ORIGINAL REPORT
Impact on Major Life-changing Decisions in Patients with Atopic Dermatitis
Lucía FUENTES-BARRAGÁN1#, Carmen GARCÍA-MORONTA2#, Raquel SANABRIA-DE LA TORRE1,3, Francisco JAVIER LEÓN-PÉREZ2, Alejandro MOLINA-LEYVA2, Salvador ARIAS-SANTIAGO1–3 and Trinidad MONTERO-VÍLCHEZ2,3
1University of Granada, Granada, 2Department of Dermatology, University Hospital Virgen de las Nieves, Granada, and 3Biosanitary Research Institute of Granada, Granada, Spain
#These authors contributed equally to this work and share first authorship.
Atopic dermatitis (AD) is a chronic skin disease that significantly affects patients’ quality of life. While other dermatological conditions like psoriasis are known to impact major life-changing decisions (MLCD), no prior studies have evaluated this in AD. A descriptive cross-sectional study was conducted in patients with AD of at least 6 months’ duration. Sociodemographic and clinical characteristics of the patients, as well as severity from both the physician’s and patient’s point of view, were assessed using different rating scales such as the Eczema Area and Severity Index (EASI). Subsequently, patients were divided according to disease severity into severe AD (EASI ≥ 21) or mild–moderate AD (EASI < 21). Life decisions were evaluated across several areas, including work, education, social life, reproduction, recreation, housing, and lifestyle, using a 4-point Likert scale. A total of 104 patients, with an average disease duration of 20.36 years, were included. The results showed significant MLCD impairment, especially in clothing choices (52.9%), lifestyle (48.1%), and sports activities (41.4%). Severe AD was associated with greater social and emotional challenges, such as difficulties in social interactions (48.6% vs 26.1%) and romantic relationships (48.5% vs 18.8%) compared with mild–moderate AD. These findings highlight the profound impact of AD on daily life, emphasizing the need for comprehensive management strategies that address physical, psychological, and social aspects.
SIGNIFICANCE
Atopic dermatitis is a chronic skin condition that affects many areas of life, beyond just physical symptoms. This study found that atopic dermatitis influences important life decisions, especially in areas like clothing choices, lifestyle, and social activities. Patients with more severe atopic dermatitis experience even greater challenges in these aspects. Understanding how atopic dermatitis impacts daily life can help doctors provide better support and treatment, addressing not just the physical symptoms but also the emotional and social effects. Early and effective care can help reduce the long-term impact of atopic dermatitis on major life choices.
Key words: atopic dermatitis; major life-changing decisions; quality of life.
Citation: Acta Derm Venereol 2025; 105: adv42241. DOI: https://doi.org/10.2340/actadv.v105.42241.
Copyright: © 2025 The Author(s). Published by MJS Publishing, on behalf of the Society for Publication of Acta Dermato-Venereologica. This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/).
Submitted: Oct 16, 2024; Accepted: Mar 3, 2025; Published: Apr 1, 2025
Corr: Dr Salvador Arias Santiago, Department of Dermatology, Hospital Universitario Virgen de las Nieves, Avenida de Madrid, 15, Granada, ES-18012 Spain. E-mail: salvadorarias@ugr.es
Competing interests and funding: The authors have no conflicts of interest to declare.
INTRODUCTION
Atopic dermatitis (AD) is a chronic, inflammatory and recurrent skin disease that occurs in flare-ups. It is characterized by pruritic, erythematous-eczematous lesions, often accompanied by excoriation, lichenification, and nodular formations on xerotic, scaly, and fragile skin. This condition significantly impairs patients’ quality of life, particularly when it involves visible areas such as the antecubital and popliteal fossae, face, and hands, which disrupts daily activities (1). Its aetiopathogenesis is multifactorial, involving genetic components – such as filaggrin gene mutations leading to compromised differentiation and maturation of the stratum corneum, resulting in increased transepidermal water loss – and environmental influences, including sensitization to antigens, microbial exposure, pollution, climate, emotional, and physiological changes. Consequently, epithelial genetic deficiencies, in conjunction with compromised skin barrier function, immune dysregulation, microbial dysbiosis, and stressors can be considered as major contributors to the pathophysiology of AD (1–3).
AD is one of the most common inflammatory diseases, with an increasing prevalence, which is higher in industrialized countries (2, 4, 5). Its symptoms, as well as its treatment requirements, have a multidimensional impact with implications for mental health, productivity, and quality of life. Moreover, it is a disease that accompanies patients at all stages of their life, from childhood and adolescence to adulthood. In the case of adults, about 57% lose at least 1 day of work per year due to the disease, more than 10% develop depressive symptoms, and 88% experience that their ability to handle everyday life is partially compromised (6).
Every day we have to face many decisions that are of no long-term importance, but there are moments in life when we need to make decisions that will mark the direction of one’s life (major life-changing decisions [MLCD]). The diagnosis of a chronic illness has a negative impact on people’s lives physically, psychologically, and socially. Some of these changes involve the alteration of their background, requiring a reconsideration of the sense of their existence, purposes, and priorities. Among these life decisions that an individual must face are professional and educational status, personal relationships, reproductive and sexual desires, housing, leisure and holidays, sport, lifestyle habits, and toxic habits (7, 8). The concept of MLCD, introduced and developed by Bhatti et al., has been foundational in understanding how chronic diseases influence life decisions. Their work led to the creation of the Major Life Changing Decision Profile (MLCDP), a validated tool with 32 questions across 5 domains (education, job/career, family/relationships, social, and physical) (7, 9–11). There are studies that evaluate how chronic diseases, such as cancer, impair patients’ quality of life and play a decisive role in life decisions (7). There are also studies on how these decisions are modified in chronic dermatological conditions like psoriasis (8). However, even though AD is a very prevalent disease, there are no available studies on this topic in AD. Given the high prevalence of AD and its multidimensional impact, understanding its influence on MLCD is crucial for improving patient care and outcomes. This study aims to bridge this knowledge gap by evaluating the effect of AD on MLCD.
