QUIZ SECTION
Erythematous Plaques on the Dorsum of both Hands and Forearm: A Quiz
Yukiko ISHIZUKA, Takehiro TAKAHASHI* and Yoshihide ASANO
Department of Dermatology, Tohoku University Graduate School of Medicine, 1-1 Seiryo-machi, Aoba-ku, Sendai, 980-8574, Japan. E-mail: takehiro.takahashi@derma.med.tohoku.ac.jp
Citation: Acta Derm Venereol 2024; 104: adv42229. DOI: https://doi.org/10.2340/actadv.v104.42229.
Copyright: © 2024 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Published: Dec 2, 2024
A 70-year-old Japanese woman with a history of diabetes and dyslipidaemia was referred to our clinic for multiple erythematous lesions on her extremities. The lesions on the dorsum of her hands appeared 3 months prior to the initial visit. Additionally, she reported having experienced severe Raynaud’s phenomenon for 5 years. On initial presentation, we observed erythematous plaques with moderate infiltration from the metacarpophalangeal joints to the proximal interphalangeal joints on the dorsum of both hands (Fig. 1A). Similar erythematous plaques were also observed on the left forearm (Fig. 1B). There was no skin sclerosis, and the modified Rodnan total skin thickness score (mRSS) was 0. However, nailfold videocapillaroscopy (NVC) revealed multiple nailfold bleedings and dilated capillaries with abnormal morphologies (Fig. 1C). Blood tests showed an antinuclear antibody titre ≥ 640 (discrete speckled pattern by indirect immunofluorescence) and an elevated serum anti-centromere antibody (ACA) level of 333 U/mL by specific enzyme-linked immunosorbent assay (ELISA) (normal range: 0–10 U/mL). Anti-Sm, anti-topoisomerase I, anti-RNA polymerase III, anti-U1RNP, anti-double-stranded DNA, anti-SS-A/B, and anti-aminoacyl-tRNA synthetase antibodies were all negative. There were no remarkable abnormalities in electrolytes or blood counts.
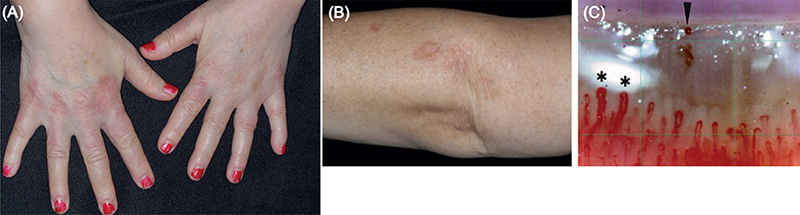
Fig. 1. Clinical presentation of the case. Clinical appearance of erythematous plaques on (A) the dorsum of both hands and (B) the left forearm. Nailfold videocapillaroscopy revealed nailfold bleedings (C: a triangle) and dilated megacapillaries (C: asterisks).
Histopathological findings of her forearm revealed granulomas consisting of epithelioid cells without caseous necrosis in the superficial to mid-dermis (Fig. 2A, B), with multinucleated giant cells also observed in some areas (Fig. 2C).
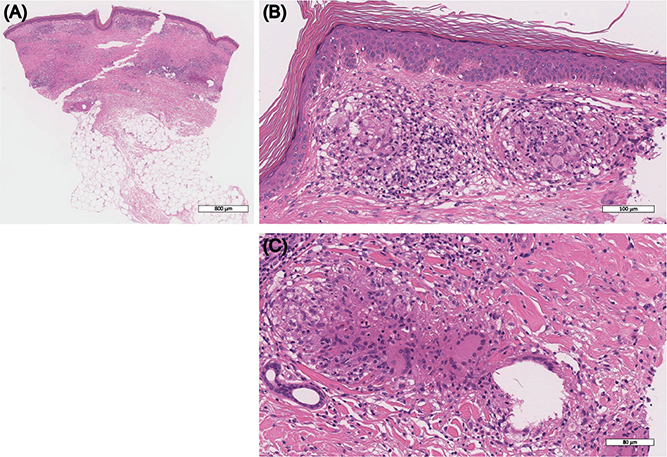
Fig. 2. Histopathological findings of the skin biopsy on the left forearm. (A, B) Epithelioid cell granulomas without caseating necrosis were observed beneath the epidermis. (C) Multinucleated giant cells were present within the granuloma (haematoxylin-eosin [HE] stain).
What is your diagnosis?
Differential diagnosis 1: lupus pernio concomitant with limited systemic sclerosis
Differential diagnosis 2: discoid lupus erythematosus
Differential diagnosis 3: chilblain
Differential diagnosis 4: dermatomyositis
Differential diagnosis 5: Granuloma annulare
See next page for answer.
ANSWERS TO QUIZ
Erythematous Plaques on the Dorsum of both Hands and Forearm: A Commentary
Diagnosis: Lupus pernio concomitant with limited systemic sclerosis
Based on the clinical and pathological findings, we diagnosed sarcoidosis, more specifically lupus pernio (LP), concomitant with ACA-positive systemic sclerosis (SSc) without skin sclerosis (i.e., limited SSc) (1). Chest X-ray revealed bilateral hilar lymphadenopathy, consistent with the diagnosis of sarcoidosis. There were no findings suggestive of sarcoidosis in her eyes or heart, nor were there signs of interstitial lung disease or pulmonary hypertension. A computed tomography scan revealed primary gastric MALT lymphoma, which has been followed up by gastroenterologists without treatment intervention. We initiated treatment for LP with topical steroids, and to date there has been no remarkable progression of either sarcoidosis or SSc.
