ORIGINAL REPORT
Type 2 Diabetes Impacts the Efficacy of Syphilis Treatment and is a Risk Factor for Late Syphilis: A Retrospective Cohort Study
Yijie TANG1#, Mengxiao WU2#, Wenwen XU1, Jiajie YU1, Dandan YANG1, Jiaqin ZHANG1, Lingyun SHEN1, Qinghui XIE1 and Qingqiong LUO1
1Department of Clinical Laboratory Medicine, Shanghai Skin Disease Hospital, School of Medicine, Tongji University, Shanghai, and 2Department of Biochemistry, School of Basic Medical Science, Fudan University, Shanghai, China
#These authors contributed equally and should be considered as first authors.
This study examined the relationship between type 2 diabetes and late syphilis. A retrospective analysis was conducted, including 96 syphilis patients with type 2 diabetes and 122 matched non-diabetic syphilis controls. The development of late-stage syphilis and responses to initial treatment were monitored over a 2-year period. Stratified logistic regression was used to assess whether diabetes increased the risk of late syphilis. Differences in initial treatment responses between the 2 groups were evaluated using χ2 tests and Kaplan–Meier curves. The cohort study confirmed that the serological cure rate within 12 months was significantly lower in diabetic syphilis patients. Type 2 diabetes significantly impacts the efficacy of syphilis treatment and is a risk factor for late syphilis.
SIGNIFICANCE
Type 2 diabetes is strongly associated with late syphilis.
Type 2 diabetes patients are more likely to experience treatment failure.
Type 2 diabetes patients with poor short-term blood glucose control are more likely to develop late syphilis.
Key words: diabetes; syphilis; cohort study; risk.
Citation: Acta Derm Venereol 2025; 105: adv42210. DOI: https://doi.org/10.2340/actadv.v105.42210.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Oct 10, 2024. Accepted after revision: Mar 13, 2025. Published: Apr 8, 2025.
Corr: Qingqiong Luo, Department of Clinical Laboratory Medicine, Shanghai Skin Disease Hospital, School of Medicine, Tongji University, Shanghai, China. E-mail: luoqingqiong2007@126.com
Competing interests and funding: The authors have no conflicts of interes to declare.
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
INTRODUCTION
Syphilis is caused by Treponema pallidum (T.p.) infection, which is the most common sexually transmitted disease (STD) worldwide. The World Health Organization (WHO) estimates that 8 million adults between 15 and 49 years old acquired syphilis in 2022 (https://www.who.int/news-room/fact-sheets/detail/syphilis). The long incubation period, diverse symptoms, and immune evasion characteristics of syphilis are responsible for its epidemic status, especially in low- and middle-income populations and men who have sex with men (MSM). The natural history of syphilis can be divided into 2 broad stages, including early syphilis (primary, secondary, and early latent syphilis of no more than 2 years’ duration), and late syphilis (late latent syphilis and symptomatic late syphilis) (2). Early syphilis is characterized by syphilitic manifestations such as primary chancre at the site of inoculation and secondary mucocutaneous lesions affecting the skin, mucous membranes, and lymph nodes. Without appropriate treatment, the disease progresses to a late latent stage, which can persist for years (3). Notably, about 35% individuals with late latent syphilis will develop severe manifestations of tertiary syphilis (4), including irreversible damage of the cardiovascular and central nervous systems, leading to severe morbidity or even death.
The diagnosis and assessment of syphilis treatment response rely on serological tests. Currently, nontreponemal tests that detect antibodies to a nonspecific antigen are the most widely used methods, such as the Venereal Disease Research Laboratory (VDRL) test and Tolulized Red Unheated Serum Test (TRUST) (5). A 4-fold decline in nontreponemal antibody titre is required to indicate effective treatment. Serological cure usually occurs within 1 year after treatment in most early syphilis cases (5). However, persistently positive nontreponemal antibody titres despite an appropriate decline (“serofast”) may happen in 15–41% patients. Moreover, about 10% patients may experience a less than fourfold decrease in titre or may have recurrence after treatment, which indicates treatment failure (6). It is currently believed that treatment failure mainly occurs in immunocompromised people, such as the HIV-infected population (7). However, there are still some non-HIV patients whose disease is not effectively controlled even if they receive early treatment. Risk factors for syphilis treatment failure and late syphilis still deserve further study.