MATERIALS AND METHODS
This is a cross-sectional, descriptive study including patients with AD.
Patients seen consecutively at their protocolized review appointment at the Atopic Dermatitis Unit of the Dermatology Department of the Virgen de las Nieves University Hospital were included.
Inclusion criteria:
- Patients with a clinical diagnosis of AD of at least 6 months’ duration.
- Patients aged over 18 years.
- Patients who signed the informed consent or whose consent had been signed by their legal representatives.
Exclusion criteria:
- Patients suffering from other chronic inflammatory skin diseases that could influence MLCD (psoriasis, hidradenitis suppurativa, etc.).
- Patients who have any type of chronic disease that could influence MLCD (inflammatory bowel disease, diabetes mellitus, transplant patients, etc.).
- Patients with cancer or who have suffered from cancer in the last 5 years.
- Patients who refuse to participate in the study.
Variables of interest:
- Sociodemographic, biometric, and clinical variables such as age, sex, profession, educational level, age of disease onset, duration of the disease, number of affected areas, and comorbidities. The data were collected through clinical interview and physical examination.
- Variables related to the impact of AD on MLCD. These were measured by the patient on a 4-point Likert scale ranging from “0: No impact” to “4: Significant impact”. The life decisions considered were those described by Bhatti et al (7):
- Work-related life decisions: career choice, job performance, job promotion opportunities, absence days, salary, decision to take early retirement.
- Education-related life decisions: educational attainment, level of education attained.
- Life decisions related to personal relationships: family relationships, social relationships, choice of partner, sexual impairment.
- Life decisions related to parenthood: decision to have children, number of children.
- Other life decisions: choice of place of residence, choice of house, choice of living abroad, choice of clothes, choice of holiday destination, sport practised, smoking, drug use.
- Variables related to the disease severity:
- Severity of AD assessed by the physician:
- ○ Eczema Area and Severity Index (EASI). This index measures the intensity and extension of AD by assessing 4 signs: erythema, papule or oedema, excoriation, and lichenification, on a scale of 0 to 3. It estimates the average intensity within 4 body regions (head and neck, arms, trunk, and legs), and multiplies it by the body surface area affected, giving a score from 0 to 72 (12). To assess the impact of the severity of AD on MLCD, patients were divided in those with mild-moderate disease (EASI < 21) and those with severe disease (EASI ≥ 21).
- ○ SCORing Atopic Dermatitis (SCORAD). This includes both a clinical assessment and patient-reported symptoms of pruritus and sleep deprivation. Six signs (erythema, oedema, oozing/crusting, excoriations, xerosis, and lichenification) are assessed, with scores from 0 to 3 according to their intensity. The extent of lesions is measured as a percentage of the affected body area (0–100%), while symptoms of pruritus and sleeplessness are assessed on a numerical scale from 0 to 10. The final score ranges from 0 to 103 (12).
- ○ Body Surface Area (BSA). This is based on the dermatologist’s visual assessment of the affected body surface. Considering that the palm of the patient’s hand corresponds to 1% of the body surface, the head and neck 9%, the upper limb 9%, the anterior trunk 18%, posterior 18%, each lower limb 18% and the perineum 19%, the final score ranges from 0–100% (13).
- ○ Investigator Global Assessment (IGA): This is a score that evaluates the patient’s overall AD status. It can be scored from 0 (no inflammatory signs and/or no lesions) to 4 (very severe erythema, papules or infiltration) (3).
- Severity of DA assessed by the patient:
- ○ Patient Oriented Eczema Measure (POEM): Self-assessment of the frequency of symptoms of AD, organized in 7 items, for 1 week. Each section is rated from 0–4 until a total score of 0–28 is obtained. The lower the POEM score, the lower the frequency of AD symptoms (14).
- ○ Atopic Dermatitis Control Tool (ADCT): Self-assessment that consists of 6 questions concerning the state of the disease in the previous 7 days including severity of symptoms, itching, discomfort, impact on sleep, daily activities, and mood and emotions. A score greater than or equal to 7 is considered to indicate poor control (15).
- ○ Well Being Index (WHO-5): This is a questionnaire used to evaluate the subjective psychological well-being of patients in the last 14 days. It contains 5 questions, scored from 5 (all the time) to 0 (none of the time). The final score varies from 0 (no well-being) to 25 (maximum well-being) (16).
- ○ Dermatology Life Quality Index (DLQI): This is a specific tool for evaluating the impact of dermatological diseases on patients’ quality of life. It has 10 sections. Each section is scored from 0–3 to a total score of 0–30. Values of 0–10 indicate no effect on patients’ lives and 11–20 a large effect (6).
- ○ Numerical Rating Scale (NRS) itch and sleep: This is a numerical scale that assesses the severity of itching and lack of sleep, scoring from 0 (no impairment) to 10 (maximum impairment) (12).
Statistical analysis
- Descriptive analysis: Descriptive statistics were used to summarize and present the sample features. Continuous variables were expressed as mean ± standard deviation, while qualitative variables were described by absolute and relative frequency distribution. Likert scale scores are expressed as median and interquartile range.
