SHORT COMMUNICATION
Treatment of Moderate-to-severe Atopic Dermatitis with Upadacitinib: Results from an Interim Analysis of the TREATgermany Registry
Barbara KIND1#  , Luise HEINRICH1# , Thomas WERFEL2* , Jochen SCHMITT1* , Stephan WEIDINGER3* and the TREATgermany study group
, Luise HEINRICH1# , Thomas WERFEL2* , Jochen SCHMITT1* , Stephan WEIDINGER3* and the TREATgermany study group
1Center for Evidence-Based Healthcare, University Hospital Carl Gustav Carus and Carl Gustav Carus Faculty of Medicine, Technische Universitaet Dresden, Dresden, 2Department of Dermatology and Allergy, Hannover Medical School, Hannover, and 3Center for Inflammatory Skin Diseases, Department of Dermatology and Allergy, University Hospital Schleswig-Holstein, Campus Kiel, Kiel, Germany. E-mail: Barbara.Kind@ukdd.de. #Equally contributing first authors, *equally contributing senior authors.
Citation: Acta Derm Venereol 2025; 105: adv42206. DOI: https://doi.org/10.2340/actadv.v105.42206.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Oct 21, 2024; Accepted after revision: Apr 25, 2025. Published: May 21, 2025
Competing interests and funding: JS reports institutional grants for investigator-initiated research from the German Federal Joint Committee, German Ministry of Health, German Ministry of Research, European Union, German Federal State of Saxony, Novartis, Sanofi, ALK, and Pfizer. He participated in advisory board meetings as a paid consultant for Sanofi, Lilly, and ALK. SE has received institutional research grants from LEO Pharma, Pfizer, and Sanofi, and has performed consulting work and lectures for AbbVie, Almirall, Boehringer, Eli Lilly, Galderma, GSK, LEO Pharma, Pfizer, Sanofi, and Regeneron. TW has received honoraria for lectures or scientific advice on atopic dermatitis from AbbVie, Almirall, Galderma, Janssen/JNJ, LEO Pharma, Leti, Lilly, Novartis, Pfizer, and Regeneron/Sanofi. The other coauthors declared no conflicts of interest.
TREATgermany is an academic, investigator-initiated clinical disease registry that is financially supported by AbbVie Deutschland GmbH & Co. KG, Almirall Hermal GmbH, Galderma S.A., LEO Pharma GmbH, Lilly Deutschland GmbH, and Sanofi.
INTRODUCTION
The JAK1 inhibitor upadacitinib substantially extended the treatment options of moderate-to-severe AD. In clinical trials, upadacitinib demonstrated high efficacy, particularly at 30 mg daily, with rapid improvements within 12–16 weeks (1, 2). Unlike targeted biologics, upadacitinib offers broader immunomodulation but requires careful monitoring due to potential risks, especially in older patients or those with cardiovascular or malignancy risk factors (3–5). Common side effects include acne-like eruptions, respiratory infections, and viral skin infections (6). Evidence for upadacitinib generated in the context of everyday clinical care is limited. Initial studies suggest strong effectiveness and safety, even in difficult-to-treat cases (7, 8).
MATERIALS AND METHODS
The TREATgermany registry is investigating its use in daily practice. TREATgermany is one of the largest AD registries worldwide, currently comprising > 2,000 adult patients with moderate-to-severe AD eligible for or receiving systemic therapy (9, 10). Here, all adult patients enrolled in the registry who received upadacitinib until December 2023 were included. Alongside demographics, disease history, and adverse events, prospective patient and physician assessments of disease activity using validated instruments were analysed (10, 11).
RESULTS
A total of 97 patients (mean age 36.7 ± 14.2 years, 42.3% female) who had initiated upadacitinib during registry observation were eligible for this analysis (Fig. S1). Fifty-two of the 97 upadacitinib-treated patients (53.6%) displayed at least 1 of the risk factors defined by the Pharmacovigilance Risk Assessment Committee (PRAC) (12). Twenty-three (23.7%) were active smokers and 20 (20.6%) have smoked in the past. Four patients were older than 64 years and 18 patients had relevant comorbidities (hypertension n = 17, cardiac insufficiency n = 1). If ex-smokers are omitted, still 37 (38.1%) patients met at least 1 risk factor. The majority of patients treated with upadacitinib (70.1%, n = 68) had previously received other systemic therapies and 31 transitioned from a previous ongoing systemic therapy without wash-out.