Diabetes mellitus is a metabolic disease characterized by high blood glucose levels. There are two types of diabetes. Type 1 diabetes (T1D) primarily results from insufficient insulin secretion, whereas type 2 diabetes (T2D) is mainly caused by insulin resistance. According to the WHO, 14% of adults aged 18 years and older were living with diabetes, with more than 95% of diabetic people having T2D in 2022 (https://www.who.int/news-room/fact-sheets/detail/diabetes). At present, multiple studies have shown that poorly controlled diabetes increases the risk and severity of a wide range of infections, leading to high rates of hospitalization and death (8, 9). However, the relationship between T2D and syphilis is still unclear. Although a series of retrospective cohort analyses suggested that neurosyphilis may induce the occurrence of T2D (10), whether diabetes would aggravate syphilis development or mitigate the therapeutic effect of syphilis remained unknown.
In this study, we explored the relationship between T2D and syphilis by retrospectively reviewing the outcomes of 218 patients with early syphilis after treatment for over 2 years. We found that T2D was highly associated with late syphilis and can cause treatment failure. This study emphasizes personalized treatment options for syphilis patients with diabetes, thereby improving their treatment outcomes and providing a basis for further research on the association between diabetes and syphilis development.
Materials and methods
Statement of ethics
This research was conducted in accordance with the ethics requirements of the World Medical Association Declaration of Helsinki and was approved by the Institutional Review Board of Shanghai Skin Disease Hospital (Approval No: 2024-15).
Syphilis patient recruitment and diagnostic criteria
This study screened patients who visited Shanghai Skin Disease Hospital between 2018 and 2024. Patients aged ≥ 18 diagnosed with early syphilis at their first visit were screened. The diagnosis of early syphilis followed the guidelines (11), requiring: (i) positive serum TPPA and (ii) corresponding characteristics of early syphilis, such as chancre, macules, papules, scaly skin lesions, follicular rash, and pustular rash.
Exposure measurement
Patients were divided into an exposure group and a control group based on the presence of diabetes. The T2D patients met at least one of the following conditions according to the American Diabetes Association (ADA) guideline for T2D, 2024 (12): (i) symptoms of diabetes and random blood sugar ≥ 11.0 mmol/L, (ii) glycated haemoglobin (HbA1c) ≥ 6.5%, (iii) fasting blood glucose ≥ 7.0 mmol/L. The diagnosis of diabetes as already mentioned should occur at or before the first treatment of the patient. Moreover, as a secondary exposure of interest, a pooled T2D cohort was utilized for a sub-analysis to assess the risk of late syphilis among patients with diabetes under varying glycaemic control conditions. Poor long-term glycaemic control was defined as HbA1c ≥ 7.0%, and poor short-term glycaemic control was defined as fructosamine (FMN) ≥ 268 mol/L (https://www.hopkinsguides.com/hopkins/view/Johns_Hopkins_Diabetes_Guide/547055/all/).
Syphilis treatment
Treatment of syphilis patients follows the Syphilis Diagnosis and Treatment Guidelines (2020) (13). The recommended regimen for early syphilis is benzathine penicillin 2.4 million U, intramuscular injection on both sides of the hip, once a week, a total of 1~2 times; or procaine penicillin 800,000 U/day intramuscular injection for 15 consecutive days. An alternative regimen is ceftriaxone 0.5~1 g intramuscular injection or intravenous injection once a day for 10 days. Patients allergic to penicillin should take doxycycline 100 mg twice a day for 15 days.