- Normality testing: A Shapiro–Wilk test for normality was performed for all continuous variables. This helped to determine whether the data followed a normal distribution. In any case where the variables did not follow a normal distribution, appropriate transformations or the use of non-parametric tests were considered.
- Comparison of variables:
- ○ To compare nominal variables, the χ² test or Fisher’s exact test was used as appropriate.
- ○ To compare nominal variables with continuous variables, Student’s t-test for independent samples or Wilcoxon–Mann–Whitney test was used as appropriate.
- Relation between variables and associated factors:
- ○ Pearson’s correlation test was used to evaluate the relation between continuous variables.
- ○ Regression analysis was used to explore associations between variables and their magnitude. Independent variables (severity of illness, gender, age) were defined as predictors in relation to the dependent variable (MLCD).
Statistical significance was defined as a two-tailed p < 0.05. SPSS version 24.0 (IBM Corp, Armonk, NY, USA) was used for statistical analyses.
Ethics
This study was approved by the Research Ethics Committee of the Junta de Andalucía (1422-N-23), in accordance with the Declaration of Helsinki. The nature of the study was explained to all participants, who accepted participation by giving verbal or written consent. All measurement instruments were non-invasive, and the confidentiality of the participants’ data was strictly preserved.
RESULTS
Sociodemographic and clinical characteristics
A total of 104 patients were included in the study. The mean age was 38.65 years (standard deviation [SD] 16.77) and the female: male ratio was 1.26 (29:23). The remaining demographic features are summarized in Table I.
Most patients with AD had an early disease onset with a mean disease duration of 20.36 years (SD 15.18), were active workers (56.7%, 59/104), and had a higher education level (65.4%, 68/104). Half of the patients suffered from rhino-conjunctivitis (51.9%, 54/104), 46.2% (48/104) from asthma, and 19.2% (20/104) from food allergies. The mean number of affected areas was 3.25 (SD 1.55); the most affected areas were the trunk and extremities 85.6% (89/104) and the face 64.4% (67/104).
In terms of disease severity, patients with AD had moderate–severe disease with mean EASI 14.29 (SD 12.14), BSA 23.03 (SD 21.99), and SCORAD 36.98 (SD 20.03). Regarding self-rated severity, mean POEM 14.97 (SD 7.53), DLQI 8.86 (SD 6.93), ADCT 11.63 (SD 6.73), and WHO-5 14.22 (SD 5.76) were found.
Correlation of severity between doctor and patient
The association between the different severity scales, physician- and patient-rated, was studied. A positive association was found between EASI with total SCORAD (r = 0.737), BSA (r = 0.878), NRS itch (r = 0.467), NRS sleep (r = 0.403), total POEM (r = 0.430), total DLQI (r = 0.441) and total ADCT (r = 0.399), with a p-value < 0.001. A correlation was observed between WHO-5 and patient-reported severity (NRS itch, NRS sleep, POEM, DLQI, ADCT). The 5 most significant associations are graphically represented in Fig. 1.

Fig. 1. Bivariate analysis of total Scoring Atopic Dermatitis (SCORAD), Body Surface Area (BSA), Numerical Rating Scale (NRS) itch, total Patient-Oriented Eczema Measure (POEM), and total Dermatology Life Quality Index (DLQI) in relation to Eczema Area and Severity Index (EASI).
Impact of AD on MLCD
AD had a strong impact on MLCD. All data are detailed in Table II. Some 52.9% of patients with AD reported a moderate–severe impact of the disease on their dressing. Lifestyle (48.1%), sport (41.4%), job performance (40.4%), national holidays and leisure (37.5%), social (33.6%) and family relationships (31.8%), sentimental life (28.9%), educational performance (27.9%), holidays and leisure abroad (25.9%), job absenteeism (24%), and consumption of anxiolytics and antidepressants (20.2%) also stood out. These data are represented by a bar diagram in Fig. 2.
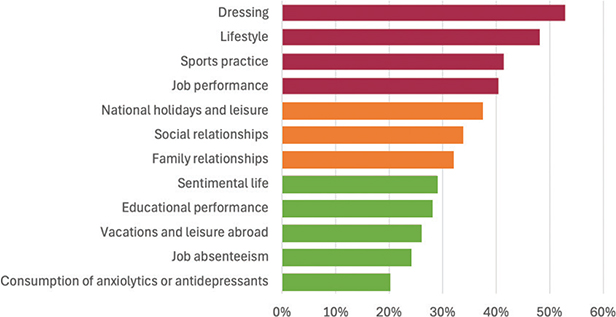
Fig. 2. Percentage of patients with atopic dermatitis showing a moderate-severe impact on most of major life-changing decisions.
Impact of AD severity on MLCD
We decided to compare the impact of AD on patients’ lives according to the severity of the disease. 69 patients had mild–moderate disease (EASI < 21) and 35 severe (EASI ≥ 21).
In relation to the clinical and demographic differences between the 2 groups, it was observed that patients with severe AD developed the disease at an earlier age (12.6 vs 21.74 years, p = 0.044). In addition, severe AD patients had a higher number of affected areas (3.97 vs 2.88, p < 0.001) and the most frequently affected body areas were the buttocks, face, trunk, and extremities. Asthma was also found to be more prevalent in severe AD.
