QUIZ SECTION
Erythematous Papules with Central Hyperkeratosis in Two Young Women: A Quiz
Nadine WIEDENMAYER*, Deniz GOECEBE, Ines BERTLICH and Ferdinand TOBERER
Department of Dermatology, Venerology, and Allergology, University Medical Center, Ruprecht-Karls-University Heidelberg, Im Neuenheimer Feld 440, DE-69120 Heidelberg, Germany. *E-mail: Nadine.wiedenmayer@med.uni-heidelberg.de
Citation: Acta Derm Venereol 2024; 104: adv42217. DOI: https://doi.org/10.2340/actadv.v104.42217.
Copyright: © 2024 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Published: Nov 19, 2024
In this quiz we present 2 cases of young women with skin lesions in form of erythematous papules with central hyperkeratosis.
Case 1: A 24-year-old female patient presented with new bilateral skin lesions on her arms, particularly on the elbows and on her thighs. Additionally, she reported a history of adrenogenital syndrome of the classic type. Dermatological examination revealed small, partly isolated, partly grouped papules with central hyperkeratosis (Fig. 1A, B). Histology revealed an epidermis with irregular acanthosis with a transepidermal canal filled with keratinous masses and neutrophilic granulocytes. In the corium, a mixed infiltrate of lymphocytes, histiocytes and small granulomas was present (Fig. 2A, B). Elastica staining showed preserved elastic fibres.
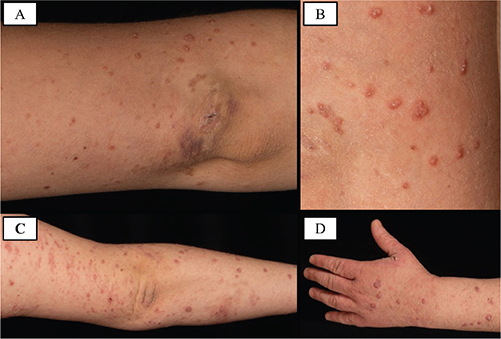
Fig. 1. Skin features of the patients. Multiple erythematous papules with central hyperkeratosis. (A) Overview patient 1. (B) Close-up patient 1. (C) Overview patient 2. (D) Close-up patient 2.
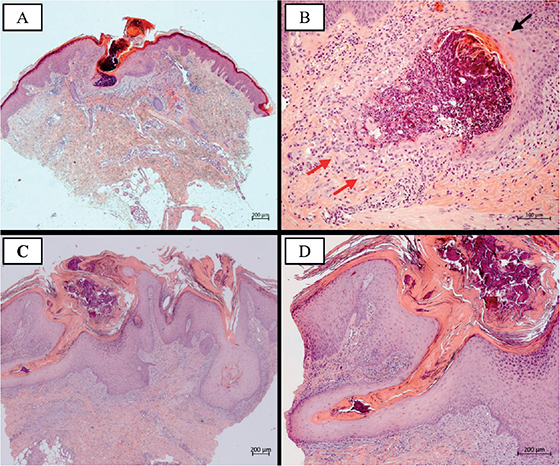
Fig. 2. Histologic findings – haematoxylin eosin staining (HE). (A) Patient 1, HE original magnification × 25: acanthotic epidermis with orthohyperkeratosis. Transepidermal canal filled with keratinous masses and neutrophilic granulocytes. Dermal mixed inflammatory infiltrate, partly lymphocytic, histiocytic, and granulomatous. (B) Patient 1, HE original magnification × 100: cell detritus and neutrophilic granulocytes. Dyskeratosis (black arrow) and multinucleated giant cells (red arrows). (C) Patient 2, HE original magnification × 25: epidermal invagination into the dermis, compact hyperkeratosis of the epidermis, parakeratosis and plug formation. Subepidermal inflammatory infiltrate of lymphocytes and eosinophilic granulocytes. (D) Patient 2, HE original magnification × 50: dilated hair follicle with keratinous masses.
Case 2: Another 24-year-old female patient presented with a 6-year history of skin lesions that initially appeared on the upper arms and subsequently spread to the forearms. In the past 2 months, the lesions had spread rapidly across the entire body, accompanied by severe itching. Clinical examination showed disseminated erythematous, mostly follicularly bound papules with central hyperkeratosis on the trunk and extremities (Fig. 1C, D). Histopathologically, clear invaginations, corresponding to dilated terminal hair follicles, accompanied by hyperparakeratosis, cell detritus, and a neutrophil-rich inflammatory infiltrate were recognizable. No transepidermal discharge of elastic fibres was found (Fig. 2C, D).
What is your diagnosis?
Differential diagnosis 1: Pseudoxanthoma elasticum
Differential diagnosis 2: Perforating reactive collagenosis
Differential diagnosis 3: Hyperkeratosis follicularis et parafollicularis in cutem penetrans
Differential diagnosis 4: Elastosis perforans serpiginosa
See next page for answer.