Sarcoidosis is a granulomatous disorder of unknown cause that affects multiple organs, including the eyes, heart, lungs, and skin. Typically, abundant CD4+ T cells are present in lesional skin, with Th1 immune responses deeply involved in the pathological condition. Additionally, an increase in the number of activated B cells, elevated immunoglobulin levels, and the presence of autoantibodies in humoral immunity have been reported (2). Skin manifestations of sarcoidosis are classified into specific lesions, such as nodules, papules, plaques, and LP, as well as reactive, non-specific lesions like erythema nodosum. LP is relatively rare and often presents on the nose, cheeks, ears, and dorsum of the hands and feet, which are common areas for chilblains (3). Due to their anatomical locations, these lesions are often misdiagnosed as skin symptoms caused by peripheral circulation disorders related to SLE or SSc (4). In our case, there were erythematous plaques on the dorsum of the hand and forearm with clearly defined borders and moderate infiltration. ACA-positive SSc is occasionally accompanied by sarcoidosis and, based on these clinical findings, we suspected LP and performed a skin biopsy, which led to its diagnosis.
SSc is an autoimmune disease characterized by vascular damage and fibrosis of the skin and various internal organs. Th2-polarized immune responses have been shown to be critical during the early and active phases of SSc. In a study analysing longitudinal changes in blood cytokines in diffuse cutaneous SSc (dcSSc) patients, serum levels of Th2 cytokines, such as IL-6, IL-10, and CCL2/MCP-1, were significantly elevated in the early disease phase compared with controls, and these levels generally decreased as skin sclerosis regressed in the later disease phase. Conversely, levels of IL-12, a representative Th1-inducing cytokine, were lower than controls in the early disease phase but increased approximately 15-fold over 6 years, eventually becoming significantly higher than controls. This transition from a Th2- to a Th1-dominant immune environment is thought to be correlated with spontaneous improvement in skin fibrosis in SSc (5).
The overlap of SSc and sarcoidosis is rare, but it has been postulated that Th1/Th2 antagonism is involved in the immune landscape of these overlapping cases (4). Th1 and Th2 cells maintain immune homeostasis by regulating and balancing each other, a concept referred to as the Th1/Th2 paradigm. Th1 cells produce cytokines such as IFN-γ, IL-2, and TNF, promoting cellular immunity and phagocyte-dependent inflammation. A Th1-dominant immune response is implicated in diseases such as rheumatoid arthritis, multiple sclerosis, Crohn’s disease, and sarcoidosis. On the other hand, Th2 cells produce cytokines like IL-4, IL-5, and IL-13, which are related to allergic responses, including IgE production and eosinophil accumulation, as well as in wound healing and fibrotic processes. Th2 immune responses play a central role in conditions such as atopic dermatitis and SSc (5, 6). Importantly, Th1 and Th2 responses are considered mutually antagonistic, offsetting each other when they overlap.
In line with this, for example, sarcoidosis is thought to have a low incidence in atopic dermatitis patients, which is mainly characterized by Th1 and Th2 immune responses, respectively, and Th1/Th2 paradigm is postulated to underpin this phenomenon (6).
In our case, the preceding disease is likely to be SSc, considering the patient’s onset of Raynaud’s phenomenon preceding the erythematous lesions. This was a case of limited SSc, and although there were remarkable capillary abnormalities in the posterior nailfold, skin sclerosis and other organ damage were absent, indicating only mild SSc activity. She had skin lesions on the dorsum of her hands, which are common areas for chilblains. However, her lesions differed from the skin symptoms typically caused by peripheral circulation disorders in SSc. The well-defined erythema and palpable infiltration led us to suspect concomitant LP. It is possible that the presence of sarcoidosis suppressed the activity of SSc, and the balance between the immune responses, based on the Th1/Th2 paradigm, may explain the moderate clinical presentation in this case.
In conclusion, we experienced an overlapping case of LP and limited SSc, with no skin sclerosis but with capillary abnormalities. The clinical picture of our case possibly reflects the Th1/Th2 paradigm, and accumulation of similar rare overlapping cases, along with further investigation into their immune landscape, is warranted.
REFERENCES
- LeRoy EC, Medsger TA, Jr. Criteria for the classification of early systemic sclerosis. J Rheumatol 2001; 28: 1573–1576.
- Damsky W, Wang A, Kim DJ, Young BD, Singh K, Murphy MJ, et al. Inhibition of type 1 immunity with tofacitinib is associated with marked improvement in longstanding sarcoidosis. Nat Commun 2022; 13: 3140. https://doi.org/10.1038/s41467-022-30615-x
- Karadağ AS, Parish LC. Sarcoidosis: a great imitator. Clin Dermatol 2019; 37: 240–254. https://doi.org/10.1016/j.clindermatol.2019.01.005
- Suga H, Asano Y, Tamaki Z, Yamamoto M, Sugaya M, Shimizu J, et al. A case of systemic sclerosis with sarcoidosis. Acta Derm Venereol 2011; 91: 718–720. https://doi.org/10.2340/00015555-1155
- Matsushita T, Hasegawa M, Hamaguchi Y, Takehara K, Sato S. Longitudinal analysis of serum cytokine concentrations in systemic sclerosis: association of interleukin 12 elevation with spontaneous regression of skin sclerosis. J Rheumatol 2006; 33: 275–284.
- Kokturk N, Han ER, Turktas H. Atopic status in patients with sarcoidosis. Allergy Asthma Proc 2005; 26: 121–124.