It was also found that vital decisions were affected by the severity of the AD disease. Severe AD patients more frequently reported moderate to severe impairment in socializing with friends (48.6% vs 26.1%, p = 0.002), their love life (48.5% vs 18.8%, p = 0.015), the presence of sexual difficulties (34.2% vs 13%, p = 0.012), the way they dressed (74.3% vs 42%, p = 0.004), and alcohol consumption (36.3% vs 8.7%, p = 0.033). The negative impact of disease symptoms on patients’ lives was also assessed. It was revealed that pain, itching, lack of sleep, physical limitation, embarrassment, lack of confidence, and depression and sadness were more intense in patients with severe AD (Table III).
| Sociodemographic characteristics and MLCD by DA severity | |||
| Mild–moderate DA n = 69 | Severe DA n = 35 | p-value | |
| Sex, % (n) | 0.293 | ||
| Female | 59.4 (41) | 48.6 (17) | |
| Male | 40.6 (28) | 51.4 (18) | |
| Age, mean (SD) | 39.54 (18.34) | 36.91 (13,21) | 0.406 |
| Age of disease onset, mean (SD) | 21.74 (24.72) | 12.6 (19,7) | 0.044* |
| Disease duration, mean (SD) | 18.52 (15.31) | 23.97 (14.44) | 0.079 |
| Employment status, % (n) | 0.507 | ||
| Student | 24.6 (17) | 17.1 (6) | |
| Active | 52.2 (36) | 65.7 (23) | |
| Not active | 7.2 (5) | 8.6 (3) | |
| Retired | 15.9 (11) | 8.6 (3) | |
| Education level, % (n) | 0.96 | ||
| No education | 0 (0) | 0 (0) | |
| Basic education | 34.8 (24) | 34.3 (12) | |
| Higher education | 65.2 (45) | 65.7 (23) | |
| Smoking (yes) % (n) | 24.6 (17) | 31.4 (11) | 0.461 |
| Number of affected areas, mean (SD) | 2.88 (1.65) | 3.97 (1.01) | < 0.001* |
| Most affected area, % (n) | |||
| Hands | 39.1 (27) | 42.9 (15) | 0.714 |
| Genitalia | 21.7 (15) | 28.6 (10) | 0.441 |
| Gluteal region | 26.1 (18) | 45.7 (16) | 0.044* |
| Sub-mammary | 7.2 (5) | 11.4 (4) | 0.473 |
| Face | 55.1 (38) | 82.9 (29) | 0.005* |
| Trunk and limbs | 79.7 (55) | 97.1 (34) | 0.017* |
| Comorbidities, % (n) | |||
| Asthma | 37.7 (26) | 62.9 (22) | 0.015* |
| Food allergies | 20.3 (14) | 20.3 (14) | 0.7 |
| Rhinoconjunctivitis | 53.6 (37) | 48.6 (17) | 0.626 |
| Nasal polyposis | 2.9 (2) | 5.7 (2) | 0.48 |
| Eosinophilic esophagitis | 7.2 (5) | 2.9 (1) | 0.356 |
| Anxiety | 4.3 (3) | 8.6 (3) | 0.383 |
| Depression | 8.7 (6) | 97.1 (34) | 0.261 |
| Cardiovascular disease | 4.3 (3) | 0 (0) | 0.211 |
| Disease severity, mean (SD) | |||
| SCORAD, mean (SD) | 27.99 (16.51) | 54.41 (13,87) | < 0.001* |
| BSA, mean (SD) | 11.89 (11.74) | 46.04 (20,33) | < 0.001* |
| NRS itch, mean (SD) | 5.49 (3.07) | 7.74 (2.92) | < 0.001* |
| NRS sleep, mean (SD) | 3.04 (3.55) | 6.03 (3.63) | < 0.001* |
| POEM, mean (SD) | 13.17 (6.85) | 18.51 (7.65) | < 0.001* |
| DLQI, mean (SD) | 6.96 (5.214) | 12.6 (8.34) | 0.001* |
| ADCT, mean (SD) | 10.14 (6.07) | 14.57 (7.1) | 0.001* |
| WHO, mean (SD) | 14.81 (5.89) | 13.06 (5.37) | 0.143 |
| P-IGA, % (n) | < 0.001* | ||
| No disease | 8.7 (6) | 2.9 (1) | |
| Almost no disease | 44.9 (31) | 8.6 (3) | |
| Mild | 26.1 (18) | 8.6 (3) | |
| Moderate | 15.9 (11) | 57.1 (20) | |
| Severe | 4.3 (3) | 22.9 (8) | |
| Disease intrusiveness, % (n) | 0.001* | ||
| Minimal | 24.6 (17) | 0 (0) | |
| Moderate | 40.6 (28) | 28.6 (10) | |
| High | 24.6 (17) | 40 (14) | |
| Very high | 10.1 (7) | 31.4 (11) | |
| Current severity of AD, % (n) | 0.395 | ||
| Mild | 40.6 (28) | 48.6 (17) | |
| Moderate | 39.1 (27) | 25.7 (9) | |
| Severe | 20.3 (14) | 25.7 (9) | |
| Overall impact of DA, % (n) | 0.001* | ||
| Absent | 0 (0) | 0 (0) | |
| Minimal | 11.6 (8) | 5.7 (2) | |
| Moderate | 23.2 (16) | 34.3 (12) | |
| High | 42 (29) | 60 (21) | |
| Very high | 23.2 (16) | ||
| Vital decisions related to work, % (n) | |||
| Career choice | 0.486 | ||
| Not at all | 56.1 (32) | 38.7 (12) | |
| Slightly | 14 (8) | 19.4 (6) | |