Of the 97 patients with an upadacitinib initiation registry visit, 36 patients (37.1%) initially received 15 mg daily, while 61 (62.9%) started with 30 mg (Fig. 1). Logistic regression revealed that the odds of receiving the lower initial dose was 8 times higher for females (p = 0.0006). The odds of receiving a prescription for the lower dose were 84% (6 times) lower for a patient who was treated in a dermatology office compared with a patient being treated in a university special outpatient clinic (hospital) (p = 0.0041). There was no significant association of smoking or being an ex-smoker with the lower initial dose of upadacitinib.
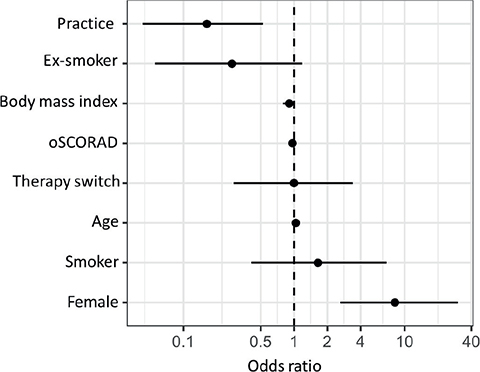
Fig. 1. What influenced the chance of being prescribed the lower initial dose of 15 mg upadacitinib per day? Odds ratio and 95% confidence interval of the variables: study site (doctor’s practice/clinic), smoking stopped (within 10 years and more than 10 years), body mass index, oSCORAD at upadacitinib start visit, direct switch to upadacitinib from another systemic therapy, active smoking, biological sex.
Among the 97 patients, 76 (78.4%) had at least 1 follow-up visit under upadacitinib treatment and were eligible for effectiveness analysis (Table SI). For better comparability of the continuous registry data with upadacitinib approval studies, 2 observation periods were defined: 3 months (13 ± 2 weeks, n = 43) and 6 months (26 ± 4 weeks, n = 35) of therapy (Table I).
At month 3, disease severity had improved in the vast majority of patients receiving upadacitinib (Table I). The EASI-50, EASI-75, EASI-90, and EASI-100 response rates were 81%, 63%, 40%, and 12%. An improvement at month 3 was also evident in POEM and DLQI.
The proportion of patients with little or uncontrolled disease (RECAP ≥ 12) decreased from 85.5% at therapy start to 21.4%, and 42.9% of the patients had completely or mostly controlled (RECAP ≤ 5) disease. The number of completely controlled weeks increased from 1.3 ± 2.4 to 6.3 ± 4.7 under upadacitinib treatment. There were also improvements in the symptoms, average skin pain, pruritus, and loss of sleep in the past 3 days as well as peak pruritus (PP-NRS) in the last 24 h, with pruritus being both the highest rated symptom and the symptom with the strongest (absolute) improvement. The proportion of patients who achieved a PP-NRS ≥ 4-point improvement from start was 52.4%. Patient satisfaction with medical treatment improved from 5.5 ± 2.8 to 7.6 ± 2.5.
Across all outcomes, a further improvement at month 6 was achieved compared with month 3 (Table I). Sleep loss reduced from 5.2 ± 3.3 to 1.2 ± 2.0. Patient satisfaction with medical treatment improved from 5.5 ± 2.8 to 8.4 ± 2.0. The proportion of patients who achieved a PP-NRS ≥ 4-point improvement from start was 60.6% at month 6. Likewise, 57.6% had completely or mostly controlled (RECAP ≤ 5) disease.
Safety data were analysed for all 76 patients with at least 1 follow-up visit while on upadacitinib therapy. A total of 15 adverse events (AEs) in 12 of these patients (15.8%) were reported. Most frequently reported AE were acne/acneiform skin lesions (5.2%, n = 4) and headache (2.6%, n = 2). Hyperlipidaemia, increase in liver values, worsening of atopic prurigo, herpes zoster, superinfection of the hand, impetigo contagiosa, and nausea/vomiting were each reported once.
