a history of photoexacerbation and the importance of a radial ‘three-zone’ biopsy. Clin Exp Dermatol 2013; 38: 219–221. https://doi.org/10.1111/j.1365-2230.2012.04451.x
- Muhlbauer JE. Granuloma annulare. J Am Acad Dermatol 1980; 3: 217–230. https://doi.org/10.1016/S0190-9622(80)80181-2
- Limas C. The spectrum of primary cutaneous elastolytic granulomas and their distinction from granuloma annulare: a clinicopathological analysis. Histopathology 2004; 44: 277–282. https://doi.org/10.1111/j.0309-0167.2004.01755.x
- Qian YT, Liu JW, Liu W, Chen T, Tan Y, Ma DL. A retrospective study of 105 patients with elastolytic giant cell granuloma and a proposal for a new clinical classification. Acta Derm Venereol 2022; 102: adv00684. https://doi.org/10.2340/actadv.v102.1985
- Aso Y, Izaki S, Teraki Y. Annular elastolytic giant cell granuloma associated with diabetes mellitus: a case report and review of the Japanese literature. Clin Exp Dermatol 2011; 36: 917–919. https://doi.org/10.1111/j.1365-2230.2011.04094.x
- Garg A, Kundu RV, Plotkin O, Aronson IK. Annular elastolytic giant cell granuloma heralding onset and recurrence of acute myelogenous leukemia. Arch Dermatol 2006; 142: 532. https://doi.org/10.1001/archderm.142.4.532
- Gyldenløve M, Faurschou A, Nielsen SL, Thyssen JP. Annular elastolytic giant cell granuloma in a patient with squamous cell carcinoma of the tonsil. JAAD Case Rep 2014; 1: 34–35. https://doi.org/10.1016/j.jdcr.2014.11.001