| Moderately | 15.8 (9) | 22.6 (7) | |
| Much | 14 (8) | 19.4 (6) | |
| Job performance | 0.091 | ||
| Not at all | 36.8 (21) | 19.4 (6) | |
| Slightly | 24.6 (14) | 16.1 (5) | |
| Moderately | 17.5 (10) | 38.7 (12) | |
| Much | 21.1 (12) | 25.8 (8) | |
| Promotion opportunities | 0.443 | ||
| Not at all | 64.9 (37) | 48.4 (15) | |
| Slightly | 19.3 (11) | 32.3 (10) | |
| Moderately | 8.8 (5) | 12.9 (4) | |
| Much | 7 (4) | 6.5 (2) | |
| Job absenteeism | 0.467 | ||
| Not at all | 50.9 (29) | 38.7 (12) | |
| Slightly | 26.3 (15) | 22.6 (7) | |
| Moderately | 19.3 (11) | 32.3 (10) | |
| Much | 3.5 (2) | 6.5 (2) | |
| Income and salary | 0.329 | ||
| Not at all | 82.5 (47) | 67.7 (21) | |
| Slightly | 7 (4) | 19.4 (6) | |
| Moderately | 7 (4) | 9.7 (3) | |
| Much | 3.5 (2) | 3.2 (1) | |
| Cause of job loss | 0.137 | ||
| Not at all | 87.7 (50) | 74.2 (23) | |
| Slightly | 7 (4) | 19.4 (6) | |
| Moderately | 1.8 (1) | 6.5 (2) | |
| Much | 3.5 (2) | 0 (0) | |
| Early retirement | 0.344 | ||
| Not at all | 93 (53) | 80.6 (25) | |
| Slightly | 1.8 (1) | 6.5 (2) | |
| Moderately | 3.5 (2) | 6.5 (2) | |
| Much | 1.8 (1) | 6.5 (2) | |
| Vital decisions related to education, % (n) | |||
| Educational performance | 0.86 | ||
| Not at all | 43.9 (29) | 40 (14) | |
| Slightly | 28.8 (19) | 28.6 (10) | |
| Moderately | 13.6 (9) | 20 (7) | |
| Much | 13.6 (9) | 11.4 (4) | |
| Achieving desired educational level | 0.94 | ||
| Not at all | 68.2 (45) | 65.7 (23) | |
| Slightly | 10.6 (7) | 14.3 (5) | |
| Moderately | 13.6 (9) | 14.3 (5) | |
| Much | 7.6 (5) | 5.7 (2) | |
| Impact on personal relationships, % (n) | |||
| Family relationships | 0.051 | ||
| Not at all | 56.5 (39) | 31.4 (11) | |
| Slightly | 18.8 (13) | 22.9 (8) | |
| Moderately | 15.9 (11) | 37.1 (13) | |
| Much | 8.7 (6) | 8.6 (3) | |
| Socializing with friends | 0.002* | ||
| Not at all | 47.8 (33) | 25.7 (9) | |
| Slightly | 26.1 (18) | 25.7 (9) | |
| Moderately | 11.6 (8) | 42.9 (15) | |
| Much | 14.5 (10) | 5.7 (2) | |
| Romantic relationship | 0.015* | ||
| Not at all | 50.7 (35) | 37.1 (13) | |
| Slightly | 30.4 (21) | 14.3 (5) | |
| Moderately | 11.6 (8) | 31.4 (11) | |
| Much | 7.2 (5) | 17.1 (6) | |
| Not having the desired partner | 0.5 | ||
| Not at all | 78.3 (54) | 74.3 (26) | |
| Slightly | 11.6 (8) | 17.1 (6) | |
| Moderately | 5.8 (4) | 8.6 (3) | |
| Much | 4.3 (3) | 0 (0) | |
| Impact on reproductive desire and sexuality, % (n) | |||
| Desire to have children | 0.547 | ||
| Not at all | 85.5 (59) | 74.3 (26) | |
| Slightly | 7.2 (5) | 14.3 (5) | |
| Moderately | 2.9 (2) | 5.7 (2) | |
| Much | 4.3 (3) | 5.7 (2) | |
| Not having children | 0.208 | ||
| Not at all | 93.3 (42) | 80.8 (21) | |
| Slightly | 2.2 (1) | 11.5 (3) | |
| Moderately | 4.4 (2) | 7.7 (2) | |
| Much | 0 (0) | 0 (0) | |
| Not having all desired children | 0.126 | ||
| Not at all | 91.1 (41) | 73.1 (19) | |
| Slightly | 4.4 (2) | 11.5 (3) | |
| Moderately | 4.4 (2) | 15.4 (4) | |
| Much | 0 (0) | 0 (0) | |
| Having sexual problems | 0.012* | ||
| Not at all | 68.1 (47) | 45.7 (16) | |
| Slightly | 18.8 (13) | 20 (7) | |
| Moderately | 11.6 (8) | 17.1 (6) | |
| Much | 1.4 (1) | 17.1 (6) | |
| Impact on housing, % (n) | |||
| Choice of usual housing | 0.398 | ||
| Not at all | 75 (51) | 71.4 (25) | |
| Slightly | 8.8 (6) | 17.1 (6) | |
| Moderately | 11.8 (8) | 11.4 (4) | |
| Much | 4.4 (3) | 0 (0) | |
| Choice of place to live | 0.98 | ||
| Not at all | 75 (51) | 71.4 (25) | |
| Slightly | 11.8 (8) | 14.3 (5) | |
| Moderately | 10.3 (7) | 11.4 (4) | |
| Much | 2.9 (2) | 2.9 (1) | |
| Living abroad | 0.576 | ||
| Not at all | 78.3 (54) | 74.3 (26) | |
| Slightly | 7.2 (5) | 5.7 (2) | |
| Moderately | 8.7 (6) | 17.1 (6) | |
| Much | 5.8 (4) | 2.9 (1) | |
| Impact on holidays and leisure, % (n) | |||