Evaluation of the efficacy of the first treatment
The included patients were retrospectively collected for TRUST titres and clinical diagnostic information. TRUST titres at 3–6 months, 6–9 months, and 9–12 months were used to evaluate treatment effectiveness. The primary criteria for treatment response include the resolution of symptoms and a decrease in serological titres. The evaluation of treatment efficacy was stratified into 3 groups based on the initial titre levels:
- Low initial titre group (< 1:4): Even if the titre of this type of patient has not completely dropped to negative (maintained between 1:2–1:4), as long as the symptoms are completely relieved and no new symptoms appear during follow-up, the treatment can still be considered effective.
- Titre 1:4–1:64 group: Most patients with early syphilis belong to this titre range. We strictly follow the efficacy evaluation guidelines. The TRUST titre needs to drop 4-fold and there should be no persistent symptoms before the treatment is considered successful.
- High initial titre (≥ 1:64) group: For the high initial titre group (≥ 1:64), a reduction to the typical low-titre level (below 1:8) and the control or disappearance of clinical symptoms are considered indicators of treatment response.
It should be noted that serological fixation is also considered a valid indicator of treatment efficacy. In the case of multiple records within the same time period, the last recorded value was retained. Patients with early symptomatic neurosyphilis at the first visit and those with HIV infection were excluded from this study.
Evaluation of late syphilis
The diagnosis of late syphilis met the following conditions: (i) the course of disease was more than 2 years, (ii) the serum TRUST titre did not reach a 4-fold decrease or remained at ≥ 1:16, (iii) with or without symptoms. Patients with reinfection were excluded, depending on whether there was a possible history of re-exposure or clinical evidence of new infection. In cases with multiple records existed within the same time period, the last record was retained. Patients with early symptomatic neurosyphilis at the first visit and those with HIV infection were excluded from this study.
Statistical analysis
Propensity score matching. For the primary analysis, propensity score matching (PSM) was used to match the control group based on age, gender, and initial TRUST titre in a 1:1 ratio using R version 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria). We first excluded patients without age, gender, blood pressure glucose or lipid information, as well as patients already diagnosed as late syphilis at the first visit. Patients were eligible for inclusion if they had follow-up records within a period of ≥ 2 years after their first visit to this hospital, and were excluded if they were lost to follow-up > 2 times within the specified follow-up time points. Patients with symptoms of reinfection (e.g., recurrent genital ulcers or rashes) or those at risk of reinfection (e.g., history of prostitution or contact with syphilis patients) during follow-up were excluded. A caliper width of 0.01 standard deviations of the logit of the propensity score was used for matching. The standardized mean difference (SMD) < 0.1 was used to identify well-balanced covariates before and after PSM.
Missing data. Missing data for serum TRUST titres were imputed using multiple imputation, which was performed using predictive mean matching (PMM) method implemented within the multiple imputation by chained equations (MICE) algorithm, adjusting for factors associated with missingness including age, sex, initial titre, HbA1c, FMN, hypertension (HTN), and dyslipidaemia (DLP). Five imputed datasets were generated. The maximum number of iterations was set at 5 to ensure convergence. A random seed of 500 was applied to ensure reproducibility. Sensitivity analyses assessed the robustness and consistency of different imputation methods by comparing the observations carried backward (LOCFB) method with the MICE results.
Regression and survival analysis. Subgroup analysis was used to evaluate the association between diabetes and late syphilis; subgroup analyses according to age, sex, and serum TRUST were performed using univariate and multivariable logistic regression, and p < 0.05 was considered statistically significant. For treatment effectiveness comparison, the χ2 test and Kaplan–Meier analysis were utilized to assess the proportion of patients responding to treatment within one year.
Results
Cohort enrolment
A total of 59,919 syphilis patients who visited Shanghai Skin Disease Hospital from January 2018 to January 2024 were screened, with 749 of them being diagnosed with early syphilis at their first attendance. Of these 749 patients, 96 patients had been diagnosed with T2D before or at the time of first visit, while 653 patients were confirmed to be non-diabetics (NOD). Basic information on these patients is summarized in Table SI. Finally, 218 patients including 122 NOD and 96 T2D patients were enrolled after PSM based on age, gender, initial serum TRUST (Table I, Fig 1A). The demographic and clinical characteristics of the two groups were generally well balanced at baseline. SMDs for all covariates after PSM were < 0.10 (age = 0.073, gender < 0.001, initial serum TRUST = 0.088).