ANSWERS TO QUIZ
Erythematous Papules with Central Hyperkeratosis in Two Young Women: A Commentary
Diagnosis: Morbus Kyrle (Hyperkeratosis follicularis et parafollicularis in cutem penetrans)
Morbus Kyrle, also known as Kyrle’s disease (KD), is a rare dermatosis belonging to the heterogeneous group of perforating disorders. It was first described as Hyperkeratosis follicularis et parafollicularis in cutem penetrans by the Austrian dermatologist Kyrle in 1916 (1).
KD primarily affects women in a ratio of 6:1 and mostly occurs in adulthood at 30 to 50 years of age (2). The clinical picture is usually dominated by hyperkeratotic parafollicular or follicular papules with an easily detachable cone-shaped epithelial plug localized on the extensor side of the extremities (3).
The aetiology of KD remains unknown. Due to a high incidence of specific systemic disorders, particularly renal failure, diabetes mellitus, haemodialysis, and hepatic failure, many case reports suggest an underlying systemic disorder as aetiology (2, 4). Therefore, thorough examination to rule out the aforementioned diseases is of utmost importance.
Nevertheless, diagnosis based solely on clinical examination remains difficult and is often contingent on histopathological examination. As seen in our patients, histopathology is characterized by invagination of the epidermis filled with keratotic plugs, parakeratosis, basophilic cell debris, and abnormal keratinization (5). Moreover, other acquired perforating dermatoses as most important differential diagnoses can be differentiated by the eliminated material: keratotic material in KD, collagen in perforating reactive collagenosis or perforating folliculitis, and elastic fibres in elastosis perforans serpinginosa. Diseases with secondary perforation such as granuloma anulare, pseudoxanthoma elasticum, and chondrodermatitis nodularis chronica helicis can be considered as further differential diagnoses (6).
Keratolytics containing tretinoin, salicylic acid, or urea are currently regarded as treatment of choice, although the recommendations are based only on reports and small case series. In severe cases acitretin or isotretinoin should be considered. Some authors have reported photo-, cryo-, or laser therapy to be effective in KD. Surgical therapy should only be performed in exceptional cases (2, 4).
In both of our cases, diagnosis of KD was established based on the clinical and histological findings. In contrast to the first case, in which only isolated papules are visible, the second case displays an eczematised picture. To date, no case of KD with concomitant adrenogenital syndrome has been described in the literature. A possible association of these 2 entities remains elusive. Apart from that, we have seen no evidence of concomitant organic diseases in our patients.
In the young woman in the first case, topical treatment with lipophilic tretinoin ointment 0.1% and moisturizing care with urea 10% over a period of 6 weeks resulted in a significant improvement of the skin condition. In the second patient, topical adapalene 1% gel was used on the face, and due to the eczematoid aspect trifarotene 0.005% alternating with betamethasone lotion 0.1% on the body, as well as consistent use of urea-containing emollients. As there was no substantial improvement, additional systemic therapy with isotretinoin 30 mg daily was initiated, with a clear response observed after only 4 weeks of treatment.
These cases are intended to draw attention to Kyrle’s disease, which represents a mostly forgotten entity that should be considered in cases of erythematous papules with central hyperkeratosis. If KD is suspected clinically, the diagnosis should be confirmed by histopathology. Furthermore, it is essential to rule out any internal disease possibly associated with KD.
REFERENCES
- Kyrle J. Über einen ungewöhnlichen Fall von universeller follikulärer und parafollikulärer Hyperkeratose: Hyperkeratosis follicularis et parafollicularis in cutem penetrans. Archiv für Dermatologie und Syphilis 1916; 123: 466–493. https://doi.org/10.1007/BF01826081
- Nair PA, Jivani NB, Diwan NG. Kyrle’s disease in a patient of diabetes mellitus and chronic renal failure on dialysis. J Family Med Prim Care 2015; 4: 284–286. https://doi.org/10.4103/2249-4863.154678
- Shah S, Dave JN, Vora NS, Cardoso B, Goel R. Kyrle’s disease and vitamin D resistant rickets in chronic renal failure (le). Indian J Dermatol Venereol Leprol 1998; 64: 156.
- Rapini RP, Herbert AA, Drucker CR. Acquired perforating dermatosis: evidence for combined transepidermal elimination of both collagen and elastic fibers. Arch Dermatol 1989; 125: 1074–1078. https://doi.org/10.1001/archderm.1989.01670200050007
- Bodman M, Ehredt D Jr, Barker R, Kirkland A, Mude P. Kyrle disease a rare dermatologic condition associated with the diabetic foot. J Am Podiatr Med Assoc 2015; 105: 451–455. https://doi.org/10.7547/14-009
- Ataseven A, Ozturk P, Kucukosmanoglu I, Kurtipek GS. Kyrle’s disease. BMJ Case Rep 2014; 2014. https://doi.org/10.1136/bcr-2013-009905