| National holidays and leisure trips | 0.355 | ||
| Not at all | 39.1 (27) | 22.9 (8) | |
| Slightly | 27.5 (19) | 31.4 (11) | |
| Moderately | 21.7 (15) | 25.7 (9) | |
| Much | 11.6 (8) | 20 (7) | |
| International holidays and leisure trips | 0.159 | ||
| Not at all | 56.5 (39) | 34.3 (12) | |
| Slightly | 23.2 (16) | 28.6 (10) | |
| Moderately | 13 (9) | 22.9 (8) | |
| Much | 7.2 (5) | 14.3 (5) | |
| Impact on sports and lifestyle, % (n) | |||
| Changing habits of lifestyle | 0.066 | ||
| Not at all | 31.9 (22) | 22.9 (8) | |
| Slightly | 29 (20) | 11.4 (4) | |
| Moderately | 24.6 (17) | 42.9 (15) | |
| Much | 14.5 (10) | 22.9 (8) | |
| Fashion choices | 0.004* | ||
| Not at all | 36.2 (25) | 20 (7) | |
| Slightly | 21.7 (15) | 5.7 (2) | |
| Moderately | 21.7 (15) | 54.3 (19) | |
| Much | 20.3 (14) | 20 (7) | |
| Sports practice | 0.593 | ||
| Not at all | 44.9 (31) | 31.4 (11) | |
| Slightly | 17.4 (12) | 20 (7) | |
| Moderately | 21.7 (15) | 25.7 (9) | |
| Much | 15.9 (11) | 22.9 (8) | |
| Impact on toxic habits, % (n) | |||
| Smoking | 0.622 | ||
| Not at all | 68 (17) | 61.5 (8) | |
| Slightly | 8 (2) | 0 (0) | |
| Moderately | 16 (4) | 23.1 (3) | |
| Much | 8 (2) | 15.4 (2) | |
| Alcohol | 0.033* | ||
| Not at all | 67.4 (31) | 54.4 (12) | |
| Slightly | 23.9 (11) | 9.1 (2) | |
| Moderately | 6.5 (3) | 22.7 (5) | |
| Much | 2.2 (1) | 13.6 (3) | |
| Anxiolytics, antidepressants, or sleeping pills | 0.804 | ||
| Not at all | 42.9 (15) | 42.1 (8) | |
| Slightly | 17.1 (6) | 21.1 (4) | |
| Moderately | 25.7 (9) | 15.8 (3) | |
| Much | 14.3 (5) | 21.1 (4) | |
| Other drugs | 0.26 | ||
| Not at all | 94.1 (16) | 80 (8) | |
| Slightly | 5.9 (1) | 20 (2) | |
| Moderately | 0 (0) | 0 (0) | |
| Much | 0 (0) | 0 (0) | |
| Impact of symptoms, % (n) | |||
| Pain | 0.038* | ||
| Not at all | 24.6 (17) | 11.4 (4) | |
| Slightly | 26.1 (18) | 25.7 (9) | |
| Moderately | 33.3 (23) | 22.9 (8) | |
| Much | 15.9 (11) | 40 (14) | |
| Itching | 0.001* | ||
| Not at all | 0 (0) | 2.9 (1) | |
| Slightly | 7.2 (5) | 0 (0) | |
| Moderately | 36.2 (25) | 5.7 (2) | |
| Much | 56.5 (39) | 91.4 (32) | |
| Sleep deprivation | 0.021* | ||
| Not at all | 18.8 (13) | 8.6 (3) | |
| Slightly | 29 (20) | 14.3 (5) | |
| Moderately | 27.5 (19) | 22.9 (8) | |
| Much | 24.6 (17) | 54.3 (19) | |
| Fatigue | 0.021* | ||
| Not at all | 49.3 (34) | 20 (7) | |
| Slightly | 29 (20) | 34.3 (12) | |
| Moderately | 15.9 (11) | 34.2 (12) | |
| Much | 5.8 (4) | 11.4 (4) | |
| Shame | 0.004* | ||
| Not at all | 37.7 (26) | 11.4 (4) | |
| Slightly | 31.9 (22) | 22.9 (8) | |
| Moderately | 15.9 (11) | 28.6 (10) | |
| Much | 14.5 (10) | 37.1 (13) | |
| Lack of confidence | 0.004* | ||
| Not at all | 47.8 (33) | 17.1 (6) | |
| Slightly | 30.4 (21) | 28.6 (10) | |
| Moderately | 8.7 (6) | 22.9 (8) | |
| Much | 13 (9) | 31.4 (11) | |
| Stress, anxiety, or mood swings | 0.487 | ||
| Not at all | 24.6 (17) | 17.1 (6) | |
| Slightly | 24.6 (17) | 22.9 (8) | |
| Moderately | 27.5 (19) | 22.9 (8) | |
| Much | 23.2 (16) | 37.1 (13) | |
| Feeling sad | 0.007* | ||
| Not at all | 42 (29) | 14.3 (5) | |
| Slightly | 20.3 (14) | 20 (7) | |
| Moderately | 24.6 (17) | 28.6 (10) | |
| Much | 13 (9) | 37.1 (13) | |
| Quantitative variables are expressed as mean and standard deviation (SD) and categorical variables as relative (%) and absolute frequencies (n). *Statistical significance. | |||
DISCUSSION
AD is a chronic skin disease that has a moderate to severe impact on the life decisions assessed. It specifically influences the way of dressing, lifestyle, sports practice, work performance, holidays and leisure, and all types of relationships (family, social, and sentimental), among others. In addition, it has been shown that more severe AD patients suffer a greater impact on these life decisions.