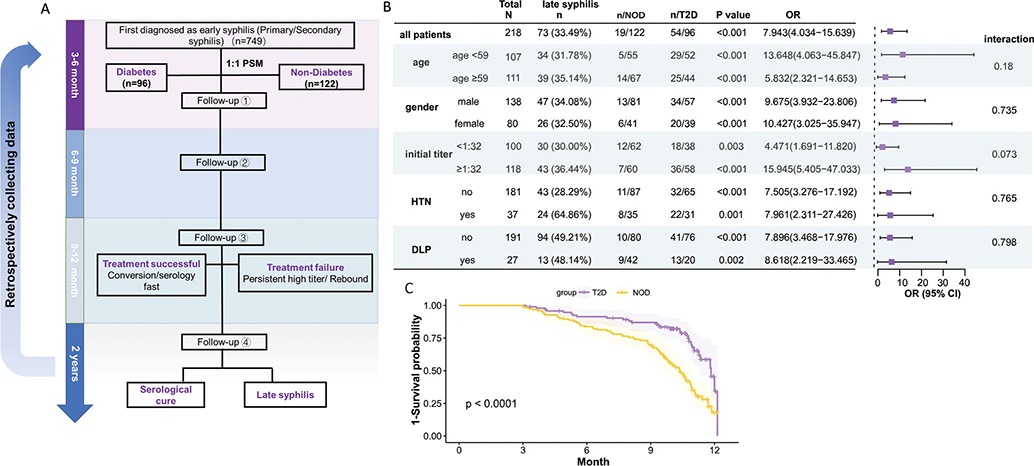
Fig. 1. Cohort analysis for association between T2D and syphilis. (A) Flowchart of patient enrolment and data collection; (B) subgroup analysis of diabetes affecting late syphilis performed using multivariable logistic regression; (C) Kaplan–Meier curve evaluating the response rate of T2D and NOD patients after MICE.
T2D was a risk factor of late syphilis
Among the 218 participants, 73 cases were finally diagnosed with late syphilis, with a significantly higher prevalence observed in the T2D group (54 cases, 73.9%) compared with the NOD group (19 cases, 26.1%) (χ² = 40.559, p < 0.0001). Multivariable logistic regression analysis showed that T2D obviously increased the risk of late syphilis, even after adjusting for age, gender, initial TRUST titre, hypertension, dyslipidaemia, and initial treatment plan (crude OR = 6.970, 95% CI = 3.700–13.14; adjusted OR = 7.943, 95% CI = 4.034–15.639, p < 0.0001). Subgroup analyses demonstrated consistent associations between diabetes and late syphilis across various patient characteristics, with a more pronounced effect observed in patients under the age of 59 and those with higher initial titres (Fig. 1B). These findings were consistent with the results from univariable logistic regression (Fig S1A).
Diabetes was correlated with syphilis treatment failure
Due to the strong association between T2D and late syphilis, we further investigated whether diabetes affected the effectiveness of the first treatment. Serum TRUST titres for all enrolled patients were retrospectively collected at each time point described in Fig 1A. Patients were classified as treatment responders and non-responders, with non-responders subdivided into those with persistently high titres and those with rebound titres (Table II). There were no significant differences in baseline characteristics between diabetic and non-diabetic patients who were lost to follow-up (Table SII). More NOD patients responded within 3–6 months after initial treatment (χ² = 4.755, p = 0.029). At the 6–9 months interval, no significant difference was found between the 2 groups. However, at the 9–12 months interval, a significantly higher portion of T2D patients exhibited persistently high titres (n = 45, χ² = 5.317, p = 0.02) and rebound titres (n = 10, χ² = 9.716, p = 0.001). The cumulative probability of effective treatment within 12 months was then estimated by Kaplan–Meier survival analysis. After MICE, NOD showed a significant higher possibility of serological recovery one year after treatment (p < 0.0001) (Fig 1C). These results were confirmed with data analysed without MICE and using LOCB methods (Fig S1B, C).