The following AEs were reported once, but the causality was assessed as unlikely by the physician: recurrent styes, and fever. An additional 3 patients discontinued upadacitinib before the follow-up visit. In 2 of these patients an AE leading to treatment discontinuation was reported: 1 patient developed granulocytopenia, and another patient had recurrent cystitis and weight gain.
DISCUSSION
This first analysis of clinical effectiveness, safety, and utilization patterns of upadacitinib from the TREATgermany registry suggests robust clinical effectiveness with improvements in both objective and subjective disease activity measures, and favourable tolerability over 6 months of treatment. Clinical effectiveness was slightly lower than the efficacy observed in clinical trials, which may be explained by differences in the baseline characteristics of the study cohorts, divergent inclusion criteria, and no wash-out period for topical treatments prior to upadacitinib initiation. To reflect daily practice, patients with direct changes of systemic therapy were included in the analysis, which is another possible reason for lower EASI and itch response rates. The discontinuation rate (3 of 79 patients; 3.8%) until first follow-up visit was lower than in a recent small difficult-to-treat routine patient cohort (7). The proportion of patients with little or uncontrolled disease (RECAP ≥ 12) decreased from 85.5% at therapy start to 21.4% at month 3 and 18.2% at month 6. At months 3 and 6, 42.9% and 57.6% had completely or mostly controlled (RECAP ≤ 5) disease.
The majority of patients who received upadacitinib in TREATgermany had undergone other systemic treatments for AD in the past. This included dupilumab, which had been used in 34% of the patients prior to upadacitinib treatment. Upadacitinib-treated patients less often had comorbid asthma and rhinitis. A potential benefit of upadacitinib on comorbid respiratory disease is insufficiently investigated thus far, but limited data exist on the benefit of upadacitinib on atopic comorbidities (13). In total, 46.2% of patients treated with upadacitinib were current or past long-term smokers, i.e., had a risk factor for serious side effects with JAK inhibitors according to PRAC (14). Of those, 69.8% were initiated on a high upadacitinib dose. However, the majority of patients (75 of 97) were started on upadacitinib prior to the release of the PRAC recommendations in Germany, and up to now trial data have not indicated increased incidence rates for MACE, venous thromboembolism (VTE), and malignancies with JAK inhibitor use in AD (15).
In the patient population studied here for up to 6 months of treatment no SAE and a rather low number of AEs were reported. There were no reports of MACE, VTE, or malignancies. In conclusion, our data suggest that upadacitinib treatment is effective and well tolerated in adult patients with moderate-to-severe AD. Limitations of the presented analyses are the rather low sample size and short observation period. Future longer-term observations from TREATgermany and other registries will provide important additional insights into potential rare AEs, and how the PRAC recommendations impact routine use of JAK inhibitors in AD.
ACKNOWLEDGEMENTS
The authors gratefully acknowledge the substantial contributions made to this work by the participating patients, physicians, and clinical staff, the documentation team, and the TREATgermany Study Group as listed on treatgermany.org. They thank especially Thomas Birkner PhD, Dr. René Sachse, PD Dr. Stephan Traidl, Inken Harder, Dr. Tatjana Honstein, Dr. Dora Stölzl, PD Dr. Annice Heratizadeh, Prof. Dr. Matthias Augustin, Dr. Tho-mas Schaefer, Dr. Anne Bong, Dr. Susanne Abraham, PD Dr. Andreas Pinter, Dr. Jutta Ramaker-Brunke, and Dr. Michael Schulz-Kiesow for their substantial input.
Data availability statement: Data will be made available on reasonable request by the TREATgermany head office.