Furthermore, it has been observed that greater severity of the disease is related to earlier onset, more affected areas, and higher prevalence of other comorbidities such as asthma. An earlier onset of AD may contribute to a deterioration of family relationships, a poorer perception of body image, low self-esteem, psychiatric comorbidities, and may even lead to suicidal behaviour and suicidal ideation (17). In short, greater severity of AD is associated with greater psychological impact. Therefore, just as the quality of life of patients decreases as the severity of the disease increases (18–20), the impact of certain life decisions such as dressing, personal, and sexual relationships was greater the greater the severity of AD.
There is a large body of scientific literature emphasizing the influence of AD on the quality of life of people with AD. Multiple studies underline the negative impact on patients of both their symptoms and their external appearance. This leads to a perception of poorer general health compared with the healthy population, as well as life dissatisfaction and lower scores on mental health questionnaires, particularly anxiety and depression, which, together with lack of sleep, leads to worse functioning in the work environment, social settings, and daily activities (21–25). Moreover, considering the chronic nature of the disease, the negative impact is not only on the patient but also on their family and on couples, with difficulties in their relationships. Indeed, 1 study found that dermatitis patients’ partners had similar results in terms of quality-of-life questionnaires to those of the patients themselves (26).
A recent study that evaluated the impact of psoriasis on life decision-making showed that the most affected aspects were career choice, job performance, dress, and job absenteeism (8). These findings were very similar to those found in this study, which is not surprising considering that both are chronic visible skin diseases. Bhatti et al., who described the concept of MLCD, have developed a questionnaire based on their initial qualitative study. Future studies may benefit from integrating the MLCDP for a more standardized evaluation (7, 9–11). It also would be interesting to incorporate this questionnaire as an additional measure of severity in chronic skin diseases such as AD, psoriasis, or hidradenitis suppurativa. Potential interventions for managing the impact of AD include adopting multidisciplinary approaches that integrate dermatological and psychological care, ensuring comprehensive treatment of both physical and emotional aspects of the disease. Additionally, early intervention programmes could play a crucial role in addressing symptoms promptly, improving emotional well-being, and minimizing the long-term psychosocial effects of AD.
This is the first study to assess the impact of AD on MLCD. However, it has some limitations. First, its cross-sectional design means it lacks follow-up. Second, it is a single-centre study conducted in the AD unit of a third-level hospital, which primarily treats more severe cases and patients under controlled treatment, making it difficult to generalize the findings to those treated in primary care or the general population. Additionally, as volunteers were included, the respondents are likely to be those most aware of their condition.
To conclude, MLCD are significantly impacted in patients with AD, with those experiencing more severe forms of the disease being more affected across a wide range of decisions. Comprehensive management strategies should integrate physical and psychological support to mitigate these impacts. Early intervention may reduce long-term consequences, enhancing quality of life and decision-making capacity in patients with AD. These findings emphasize the need to address the psychosocial burden of AD through patient education and advocacy. Resource allocation should focus on integrating holistic care approaches that target both physical and emotional aspects of the disease. Furthermore, future studies are warranted to validate these results across diverse populations and to develop targeted tools for assessing and addressing MLCD in chronic diseases. In AD patients, it is not just their skin that suffers: the disease extends beyond physical symptoms, affecting emotional, psychological, and social aspects, altering the fabric of their daily lives.
ACKNOWLEDGEMENTS
This research was funded by Instituto de Salud Carlos III (ISCIII) through the project PI23/01875. R.S.d.l.T. was supported by a predoctoral fellowship from Ministry of Universities (FPU21/00833) and T.M.V. was supported by a postdoctoral fellowship from the ISCIII (CM22/00083).
IRB approval status: This study was reviewed and approved by the ethics committee (CEIM Granada).
REFERENCES
- Nutten S. Atopic dermatitis: global epidemiology and risk factors. Ann Nutr Metab 2015; 66: 8–16. https://doi.org/10.1159/000370220
- Montero-Vilchez T, Rodriguez-Pozo J-A, Diaz-Calvillo P, Salazar-Nievas M, Tercedor-Sanchez J, Molina-Leyva A, et al. Dupilumab improves skin barrier function in adults with atopic dermatitis: a prospective observational study. J Clin Med 2022; 11: 3341. https://doi.org/10.3390/jcm11123341
- Ortiz de Frutos FJ, Torrelo A, de Lucas R, González MA, Alomar A, Vera Á, et al. Patient perspectives on triggers, adherence to medical recommendations, and disease control in atopic dermatitis: the DATOP Study. Actas Dermosifiliogr 2014; 105: 487–496. https://doi.org/10.1016/j.ad.2014.01.004