Poor short-term glycaemic control led to higher risk of late syphilis
A subset analysis of pooled T2D patients (n = 96) with different baseline glycaemic control status was also performed (Table III). Among patients with poor long-term glycaemic control, 62.26% were found to have late syphilis, compared with 41.81% in the better long-term glycaemic control group. However, this difference was not statistically significant (χ² = 0.038, p = 0.844). In patients with poor short-term control, 66.67% progressed into late syphilis, compared with 42.85% in the better short-term control group (χ² = 5.385, p = 0.02). Multivariable logistic regression showed that T2D patients with poor short-term glycaemic control had a significantly increased risk of late syphilis (adjusted OR = 2.61, 95% CI = 1.019-6.724, p = 0.004, Table III).
DISCUSSION
Diabetes, a prevalent chronic metabolic disorder globally, is strongly associated with increased susceptibility to infectious diseases. However, the interplay between diabetes and syphilis remains underexplored. In this study, we retrospectively compared the progression of syphilis between T2D patients and age-, sex-, and condition-matched NOD controls. Our findings reveal that T2D significantly correlates with treatment failure and prolonged disease duration in syphilis.
The influence of diabetes on infections has been extensively documented in a series of studies. Carey et al. demonstrated in a large primary care cohort study in the UK that diabetes increased the long-term infection risk and hospitalization ratio (14), a finding also corroborated by Mor et al. in Denmark (15). Specifically, diabetes is known to significantly increase susceptibility to diverse cutaneous complications such as foot infections, gangrene, skin ulcers, and poor wound healing (16). The association between syphilis and diabetes has been noted since the 19th century (17). More recently, Yang et al. identified a higher prevalence of diabetes among neurosyphilis patients (10). Wang et al. highlighted the severity of blood–brain barrier disruption in syphilis patients with high HbAc1 levels (18). Additionally, Li et al. explored dysregulated gene expression patterns in syphilis combined with diabetes (19). However, these studies predominantly focused on the nerve damage caused by syphilis, treating diabetes as a secondary metabolic disorder. The impact of diabetes on the progression of syphilis has thus far received limited attention.
In our study, we specifically investigated how diabetes contributed to treatment failure and prolonged disease progression in syphilis. Cohort analysis showed that T2D patients had a significantly higher likelihood of progressing to the late stage of syphilis. Subgroup analysis further underscored that diabetes exerted a pronounced influence in patients with higher initial serum TRUST titres, consistent with previous findings indicating high initial TRUST titres as a strong risk factor for severe syphilis (20). Moreover, we observed that T2D patients were more likely to experience persistently high serum TRUST titre and titre rebound after initial treatment, a pattern reminiscent of treatment outcomes observed in diabetic patients with Mycobacterium tuberculosis infection (21). These findings carry significant implications for patient-centred care decisions for individuals with both diabetes and syphilis.
Our study also uncovered several additional significant findings. Firstly, we observed that short-term glycaemic control, as indicated by FMN, was more strongly associated with late syphilis compared with HbA1c levels. This suggested that transient hyperglycaemia may play a more critical role in exacerbating disease severity. Secondly, we found a substantial association between diabetes and neurosyphilis among patients, aligning with findings from the research by Xiao et al. in Xiamen (22). Specifically, of the 24 T2D patients with late syphilis who received CSF testing in our study, 22 were diagnosed with neurosyphilis, compared with 13 out of 21 NOD patients (p = 0.01). However, due to the limited number of patients who underwent cerebrospinal fluid (CSF) testing in our cohort (only 45 patients), and the fact that some patients had CSF testing more than two years after diagnosis, further research was needed to thoroughly investigate the association between diabetes and early neurosyphilis.