REFERENCES
- Werfel T, Heratizadeh A, Aberer W, Augustin M, Biedermann T, Bauer A, et al. S3 guideline Atopic dermatitis: Part 2 - Systemic treatment. J Dtsch Dermatol Ges 2024; 22: 307–320. https://doi.org/10.1111/ddg.15229
- Simpson EL, Papp KA, Blauvelt A, Chu CY, Hong HC, Katoh N, et al. Efficacy and safety of upadacitinib in patients with moderate to severe atopic dermatitis: analysis of follow-up data from the measure up 1 and measure up 2 randomized clinical trials. JAMA Dermatol 2022; 158: 404–413. https://doi.org/10.1001/jamadermatol.2022.0029
- Silverberg JI, Guttman-Yassky E, Simpson EL, Papp KA, Blauvelt A, Chu C-Y, et al. 502 - Efficacy and safety of upadacitinib through 140 weeks in adolescents and adults with moderate-to-severe atopic dermatitis: phase 3 randomized clinical trial results. Br J Dermatol 2024; 190: ii8–ii. https://doi.org/10.1093/bjd/ljad498.010
- Taylor PC, Laedermann C, Alten R, Feist E, Choy E, Haladyj E, et al. A JAK inhibitor for treatment of rheumatoid arthritis: the baricitinib experience. J Clin Med 2023; 12: 4527. https://doi.org/10.3390/jcm12134527
- Lancet Gastroenterology H. New restrictions on JAK inhibitors in the EU. Lancet Gastroenterol Hepatol 2023; 8: 1. https://doi.org/10.1016/S2468-1253(22)00397-1
- Guttman-Yassky E, Thyssen JP, Silverberg JI, Papp KA, Paller AS, Weidinger S, et al. Safety of upadacitinib in moderate-to-severe atopic dermatitis: an integrated analysis of phase 3 studies. J Allergy Clin Immunol 2023; 151: 172–181. https://doi.org/10.1016/j.jaci.2022.09.023
- Schlösser AR, Boeijink N, Olydam J, Nijsten TEC, Hijnen D. Upadacitinib treatment in a real-world difficult-to-treat atopic dermatitis patient cohort. J Eur Acad Dermatol Venereol 2024; 38: 384–392. https://doi.org/10.1111/jdv.19581
- Gargiulo L, Ibba L, Bianco M, Di Giulio S, Alfano A, Cascio Ingurgio R, et al. Upadacitinib 30 mg for the optimal management of moderate-to-severe atopic dermatitis: a 52-week single-center real-world study. J Dermatolog Treat 2024; 35: 2375102. https://doi.org/10.1080/09546634.2024.2375102
- Siegels D, Haufe E, Heinrich L, Werfel T, Weidinger S, Schmitt J, et al. Status report on the atopic dermatitis registry TREATgermany. Allergol Select 2021; 5: 274–286. https://doi.org/10.5414/ALX02262E
- Heratizadeh A, Haufe E, Stölzl D, Abraham S, Heinrich L, Kleinheinz A, et al. Baseline characteristics, disease severity and treatment history of patients with atopic dermatitis included in the German AD Registry TREATgermany. J Eur Acad Dermatol Venereol 2020; 34: 1263–1272. https://doi.org/10.1111/jdv.16078
- Traidl S, Heinrich L, Siegels D, Heratizadeh A, Kind B, Haufe E, et al. Treatment of moderate-to-severe atopic dermatitis with baricitinib: results from an interim analysis of the TREATgermany registry. J Eur Acad Dermatol Venereol 2024; 38: e887–e891. https://doi.org/10.1111/jdv.19979
- Risk of serious adverse effects with Janus kinase inhibitors. Drug Ther Bull 2023; 61: 35. https://doi.org/10.1136/dtb.2022.000078
- Gargiulo L, Ibba L, Piscazzi F, Amoruso F, Balato A, Barei F, et al. Upadacitinib improves symptoms of concomitant allergic rhinitis or allergic asthma in patients with severe atopic dermatitis: a 16-week multicentre retrospective study. J Eur Acad Dermatol Venereol 2024; 38: e743–e6. https://doi.org/10.1111/jdv.19862
- Ytterberg SR, Bhatt DL, Mikuls TR, Koch GG, Fleischmann R, Rivas JL, et al. Cardiovascular and cancer risk with tofacitinib in rheumatoid arthritis. N Engl J Med 2022; 386: 316–326. https://doi.org/10.1056/NEJMoa2109927
- Yoon S, Kim K, Shin K, Kim HS, Kim B, Kim MB, et al. The safety of systemic Janus kinase inhibitors in atopic dermatitis: a systematic review and meta-analysis of randomized controlled trials. J Eur Acad Dermatol Venereol 2024; 38: 52–61. https://doi.org/10.1111/jdv.19426