- Bylund S, Kobyletzki L, Svalstedt M, Svensson. Prevalence and incidence of atopic dermatitis: a systematic review. Acta Derm Venereol 2020; 100: adv00160. https://doi.org/10.2340/00015555-3510
- Margolis JS, Abuabara K, Bilker W, Hoffstad O, Margolis DJ. Persistence of mild to moderate atopic dermatitis. JAMA Dermatol 2014; 150: 593–595. https://doi.org/10.1001/jamadermatol.2013.10271
- Ali F, Vyas J, Finlay A. Counting the burden: atopic dermatitis and health-related quality of life. Acta Derm Venereol 2020; 100: adv00161. https://doi.org/10.2340/00015555-3511
- Bhatti Z, Salek M, Finlay A. Chronic diseases influence major life changing decisions: a new domain in quality of life research. J R Soc Med 2011; 104: 241–250. https://doi.org/10.1258/jrsm.2011.110010
- Sanchez-Diaz M, Díaz-Calvillo P, Soto-Moreno A, Molina-Leyva A, Arias-Santiago S. Factors influencing major life-changing decisions in patients with psoriasis: a cross-sectional study. Acta Derm Venereol 2023; 103: adv11640. https://doi.org/10.2340/actadv.v103.11640
- Bhatti ZU, Salek K, Finlay AY. Concept of major life-changing decisions in life course research. In Kimball AB, Linder MD, editors. Basel: Karger, 2013: p. 52–66. https://doi.org/10.1159/000350389
- Bhatti ZU, Finlay AY, Bolton CE, George L, Halcox JP, Jones SM, et al. Chronic disease influences over 40 major life changing decisions (MLCDs): a qualitative study in dermatology and general medicine. J Eur Acad Dermatol Venereol 2014; 28: 1344–1355. https://doi.org/10.1111/jdv.12289
- Bhatti ZU, Salek SS, Bolton CE, George L, Halcox JP, Jones SM, et al. The development and validation of the Major Life Changing Decision Profile (MLCDP). Health Qual Life Outcomes 2013; 11: 78. https://doi.org/10.1186/1477-7525-11-78
- Chopra R, Silverberg JI. Assessing the severity of atopic dermatitis in clinical trials and practice. Clin Dermatol 2018; 36: 606–615. https://doi.org/10.1016/j.clindermatol.2018.05.012
- Reolid A, Servitje O, Ginarte M, Pérez-Ferriols A, Vélez A, Aragües M, et al. Validation of an optical pencil method to estimate the affected body surface area in psoriasis. Actas Dermosifiliogr 2020; 111: 143–148. https://doi.org/10.1016/j.ad.2019.07.002
- Simpson EL, de Bruin-Weller M, Eckert L, Whalley D, Guillemin I, Reaney M, et al. Responder threshold for Patient-Oriented Eczema Measure (POEM) and Children’s Dermatology Life Quality Index (CDLQI) in adolescents with atopic dermatitis. Dermatol Ther (Heidelb) 2019; 9: 799–805. https://doi.org/10.1007/s13555-019-00333-2
- Pariser DM, Simpson EL, Gadkari A, Bieber T, Margolis DJ, Brown M, et al. Evaluating patient-perceived control of atopic dermatitis: design, validation, and scoring of the Atopic Dermatitis Control Tool (ADCT). Curr Med Res Opin 2020; 36: 367–376. https://doi.org/10.1080/03007995.2019.1699516
- Topp CW, Østergaard SD, Søndergaard S, Bech P. The WHO-5 Well-Being Index: a systematic review of the literature. Psychother Psychosom 2015; 84: 167–176. https://doi.org/10.1159/000376585
- Kelly KA, Balogh EA, Kaplan SG, Feldman SR. Skin disease in children: effects on quality of life, stigmatization, bullying, and suicide risk in pediatric acne, atopic dermatitis, and psoriasis patients. Children, 2021; 8: 1057. https://doi.org/10.3390/children8111057
- Haeck IM, ten Berge O, van Velsen SGA, de Bruin-Weller MS, Bruijnzeel-Koomen CAFM, Knol MJ. Moderate correlation between quality of life and disease activity in adult patients with atopic dermatitis. J Eur Acad Dermatol Venereol 2012; 26: 236–241. https://doi.org/10.1111/j.1468-3083.2011.04043.x
- Holm JG, Agner T, Clausen M-L, Thomsen SF. Quality of life and disease severity in patients with atopic dermatitis. J Eur Acad Dermatol Venereol 2016; 30: 1760–1767. https://doi.org/10.1111/jdv.13689
- Kim DH, Li K, Seo SJ, Jo SJ, Yim HW, Kim CM, et al. Quality of life and disease severity are correlated in patients with atopic dermatitis. J Korean Med Sci 2012; 27: 1327. https://doi.org/10.3346/jkms.2012.27.11.1327
- Silverberg JI, Gelfand JM, Margolis DJ, Boguniewicz M, Fonacier L, Grayson MH, et al. Patient burden and quality of life in atopic dermatitis in US adults. Ann Allergy Asthma Immunol 2018; 121: 340–347. https://doi.org/10.1016/j.anai.2018.07.006
- Drucker AM. Atopic dermatitis: burden of illness, quality of life, and associated complications. Allergy Asthma Proc 2017; 38: 3–8. https://doi.org/10.2500/aap.2017.38.4005
- Birdi G, Cooke R, Knibb RC. Impact of atopic dermatitis on quality of life in adults: a systematic review and meta-analysis. Int J Dermatol 2020; 59 434–447. https://doi.org/10.1111/ijd.14763
- Lundin S, Bergström A, Wahlgren CF, Johansson EK, Andersson N, Ballardini N, et al. Living with atopic dermatitis as a young adult in relation to health-related quality of life and healthcare contacts: a population-based study. Acta Derm Venereol 2022; 102: adv00702. https://doi.org/10.2340/actadv.v102.294
- Ferrucci SM, Tavecchio S, Angileri L, Surace T, Berti E, Buoli M. Factors associated with affective symptoms and quality of life in patients with atopic dermatitis. Acta Derm Venereol 2021; 101: adv00590. https://doi.org/10.2340/00015555-3922
- Misery L, Seneschal J, Corgibet F, Halioua B, Marquié A, Merhand S, et al. Impact of atopic dermatitis on patients and their partners. Acta Derm Venereol 2023; 103: adv5285. https://doi.org/10.2340/actadv.v103.5285