The mechanism through which diabetes impacts infectious diseases primarily centres on immune deficiency, characterized by significant impairments in key immune functions. For instance, diabetes is associated with reduced chemotactic and phagocytic abilities of neutrophils (23), decreased activity of natural killer (NK) cells (24), and abnormal function of CD4+ T cells and cytokines, which can lead to chronicity of infections (25). In the context of syphilis progression, the interplay involves the accumulation of macrophages, activation of CD4+ T cells and the intricate Th1 cell–cytokine–macrophage interaction, which is crucial for clearing Treponema pallidum (26). Consequently, impaired immune responses in diabetic patients may result in persistent infection and a diminished response to treatment.
The necessity of glycaemic control and diabetes management has been well recognized in the management of various infectious disease. For example, hyperglycaemia-induced antibiotic resistance in Staphylococcus aureus has recently been proved to be mitigated by insulin therapy (27). Reduction in blood glucose to within a normal range was found to be associated with increased serum neutralizing antibody concentrations and can improve therapeutic outcomes in COVID-19 (28). Moreover, long-term glycaemic control has also been shown to reduce the incidence of surgical and trauma infections associated with hyperglycaemia (≥ 200 mg/dL) (29, 30). However, glycaemic control strategies specifically for syphilis patients have not yet been well studied. In this study, although we found a significant correlation of T2D with the development of late syphilis, the impact of glycaemic control on the clinical outcomes of syphilis patients needs further investigation. Careful consideration of factors such as the patient’s immune status and potential drug interactions is essential when developing glycaemic management plans for syphilis patients with diabetes to optimize therapeutic outcomes.
Of note is that there are also several limitations in this study. Firstly, in process of patient recruitment and analysis, the study was conducted in a hospital specializing in sexually transmitted diseases (STDs), thus the higher proportion of complex cases in specialized hospitals may affect the generalizability of the findings. Besides, although PSM was used to match diabetic and non-diabetic patients to ensure equality between the two groups, the number of young syphilis patients with T2D was small, resulting in a relatively high overall age of the cohort after matching. Although a subgroup analysis was performed based on a median age of 59, the results in the younger population with syphilis infection need further exploration. For missing follow-up data, although MICE is a widely accepted method that effectively reduces bias introduced by missing data, this method is based on the assumption that data are missing completely at random (MCAR). We cannot completely rule out the possibility of loss to unobserved factors, which may introduce inaccuracy in the imputed values. Secondly, due to the limited number of T1D patients, we did not investigate the relationship between T1D and syphilis in the cohort study. However, we performed a Mendelian randomization (MR) analysis on T1D and syphilis. Similar to T2D, it increased the risk of late syphilis (Fig. S2). Thirdly, this study employed the Kaplan–Meier (K–M) curve to assess the treatment outcomes in diabetic and non-diabetic syphilis patients. However, in practice, the risk of treatment failure in diabetic patients may fluctuate over time due to various factors, which cannot be reflected by K–M curve. Although glucose control was assessed by HbA1c and FMN in this study, these indicators did not directly describe the glucose fluctuations, so future studies should incorporate continuous glucose monitoring (CGM) or flash glucose monitoring (FGM) to obtain more accurate data on glycaemic control. Time-series analysis may be employed to explore the relationship between blood glucose changes and syphilis. Additionally, the impact of diabetes-induced immune dysfunction on the immune system is another important research direction. Finally, unobserved confounding factors may still affect the results, such as the patient’s occupation, place of residence, and income etc.
In conclusion, the study demonstrated a significantly elevated risk of treatment failure and disease progression to late syphilis among T2D patients compared with the general population, especially in those with poor short-term glycaemic control. These results highlight the need for tailored treatment strategies for syphilis patients with diabetes, including more frequent follow-ups and personalized treatment plans. Future research should involve large-scale, longitudinal clinical cohort studies to investigate the relationship between diabetes, glycaemic control, and syphilis progression. Emphasis should be placed on key factors such as glucose fluctuations and immune status etc. to better inform the development of personalized treatment strategies.
ACKNOWLEDGEMENTS
IRB approval status: This research was conducted in accordance with the ethics requirements of the World Medical Association Declaration of Helsinki and was approved by the Institutional Review Board of Shanghai Skin Disease Hospital (Approval No: 2024-15).
REFERENCES
- Elendu C, Amaechi DC, Elendu ID, Elendu TC, Amaechi EC, Usoro EU, et al. Global perspectives on the burden of sexually transmitted diseases: a narrative review. Medicine 2024; 103: e38199. https://doi.org/10.1097/MD.0000000000038199
- Plagens-Rotman K, Jarząbek-Bielecka G, Merks P, Kędzia W, Czarnecka-Operacz M. Syphilis: then and now. Postepy Dermatol Alergol 2021; 38: 550–554. http://doi.org/10.5114/ada.2021.108930
- Whiting C, Schwartzman G, Khachemoune A. Syphilis in dermatology: recognition and management. Am J Clin Dermatol 2023; 24: 287–297. http://doi.org/10.1007/s40257-022-00755-3
- O’Byrne P, MacPherson P. Clinical updates syphilis. London: BMJ Publishing Group; 2019. http://doi.org/10.1136/bmj.l4159
- Clement ME, Okeke NL, Hicks CB Treatment of syphilis: a systematic review. JAMA 2014; 312: 1905–1917. http://doi.org/10.1001/jama.2014.13259
- Workowski KA, Berman SM. Centers for Disease Control and Prevention sexually transmitted disease treatment guidelines. Clin Infect Dis 2011; 53: S59–S63. http://doi.org/10.1093/cid/cir694
- Seña AC, Zhang X-H, Li T, Zheng H-P, Yang B, Yang L-G, et al. A systematic review of syphilis serological treatment outcomes in HIV-infected and HIV-uninfected persons: rethinking the significance of serological non-responsiveness and the serofast state after therapy. BMC Infect Dis 2015; 15: 1–15. http://doi.org/10.1186/s12879-015-1209-0
- Shah BR, Hux JE Quantifying the risk of infectious diseases for people with diabetes. Diabetes Care 2003; 26: 510–513. http://doi.org/10.2337/diacare.26.2.510
- Zoppini G, Fedeli U, Schievano E, Dauriz M, Targher G, Bonora E, et al. Mortality from infectious diseases in diabetes. Nutr Metab Cardiovasc Dis 2018; 28: 444–450. http://doi.org/10.1016/j.numecd.2017.12.007
- Yang T, Tong M, Xi Y, Guo X, Chen Y, Zhang Y, et al. Association between neurosyphilis and diabetes mellitus: resurgence of an old problem. J Diabetes 2014; 6: 403–408. http://doi.org/10.1111/1753-0407.12119
- Tuddenham S, Hamill MM, Ghanem KG. Diagnosis and treatment of sexually transmitted infections: a review. JAMA 2022; 327: 161–172. http://doi.org/10.1001/jama.2021.23487
- American Diabetes Association Professional Practice Committee. Diagnosis and classification of diabetes: standards of care in diabetes – 2024. Diabetes Care 2024; 47: S20–S42. http://doi.org/10.2337/dc24-S002
- Wang Q. Guidelines for diagnosis and treatment of syphilis, gonorrhea and genital chlamydia trachomatis infection (2020). Chin J Dermatol 2020; 53: 168–179. http://doi.org/10.35541/cjd.20190808
- Carey IM, Critchley JA, Chaudhry UA, DeWilde S, Limb ES, Bowen L, et al. Contribution of infection to mortality in people with type 2 diabetes: a population-based cohort study using electronic records. Lancet Reg Health Eur 2025; 48: 101147. http://doi.org/10.1016/j.lanepe.2024.101147
- Mor A, Dekkers OM, Nielsen JS, Beck-Nielsen H, Sørensen HT, Thomsen RW. Impact of glycemic control on risk of infections in patients with type 2 diabetes: a population-based cohort study. Am J Epidemiol 2017; 186: 227–236. http://doi.org/10.1093/aje/kwx049
- Hines A, Alavi A, Davis MD. Cutaneous manifestations of diabetes. Med Clin 2021; 105: 681–697. http://doi.org/10.1016/j.mcna.2021.04.008
- Rosenbloom J. The relation between diabetes mellitus and clinical syphilis. J Am Med Assoc 1917; 68: 1232–1234. https://jamanetwork.com/journals/jama/article-abstract/442004
- Wang F, Ge H, Su X, Wang R, Zeng J, Miao J. High HbA 1c level is correlated with blood–brain barrier disruption in syphilis patients. Neurol Sci 2020; 41: 83–90. https://doi.org/10.1007/s10072-019-04031-x
- Li W, Luo C, Xie X, Xiao Y, Zhao F, Cai J, et al. Identification of key genes and pathways in syphilis combined with diabetes: a bioinformatics study. AMB Express 2020; 10: 1–10. https://doi.org/10.1186/s13568-020-01009-3
- Luo Z, Zhu L, Ding Y, Yuan J, Li W, Wu Q, et al. Factors associated with syphilis treatment failure and reinfection: a longitudinal cohort study in Shenzhen, China. BMC Infect Dis 2017; 17: 1–5. https://doi.org/10.1186/s12879-017-2715-z
- Baker MA, Harries AD, Jeon CY, Hart JE, Kapur A, Lönnroth K, et al. The impact of diabetes on tuberculosis treatment outcomes: a systematic review. BMC Med 2011; 9: 1–15. https://doi.org/10.1186/1741-7015-9-81
- Xiao Y, Chen M-J, Shen X, Lin L-R, Liu L-L, Yang T-C, et al. Metabolic disorders in patients with central nervous system infections: associations with neurosyphilis. Eur Neurol 2019; 81: 270–277. http://doi.org/10.1159/000503626
- Spiller F, Carlos D, Souto FO, De Freitas A, Soares FS, Vieira SM, et al. α1-Acid glycoprotein decreases neutrophil migration and increases susceptibility to sepsis in diabetic mice. Diabetes 2012; 61: 1584–1591. https://doi.org/10.2337/db11-1613.
- Kim JH, Park K, Lee SB, Kang S, Park JS, Ahn CW, et al. Relationship between natural killer cell activity and glucose control in patients with type 2 diabetes and prediabetes. J Diabetes Investig 2019; 10: 1223–1228. https://doi.org/10.1111/jdi.13002
- Jagannathan-Bogdan M, McDonnell ME, Shin H, Rehman Q, Hasturk H, Apovian CM, et al. Elevated proinflammatory cytokine production by a skewed T cell compartment requires monocytes and promotes inflammation in type 2 diabetes. J Immunol 2011; 186: 1162–1172. https://doi.org/10.4049/jimmunol.1002615
- Carlson JA, Dabiri G, Cribier B, Sell S. The immunopathobiology of syphilis: the manifestations and course of syphilis are determined by the level of delayed-type hypersensitivity. Am J Dermatopathol 2011; 33: 433–460. https://doi.org/10.1097/DAD.0b013e3181e8b587
- Shook JC, Genito CJ, Darwitz BP, Tyson KJ, Velez AZ, Bridwell SK, et al. Diabetes potentiates the emergence and expansion of antibiotic resistance. Sci Adv 2025; 11: eads1591. https://doi.org/10.1126/sciadv.ads1591
- Watanabe M, Balena A, Masi D, Tozzi R, Risi R, Caputi A, et al. Rapid weight loss, central obesity improvement and blood glucose reduction are associated with a stronger adaptive immune response following COVID-19 mRNA vaccine. Vaccines 2022; 10: 79. https://doi.org/10.3390/vaccines10010079
- Seidelman JL, Mantyh CR, Anderson DJ. Surgical site infection prevention: a review. JAMA 2023; 329: 244–52. https://doi.org/10.1001/jama.2022.24075
- Ma J, Zhao X, Su Q, Dang W, Zhang X, Yuan X, et al. Effect of early intensive insulin therapy on immune function of aged patients with severe trauma. J Huazhong Univ Sci Technolog Med Sci 2012; 32: 400–404. https://doi.org/10.1007/s11596-012-0069-8